
I
NASA CONTRACTOR
REPORT
0
h
PHYSIOLOGIC OBSERVATIONS
ON RACE CAR DRIVERS
by Vincent P, Collins
,, .'.'
Prepared by
&
:.’ .=
::.
.,’ ._
L.1
BAYLOR UNIVERSITY
;!:. -,
‘L.‘ ‘;I
; -’ -, ;
. . _
‘, _ _
Houston, Texas
i I
.;>‘.
? _
. , .,-
A.>
-.
._
,:. ;
t.,.. L.
.
-r or
f
'\ ,, ,'
..
/
I
:,'
,._'
NATIONAL AERONAUTICS AND SPACE ADMINISTRATION . WASHINGTON, D. C.
l
SEPTEMBER 1966
PHYSIOLOGIC OBSERVATIONS ON RACE CAR DRIVERS
By Vincent P. Collins
Distribution of this report is provided in the interest of
information exchange.
Responsibility for the contents
resides in the author or organization that prepared it.
Prepared under Grant No. NsG-‘730 by
BAYLOR UNIVERSITY
Houston, Texas
for
NATIONAL AERONAUTICS AND SPACE ADMINISTRATION
For sole by the Clearinghouse for Federal Scientific and Technical Information
Springfield, Virginia 22151 - Price
$3.00


CONTENTS
Section
INTRODUCTION
...........................
GENERALDESCRIPTIONOFMETHODS EMPLOYED
.............
Histories
...........................
In-Race Recording
.......................
Tilt Table Test
.........................
Blood
Blood
Renal
Vital
DAYTONA
Volumes .........................
Chemistries .......................
Function .........................
Signs and Weights
....................
SPORTS CAR RACES, FEBRUARY
1964 . . . . . . . . . . . . .
GALVESTONSFORTS CARRACE, JULY
1964.
..............
AUSTIN SPORTS CAR RACE, AUGUST
1964
...............
HOUSTON SPORTS CAR RACE, OCTOBER
1964
..............
SUMMARY
.............................
Tilt Table Tests
........................
In-Car Recordings
.......................
Blood and Urine Studies
....................
BloodVolume
..........................
CONCLUSIONS
...........................
Page
1
2
2
2
2
4
6
10
12
13
45
68
92
107
107
110
110
112
113
iii
TABLES
Page
Table
1
2
3
4
7
8
9
10
11
12
13
VOLUNTEER DRIVERS, DRIVING TIME, AND STUDIES PER-
FORMED AT DAYTONA INTERNATIONAL SF!FZDWAY . . . . . . . . .
13
VITAL STATISTICS OF SUBJ-ECTS IN RACE AT DAYTONA . . . . . . .
14
PRE- AND POST-RACE TEMPERATURE, PULSE, AND BLOOD PRES-
SURE READINGS OFDRIVERS INTHEAMERICAN CHALLEfNGE
CUP RACE AT DAYTONA INTERNATIONAL SPEEDWAY . . . . . . . .
17
F!RE- AND POST-RACE TEMPERAtiRE, PULSE, AND BLOOD PRES-
SURE REXDTNGS OF DRIVERS IN THE DAYTONA CONTINENTAL
RACE AT DAYTONA INTERNATIONAL SPEEDWAY . . . . . . . . . .
18
WEIGHT-CHANGE STUDIES CONDUCTED ON DRIVERS AT DAYTONA
INTERNATIONAL SPEEDWAY . . . . . . . . . . . . . . . . . . 20
BLOOD-VOLUME STUDIES CONDUCTED ON DRIVERS lX THE
AMERICAN CHAIJXNGE CUF' RACE AT DAYTONA IXTERNATIONAL
SPEEDWAY . . . . . . . . . . . . . . . . . . . . . . . . . 21
BLOOD-VOLUME STUDIES CONDUCTED ON DRIVERS IN TKE DAY-
TONA CONTIKENTAL R.kCE AT DAYTONA INTERNATIONAL
SPEEDWAY . . . . . . . . . . . . . . . . . . . . . . . . . 22
BLOOD-CHEMSSTRY STUDIES CONDUCTED ON DRIVERS AT
DAYTONA INTERNATIONAL SPEEDWAY . . . . . . . . . . . . . .
23
VITAL STATISTICS OF SUaTECTS IN RACES AT GALVKX'ON,
TEXAS,INl964 . . . . . . . . . . . . . . . . . . . . . . 50
PRE-AND POST-RACE TEMFZRATURE, PULSE, AND BLOOD PRES-
SURE READINGS OF DRIVERS IN THE RACES AT GALVESTON,
TEXAS...........................
51
:
WEIGHT-CHANGE STUDIES CONDUCTED ON DRIVXRS IN THE
GALVESTON RACES IN
1964
. . . . . . . . . . . . . . . . . .
52
BLOOD-CHEMISTRY STUDIES CONDUCTED ON DRIVERS IN THE
RACES AT GALVESTON, TEXAS . . . . . . . . . . . . . . . . .
53
PRE- AND POST-RiCE URINALYSES OF DRIVERS IN THE RACES
ATGALVESTON,TEKAS....................
55
iv

Table
14
15.
16
17
18
19
20
Page
VITAL STATISTICS OF DRIVERS IN SPORTS CAR RACES
AT AUSTIN, TEXAS, IN AUGUST 1964 . . . . . . . . . . .
69
PRE- AND POST-RACE TEWERATURE READINGS OF DRIVERS
IN SPORTS CAR,RACES AT AUSTIN, TEXAS, IN 1964 . . . . . 70
WEIGHT-CHANGE STUDIES CONDUCTED ON DRIVERS IN SPORTS
CAR RACES AT AUSTIN, TEXAS, IN AUGUST
1964
. . . . . .
71
BLOOD-CHEMISTRY STUDIES CONDUCTED ON DRIVERS ;TrJ
SPORTS CAR RACES AT AUSTIN, TEXAS, IN AUGUST 1964 . . .
72
UKCNE VOLUME AND CHEMISTRY STUDIES CONDUCTED ON
DRIVERS IN SPORTS CAR RACES AT AUSTIN,.,TExAS, IN
AUGUST 1964 . . . . . . . . . . . . . . . . . . . . . .
78
VITAL STATISTICS OF SUBJECTS IN RACES AT HOUSTON,
TEXAS, IN
1964
. , . . . . . . . . . . . . . . . . . .
105
BLOOD-CHEMISTRY STUDIES CONDUCTED ON DRIVERS IN THE
RACES AT HOUSTON, TEXAS . . . . . . . . . . . . . . . .
106

F'IGURES
Figure
Page
1
Driving periods, Daytona International Speedway . . . . . . .
15
2
Legends for blood chemistry figures
(a) Daytona Continental Race
.................
25
(b) American Challenge Cup Race
..............
25
3
Blood chemistry, glucose
(a) American Challenge Cup Race
..............
26
(b) Daytona Continental Race
................
26
4
Blood chemistry, CO2 combining power
(a) American Challenge Cup Race . . . . . . . . . . . . . .
26
(b) Daytona Continental Race . . . . . . . . . . . . . . . .
26
5
Blood chemistry, lactic dehydrogenase
(a) American Challenge Cup Race . . . . . . . . . . . . . .
27
(b) Daytona Continental Race . . . . . . . . . . . . . . . .
27
6
Blood chemistry, blood urea nitrogen
(a) American Challenge Cup Race . . . . . . . . . . . . . .
27
(b) Daytona Continental Race . . . . . . . . . . . . . . . .
27
7
Blood chemistry, cholesterol
(a) AmericanChallengeCupRace
..............
28
(b) Daytona Continental Race
................
28
8
Blood chemistries
(a) SGOT, American Challenge Cup Race
........... 29
(b) SGOT, Daytona Continental Race
.............
29
(c) SGPT, American Challenge Cup Race
...........
29
(d) SGPT, Daytona Continental Race
.............
29
9
Pulse rate and blood pressure during tilt-table testing
(Driver A, control test) . . . . . . . . . . . . . . . . .
31
vi

Figure
10
11
12
13
14
15
16
17
18
19
20
21
22
23
Page
Pulse rate and blood pressure during tilt-table testing
(Driver A, post race) . . . . . . . . . . . . . . . . . . .
32
Pulse rate and blood pressure during tilt-table testing
(Driver B, control test) . . . . . . . . . . . . . . . . .
33
Pulse rate and blood pressure during tilt-table testing
(DriverB,postrace)................... 34
Pulse rate and blood pressure during tilt-table testing
(Driver C, post race) . . . . . . . . . . . . . . . . . . .
35
Pulse rate and blood pressure during tilt-table testing
(Driver I, post race) . . . . . . . . . . . . . . . . . . . 36
Pulse rate and blood pressure during tilt-table testing
(Driver F, post race) . . . . . . . . . . . . . . . . . . .
37
Pulse rate and blood pressure during tilt-table testing
(Driver H, post race) . . . . . . . . . . . . . . . . . . .
38
Pulse rate and blood pressure during tilt-table testing
(Driver G, post race) . . . . . . . . . . . . . . . . . . .
39
Pulse rate and blood pressure during tilt-table testing
(DriverJ,postrace)................... 40
Pulse rate and blood pressure during tilt-table testing
(Driver L, post race) . . . . . . . . . . . . . . . . . . .
41
Pulse rate and blood pressure during tilt-table testing
(Driver K, post race) . . . . . . . . . . . . . . . . . . .
42
Pulse rate and blood pressure during tilt-table testing
(DriverE,postrace)................... 43
Pulse rate and blood pressure during tilt-table testing
(DriverD,controltest) . . . . . . . . . . . . . . . . . 44
Legends for blood chemistries,
San Jacinto Regional Race,
Galveston, Texas
(a) July4,1964......................
(b) July
5,1964......................
vii

-
Figure
24
Blood chemistry, glucose, San Jacinto Regional Race
Page
(a) July4,1964
......................
47
(b) Jtiy5,1964
......................
47
25
Blood chemistry,
cholesterol, San Jacinto Regional Race
(a) July4,
1964.
......
;
...............
47
(b) July5, 1964. ............
. ........
47
26
Blood chemistry,
uric acid, San Jacinto Regional Race
(a) ~uly4,l964
......................
(b) JUly5.1964
......................
27
Blood chemistry, creatinine, San Jacinto Regional Race
(a) ~uly4,1964......................
(b) J~iLy5,1964......................
28
Blood chemistry, chlorides, San Jacinto Regional Race
(a) July4,1964......................
(b) July"5,1964. . . . . . . . . . . . . . . . . . . . . .
49
49
29
Blood chemistry, phosphorus,
San Jacinto Regional Race
(a) July 4,
1964
......................
49
(b) July5,lg64
......................
49
Pulse rate and blood pressure during tilt-table testing
(Driver I, pre-race control) . . . . . . . . . . . . . . .
30
31
32
33
34
35
57
Pulse rate and blood pressure during tilt-table testing
(Driver I, post race) . . . . . . . . . . . . . . . . . . .
58
Pulse rate and blood pressure during tilt-table testing
(Driver H, post win) . . . . . . . . . . . . . . . . . . .
59
Pulse rate and blood pressure during tilt-table testing
(Driver H, post race) . . . . . . . . . . . . . . . . . . .
60
Pulse rate and blood pressure during tilt-table testing
(Driver E, post race) . . ; . . . . . . . . . . . . . . . .
61
Pulse rate and blood pressure during tilt-table testing
(Driver B, post win) . . . . . . . . . . . . . . . . . . .
62
viii

Page
Figure
36
37
38
39
40
41
42
43
44
45
46
47
48
49
50
51
Pulse rate and blood pressure during tilt-table testing
(Driver J, post race) . . . . . . . . . . . . . . . . . . .
63
Pulse rate and blood pressure during tilt-table testing
(Driver F, post race) . . . . . . . . . . . . . . . . . . .
64
Pulse rate and blood pressure during tilt-table testing
(Driver D, post race) . . . . . . . . . . . . . . . . . . .
65
Pulse rate history during race (Driver E) . . . . . . . . . .
67
Legends for blood chemistries, Alamo Regional Race, Austin,
Texas, August
16,
1964 . . . . . . . . . . . . . . . . . .
74
Blood chemistry, glucose, Alamo Regional Race,
August
16,
1964. . . . . . . . . . . . . . . . . . . . . .
75
Blood chemistry,
cholesterol, Alamo Regional Race,
August
16,1964. . . . . . . . . . . . . . . . . . . . . .
75
Blood chemistry,
uric acid, Alamo Regional Race,
August16, 1964. . . . . . . . . . . . . . . . . . . . . .
75
Blood chemistry,
creatinine, Alamo Regional Race,
August
16,1964. . . . . . . . . . . . . . . . . . . . . .
75
Blood chemistry, chloridws, Alamo Regional Race,
August16,1g64...................... 76
Blood chemistry, phosphorus, Alamo Regional Race,
August
16, 1964. . . . . . . . . . . . . . . . . . . . . .
76
Pulse rate and blood pressure during tilt-table testing
(Driver B
, post race, without ice-cooled suit) . . . . . .
81
Pulse rate and blood pressure during tilt-table
testing
(Driver B, post race,. with ice-cooled suit) . . . . . . . .
82
Pulse rate and blood pressure during tilt-table testing
(Driver A, post race,
without ice-cooled suit) . . . . . . 83
Pulse rate and blood pressure during tilt-table testing
(Driver A, post race,
with ice-cooled suit) . . . . . . . .
84
Pulse rate and blood pressure during tilt-table testing
(Driver D, post practice) . . . . . . . . . . . . . . . . .
85
ix

Figure
52
Pulse rate and blood pressure during tilt-table testing
(Driver D, post race) . . . . . . . . . . . . . . . . . . .
Page
86
53
Pulse rate and blood pressure during tilt-table testing
(Driver C, post practice) . . . . . . . . . . . . . . . . .
54
Pulse rate and blood pressure during tilt-table testing
(Driver E, pre-race control) . . . . . . . . . . . . . . . .
87
88
55
Pulse rate and body temperature (Driver A, without
ice-cooled suit) . . . . . . . . . . . . . . . . . . . . . .
90
56
Pulse rate and body temperature (Driver A, with
ice-cooled suit) . . . . . . . . . . . . . . . . . . . . .
57
Pulse rate and blood pressure during tilt-table testing
(Driver A, post race) . . . . . . . . . . . . . . . . . . .
91
94
58
Pulse rate and blood pressure during tilt-table testing
(Driver C, post race) . . . . . . . . . . . . . . . . . . .
59
Pulse rate and blood pressure during tilt-table testing
(Driver B
,postrace)...................
Pulse rate and blood pressure during tilt-table testing
(Driver D,,post race) . . . . . . . . . . . . . . . . . . .
95
96
60
61
Pulse rate and blood pressure during tilt-table testing
(Driver E, pre-race control) . . . . . . . . . . . . . . .
97
98
62
Pulse rate and blood pressure during tilt-table testing
(Driver E, pre-race control) . . . . . . . . . . . . . . .
63
Pulse rate and blood pressure during tilt-table testing
(Driver E, post race) . . . . . . . . . . . . . . . . . . .
64
Pulse rate and blood pressure during tilt-table testing
(Driver F, control test) . . . . . . . . . . . . . . . . .
65
Pulse rate and blood pressure during tilt-table testing
(Driver F, post race) . . . . . . . . . . . . . . . . . . .
99
100
101
102
66
Pulse rate history during race (Driver E) . . . . . . . . . .
104
X

PHYSIOLOGIC OBSERVATIONS ON RACE CAR DRIVERS*
Project Coordinator:
Vincent P. Collins, M.D.,
Professor of Radiology
INTRODUCTION
Performance under conditions of stress is the essence of athletic
activities. These are commonly carried out by individuals equipped with
certain physical advantages augmented by special training of varying de-
grees of intensity. Athletic contests provide a testing ground where
performance is an index of ability and preparation.
Many daily activities and occupations
--driving on city streets and
highways, piloting commercial planes or manning spacecraft--involve per-
formance where error could endanger lives of individuals or projects of
great national importance.
In these activities, too, natural ability and
preparation are elements in performance that become increasingly important
where public welfare and safety are involved.
Educational and training programs for a wide variety of occupations
provide reasonable competence to cope with normal circumstances.
Rner-
gency
situations involving physical danger are more difficult to study
because simulated testing necessarily lacks the ingredient of genuine
danger and its effect upon emotion and performance.
One sports activity which provides an opportunity for a study of indi-
vidual performance under conditions of non-simulated stress is auto rac-
ing. This is the subject of this investigation.
The underlying concept of the study is that environmental stimuli
produce physiological and biochemical responses within the individual
which govern the effectiveness and efficiency of his reaction.
There are
therefore two stages of investigation: the first is to identify and clas-
sify the range of physiological and biochemical responses; the second is
to relate these to performance. This study deals with the first stage.
Observations were carried out at four
auto
races which will be reported
individually.
This was augmented, when possible, by control studies in
the radiology department at Baylor University College of Medicine.
*From Department of Radiology, Baylor University College of Medicine,
Houston, Texas.

GENERAL DESCRIPTION OF METHODS EMPLOYED
Histories
A complete history of each driver was obtained. A copy of the his-
tory format is contained in the report.
Information pertaining to the
drivers' vital statistics, medical history, occupation, hobbies, and ex-
perience in racing was obtained. Additional information as to the amount
of rest received prior to driving,
food intake, or any other information
giving a better understanding of factors which may influence performance,
was recorded.
In-Race Recording
Continuous monitoring of the transthoracic and sternal lead ECG, oral
temperature, and respiration were recorded during the race.
Four drivers
were monitored simultaneously, two by telemetry and two by in-car tape
recorders.
A lap-by-lap description of the race
, giving position of monitored
drivers and performance, was recorded on a tape recorder.
Additional
spotters were deployed at strategic positions around the track to assist
in following the progress of the drivers.
As each driver passed these
observation points, the information was relayed to the monitoring station
and pit area by radio communication.
Tilt Table Test
Performance, and even existence, depend upon a precise maintenance
of cerebral blood supply which hence becomes the first function of the
circulatory system. The efficiency of the intricate reflexes involved is
a likely index of the stress to which physiological mechanisms are sub-
jected in maintaining an even blood flow to the brain while meeting the
requirements of violent physical exertion, emotional responses, energy
utilization, and heat exchange.
The tilt table test provides a simple record of cardiovascular reflex
response to the altered dynamics of circulation required by a sudden
change in the hydrostatic pressures in tilting the body from horizontal
to vertical and back to horizontal.
In the recumbent position, the heart must circulate blood in a sys-
tem less than 12 inches in vertical height against a resistance in the
peripheral vascular bed of extremities and splanchnic areas that must be
in balance with the resistance in the cerebral circulation on the same
level.
On tilting to the erect position,
the heart must now pump blood to
the brain at a height of 5 to 6 feet. There is a column of blood of this
height offering a hydrostatic pressure which the dependent peripheral
2

vascular bed must resist to avoid dilatation and pooling.
The correction
must provide unfaltering cerebral blood flow while meeting and coordinat-
ing all circulatory demands for other parts and functions of the body.
In a rigid closed system, the demand upon the circulatory pump would
be simplified by unchanging volume and distribution.
In the elastic
closed system of the human circulatory system, complex interlocking re-
flexes are involved.
There are two mechanisms for maintaining cerebral circulation on
tilting up to the erect position: (1) The vasomotor reflex which in-
creases peripheral resistance in order to maintain or increase the dia-
stolic pressure (2) The cardiac output which increases in order to
maintain systolic pressure by an increase in pulse rate and/or an increase
in stroke volume.
One might expect stress to be reflected in alterations of either or
both of these mechanisms.
The tilt table test utilizes a basket stretcher that can be tilted
up to TO0 with a smooth and rapid motion. The only support is the con-
tour of the stretcher and the 'foot-plate; restraining bands are avoided
because of possible influence on circulation. During the test a contin-
uous recording is made of blood pressure, ECG, cardiotach, and pneumogram.
There are three phases:
(1)
a pre-tilt recording in the recumbent posi-
I;:? (2)
a recording with the subject in orthostatic position (70') and
a post-tilt recording in the recumbent position.
A minimum of 5 min-
utes of recording in each position is obtained unless the individual shows
syncope in the erect position.
Systolic pressure is the result of ejection of blood by the heart.
The factors will be the rate of ejection, the amount ejected, and the
residual pressure in the great vessels. Heart rate and duration of sys-
tale are readily determined. In this study stroke volume can only be
inferred.
In the erect position, diastolic pressure would fall if blood were to
drain away or pool in dependent vascular beds under the effect of increased
hydrostatic pressure. This is opposed by a nicely timed vasomotor reflex
to contract the dependent capillary bed and increase the peripheral re-
sistance by a precise degree which must vary as the hydrostatic pressure
at different vertical heights within the circulatory tree.
It is also
opposed by an increased cardiac output to meet the demand of an increased
blood flow through the dependent vascular bed.
Diastolic pressure changes
then are assumed to reflect the vasomotor response, primarily but not
entirely.
Pulse pressure is the difference between systolic and diastolic pres-
sure. This is primarily a function of cardiac output.
If vasomotor pro-
tection of diastolic pressure is good,
then cardiac.output is principally
utilized to maintain systolic pressure,
and pulse pressure may be wide.
3

If vasomotor protection of diastolic pressure is poor, then an in-
creased cardiac output may maintain diastolic pressure, at least tempo-
rarily.
However, this is at the expense of maintenance of systolic
pressure and pulse pressure which tend to fall.
A narrow pulse pressure
will generally indicate a diminished blood flow to all areas and, if it is
not 'corrected, syncope may follow.
Blood Volumes
Iodinated human serum albumin tagged with
I
131
has been employed for
several years in the determination of blood volumes.
The basic principle
of measurement is the introduction of a known quantity of a radioisotope
tracer and measuring its distribution and dilution according to formula:
where
Cl = concentration of isotope/ml injected.
Vl = number ml injected.
C2 = concentration of dilutent/ml.
V2 = volume of dilutent/ml.
Standard technique of blood volume determination has a small techni-
cal error of +2 percent S.E.
and is suitable for clinical use.
Certain
modifications used by this institution further minimize this error.
Laboratory studies to determine blood volumes during the passive tilt
study indicate changes in the estimated total volume of blood, plasma
volume,
red cell mass, and the ratio of red cell mass to total volume
(hematocrit).
This can be interpreted as a decrease in effective volume
during the tilt.
These changes become more pronounced after exercise.
The drivers were placed in a supine position in a Stokes stretcher
and the physiograph electrode applied.
At this time,
10 ml (approx. 20 WC>
iodinated human serum albumin is injected.
A sample of blood is withdrawn
at the end of 10 minutes (equilibrium takes 6 to 8 minutes).
The driver
is immediately raised to TO0
and retained in this position for 8 minutes,
at which time another sample is obtained.
He is then returned to the
supine position.
Previous studies have indicated that during tilt there is a certain
amount of pooling of whole blood and/or plasma in the extremities.
The
impression is that the effective volume is decreased by pooling whole
blood in the vascular space and the total volume decreases by the loss of
plasma water to the tissue space.
4

Returning to horizontal position,
the vascular pooled blood returns
to circulation rapidly but there is a delay in the return of the tissue
pooled water.
The more plasma water pooled in the tissue space the slower
the return to normal.
An attempt was made to measure the plasma water loss during tilt, and
the relation to cardiovascular response.
Results of the study are presented in tables 6 and 7.
Because of
some doubt as to the volume measured by iodinated human serum albumin di-
lution technique, the results are presented as normalized volumes related
to the isotope concentration in the lo-minute whole blood sample. As
equilibrium is reached by 6 to 8 minutes,.the lo-minute whole blood deter-
mination represents a volume of 100.
Therefore, the basicdilution equa-
tion is now written:
'B,t =
‘B,lO (loo>’
'B,t
where V
B,t
= volume of whole blood at time t.
C
B,lO
= counts in whole blood at 10 min.
'B,t
= counts in whole blood at time t.
The plasma volume at 10 minutes is:
v
p,lO =
‘B,JO (loo)
c
P,lO
where V
P,lO
= plasma volume at 10 min.
C
P,lO
= counts in plasma at 10 min.
The plasma volume at time t is:
V
- %t
P,t Cp t x 'B,t
>
where, C
p,t
= counts in plasma at time t.
(1)
(31
The red cell mass at any time can be determined by subtracting the
plasma volume from the whole blood volume at that time.
The hematocrit
is the ratio of the red cell mass at any given time to the whole blood
volume at the same time.
5

In tables 6 and 7, the changes from the value at 10 minutes are given
in the column headed AV, or for the hematocrit A.
The predominant change is towarda decreased circulating whole blood
volume while in tilt. Right of the twelve drivers tested responded in
this manner.
Two were excluded from the analysis because of development
of syncope. The other two drivers responded by an increased circulating
blood volume. Analysis indicates this is due to an increase in red cells
with little or no change in plasma.
The decrease in whole blood is al-
most exclusively due to loss in plasma.
Only one individual responded
with a significant decrease in red cells.
This was Driver L, whose hema-
tocrit (53.9 percent) indicated marked dehydration. He is also the driver
who lost the most weight and recorded the highest body temperature while
driving.
It is interesting to note that the change in whole blood volume is
a manifestation of predominant changes in either plasma or red cells, but
never both to the same degree.
The direction of change in one is indepen-
dent of the direction of change in the other. Regardless of which com-
ponent of blood changed, the net result was an increase in hematocrit
except in the one individual who showed indications of marked dehydration.
No relation between the increased whole blood volume and cardiovas-
cular response in tilt could be drawn with this limited number of studies.
Blood Chemistries
The notable changes in blood chemistries are in the values for glu-
cose, CO2 combining power,
and lactic acid dehydrogenase. These and other
metabolites and products recorded, fall within the following scheme for
energy production from stores of carbohydrates, proteins, and fats.
During periods of high energy requirements, the metabolic activity
associated with the conversion of stored metabolites to energy-yielding
compounds and the relation to the biochemicals studied, can be summarized
as :
Carbohydrates
Proteins
Fats
Lactic acid
r
L N-B --m-w
Citric acid 1
I
cycle
L-- --mm-
3
J
co2
+ H20
Cholesterol
(Lactic acid and CO2 are indirectly measured by the CO2 combining power.)
6

The follo&.ng blood chemistries were obtained when possible: glu-
cose, CO2 combining power,
cholesterol, SGOT, SGPT, LDH, BUN, uric acid,
creatinine, and chlorides.
These are normal constituents of the blood
which may show changes in concentration during exercise, as each is in-
volved in the various pathways of metabolic production of muscular energy.
A discussion is given in the following paragraphs on each of the chemis-
tries studied.
Glucose.- In short periods of exercise,, the glucose concentration in
the blood may reach 200 mg percent.
This early rise in glucose may be a
response to a release of adrenalin. Continuance of the exercise may use
up the carbohydrate stores more rapidly than they are formed, resulting
in a decrease in glucose concentration to subnormal levels. It has been
suggested that lactic acid, formed during muscular activity, can stimu-
late the production of glucose by the liver from the metabolite stores.
This may represent the stimulus for glucose production during prolonged
exercise.
CO2 combining power.- CO2 combining power may be changed by the lac-
tic acid liberated into the blood during muscular metabolism. In the
blood, lactic acid is buffered by bicarbonate with the formation of car-
bonic acid.
This bicarbonate;which is tied up with lactic acid, is re-
moved from the role of a buffer for CO2 in the blood. This loss of CO2
buffering may result in a decreased transport of CO2 from the tissue.
Acidosis can ensue if this situation becomes critical. Measurement of
the buffering capacity of the blood can be determined by the CO2
COM-
bining power. In severe exercise, the amount of CO2 which can combine
with the serum should decrease.
Cholesterol.- Cholesterol? as mentioned, carbohydrates, fatty acids,
and amino acids are utilized in the formation of glucose by the liver.
Calorie-rich lipids, after having first been changed to the more active
acetate in the liver, may be used to supply energy to areas of high meta-
bolic activity, such as muscles during exercise. This active acetate is
also an intermediate in the formation of cholesterol during periods of
normal muscular activity. Cholesterol is not utilized in the formation
of energy but is an alternate metabolic pathway for the high-energy com-
pound active acetate. If the metabolic pathway for the active acetate
is shunted toward meeting high energy requirements, then the rate of
cholesterol synthesis should decrease.
Serum glutsmic oxaloacetate transaminase (SGOT) and serum glutsmic
pyruvate transaminase (SGFT).- During tissue respiration certain protein
and carbohydrate intermediates are rapidly converted to the keto-acid by
transamination. Pyruvate, oxaloacetate, and alphaketoglutarate are

intermediates in the citric acid cycle;
The interaction is illustrated in
the following diagram.
Urea cycle - WAspartate Oxaloacetate -Citric acid cycle
+A-ketoglutarate
nGlutamate
Glycine
--* Alanine=Pyruvate
--
-Citric acid cycle
These compounds,
or the enzyme systems necessary for their metabolism,
may change their concentration in the blood under the requirements of pro-
longed exercise. Changes in the glutsmic-oxaloacetic and glutsmic-pyruvate
transaminase were followed during the driving stress.
Lactic dehydrogenase (LDH).-
Lactic acid is formed by the muscular
activity of contraction;
The lactic acid thus formed is broken down to
CO2 and water in the presence of oxygen.
Muscles do not require the im-
mediate availability of oxygen to contract.
Energy can be obtained from
glycogen during the formation of lactic acid without oxygen.
In the ab-
sence of oxygen, pyruvic acid is reduced to lactic acid and energy by the
enzyme lactic dehydrogenase.
During strenuous exercise, lactic acid may
be formed more rapidly than the oxygen becomes available or the lactic
acid can be converted back to the glycogen stores.
This increase in lac-
tic acid formation may result in an increased lactic dehydrogenase concen-
tration in the blood.
Blood urea nitrogen (BUN).-
Urea nitrogen proteins are not completely
oxidized in the body.
Partial oxidation occurs with about 40 percent of
the available energy being excreted as urea.
This energy does not become
available because urea is not oxidized.
Ordinary exercise does not increase the excretion of nitrogen in the
urine nor does it increase the concentration of non-protein nitrogen in
the blood.
As the work becomes strenuous and prolonged, an increased con-
centration of non-protein nitrogen is found in the blood, associated with
an increased excretion in the urine.
The major portion of the non-protein
nitrogen of the blood is in the form of urea.
Retention of urea should be
further increased by the low urine flow on a hot day when water loss by
perspiration is high.
Creatinine.- Creatine,
or some complex body containing creatine, that
is,
creatine phosphate,
is believed the precursor of the waste product
creatinine which is the easiest of the nitrogenous waste products to be
eliminated by the kidneys.
Creatinine is excreted by the kidneys with no
reabsorption; therefore, the plasma concentration is only a function of
production and simultaneous filtration rate.
The reaction of phosphocreatine resulting in the transfer of phosphate
to some acceptor does not yield creatinine directly.
Therefore, the con-
centration of creatinine is not related to muscular acitivity but under
8

normal conditions it has been found to be more closely related to muscle
mass.
The concentration is possibly.related to a constant synthesis of
new creatine with degradation of that replaced to the waste product cre-
atinine.
Since production of creatinine is not related to muscular activity,
change in concentration with no change in muscle mass becomes a function
of the filtration rate in the kidneys.
Any physiological event which causes a hindrance to the flow of urine
may result in an increased creatinine concentration in the serum. Dehy-
dration of the blood, caused by loss of body fluids, should be accompanied
by an increase in blood creatinine. This
is
partly due to concentration
per se, but primarily by impairment of renal circulation from a decrease
in the effective renal plasma flow.
Fhosphorus.-
The physiological utilization of carbohydrates causes a
decrease in serum phosphorus due to phosphorylation.
Urinary pH regularly decreases toward acid levels during and follow-
ing exercise.
This is a direct effort of the body to get rid of hydrogen
ions, preserve its base as far as possible, and maintain the normal pH. An
increased elimination of phosphate is one of the first events. Although
the pH of urine changes only slightly during exercise, it decreases steeply
to low levels within only a few minutes after completion of exercise.
Uric acid.- Uric acid is a weak dibasic acid which is an end product
of purine metabolism. The sources of uric acid can be "endogenous," that
derived from internal tissue metabolism, or "exogenous," which is due to
ingestion of a purine diet.
Ingestion of large amounts of purine-yielding foods normally has very
little effect upon the blood uric acid, as it is excreted rapidly, or up to
20 percent may be destroyed by the body rather than excreted. Of the ni-
trogenous compounds, uric acid is least readily excreted, in that any con-
dition leading to suppression of urinary secretion would be reflected fast
in an increased blood uric acid.
Therefore increases may be due to:
(1) Diminished excretion of uric acid.
(2) Increased production.
(3) Diminished destruction.
Violent exercise raises the concentration slightly, about 1 mg per-
cent , probably due to diminished excretion. A decrease in the uric acid
level of the blood is stated to almost never occur.
Chloride.-
The chloride anions play an essential part in the buffer-
ing action of the plasma by means of the chloride shift. If the CO2
9

tension is raised in the whole blood, the chloride of the plasma decreases,
the chloride of the corpuscle increases,
and the bicarbonate of the plas- -
ma increases.
The chloride anions, which are released by the sodium during
the formation of bicarbonate, migrate into the cells, causing a decrease
in the chloride concentration of the plasma.
This chloride shift may be balanced or overcompensated for by a rapid
decrease in sodium chloride excretion, which occurs during and after mod-
erately severe and severe exercise. This decreased excretion returns to
normal gradually after exercise, often requiring an hour or more. The ex-
cretion ratio of chlorides may decrease to l/5 that of normal.
Loss of fluid and loss of salt generally accompany each other, also
leading to a retention of chloride.
If the loss of fluid is greater than
the ability of the kidney to retain the chlorides, as in prolonged and
profound sweating, weakness, fatigue, lack of appetite, nausea, a dimi-
nution of mental activity, and impairment of renal function can ensue.
Renal Function
Many of the changes in plasma constituents center around kidney func-
tion either' in part or entirety.
The effective renal plasma flow (ERPF) is normally decreased during
and for about 1 hour after exercise.
The degree and rate of decrease,
-- ..-._
as well as the duration,
is possibly a function of the degree of exhaustion
or taxation of the individual. If the exercise is exhausting, the ERPF
may decrease to l/3 the resting rate. Simultaneously, the glomerular fil-
tration rate (GFR) decreases,
but less than the ERPF.
Consequently, the
ratio of amount of plasma which is presented to the glomerular cells and
that filtered per unit time rises.
The plasma concentration of a substance which is filtered and excreted
becomes a function of rate of production, plasma flow, and glomerularfil-
tration rate.
For substances which may be reabsorbed, as in the case of
glucose, reabsorption rate is another function to consider.
The maximum output of any material by the kidney can be defined as
the point where the amount of material filtered minus the amount appearing
in the urine per minute does not change with increasing concentration. A
substance which is filtered and excreted with no reabsorption (such as
creatinine) has a maximum output equal to the maximum filtration rate.
The output at any time would be equal to the plasma concentration times the
simultaneous filtration rate. The maximum output for other substances,
such as glucose,
appear to be more closely governed by the maximum reab-
sorption rate.
Vasomotor disturbances accompanying excitement, digestion, and mus-
cular activity may have marked effects on urine flow by the rate at which
plasma is presented to the cell for filtration. Post-exercise urine flow
returns to approximately normal about 8 minutes after stopping exercise.
10

There is contradictory evidence pointing toward the roles ERPF, GFR,
and reabsorption have on the effectiveness of urinary output under stress.
The major adjustment of renal function must be primarily by the effective
renal plasma flow and tubular reabsorption.
Urine chemistries obtained included glucose, acetone, sodium, potas-
sium, and osmolality when possible.
Glucose (urine).- For glucose,
there appears to be a reabsorption
maximum.
At high plasma concentrations, the rate of reabsorption becomes
fixed. Under normal filtration rates (100 to 125 ml/min), the threshold
concentration in the blood is approximately 160 mg percent. Above this,
the excess is "spilled" into the urine for elimination. The maximum re-
absorption for glucose under these conditions appears to be about 160
to 200 mg/min. Individual variations may occur.
The filtration rate may decrease significantly under conditions of
exhausting exercise.
Assuming a decrease to 60 ml/min and no change in
rate of reabsorption, the blood concentration of glucose would have to
approach 270 mg percent before any sugars would be spilled into the urine.
Potassium (urine).- In mild exercise , potassium excretion either does
not change or decreases slightly with rapid recovery afterward. A reason-
able explanation of a decrease may be a diminished supply of sodium ions
to the potassium-secreting segment of the nephrons.
Potassium is only
partially
reabsorbed by the tubules; the rest is excreted.
Increased uri-
nary output may be related to impaired reabsorption of potassium due to a
preference for the sodium ion.
Additional increase may be due to the pro-
duction of highly concentrated urine.
Sodium (urine).-
A decrease in glomerular filtration rate is a suf-
ficient cause for a decrease in sodium chloride excretion. This, along
with an apparent increase in sodium reabsorption in an attempt to con-
serve the bases of the blood, would make any decrease more apparent. The
excretion of sodium after exercise follows very closely that of chloride
excretion previously mentioned in the discussion of the blood chemistries.
Osmolality (urine).- The measure of the osmolar concentration of a
solute in a fluid is termed osmolality. The capacity of solutes to re-
duce the molar concentration of water is dependent on number, not kind, of
solute particles. In effect, the solute particles displace or dilute the
water molecules,
reducing the escaping tendency of the water from solu-
tion.
The capacity of solutes to influence this colligative property is
expressed in osmols or milliosmols.
One mol of a substance that does not ionize or dissociate when dis-
solved in water is defined as an osmol. One osmol of an undissociated
solute is therefore equal to its molecular weight. Where dissociation
enters the picture, the osmol is something less than the molecular weight,
depending on the number of particles into which the molecule is disso-
ciated at the molar concentration.
11

The molar
concentration of particles in solution can be calculated
from the freezing point of solution using the equation:
t=KxM
where t = freezing point of solution.
K =.cryoscopic constant of water.
M = dissolved particle concentration.
The dissolved particle concentration is expressed as mols per kilo-
gram of water (osmols). The normal range for plasma is 300 to 500 milli-
mols per kg of water while urine may vary from 500 to 1350. Concentrated
urine may reach values as high as 2700 millimols.
The higher the osmolality the more concentrated the solutes, which may
be interpreted as meaning the more the body is conserving H20, or the
more
solutes being excreted.
Vital Signs and Weights
Heart rate, blood pressure, respiration rate, temperature, and weight
were taken, as feasible, before and after control studies and stress events,
and, when possible, during the stress event.
Manually counted radial pulse
rate is of limited value since the change in pulse rate during the cus-
tomary 15-second counting period may be great. Cardiotachometry is of
much greater value, but of course requires application of electrodes and
a paper or tape recorder. This is part of the tilt table test and of in-
race recordings. Isolated blood pressure readings are also of limited
value because of change and human error.
The same is true for respiration
rate manually or visually counted and the impedance pneumogram has been of
little value during violent physical motions.
Oral temperature readings
are dependable if carefully taken; but, under conditions of stress, subjects
may breathe with open mouth, drink cold fluids,
or succumb to nausea and
vomiting. The oral thermistor is satisfactory for constant recording with
a trained subject, but some subjects lose the device or chew it destruc-
tively under excitement of the race.
These signs, therefore, are of limited value under field research con-
ditions.
Weights were all recorded as stripped weight before and after active
competition,
with the minimum possible delay.
12

TABLE l.- VOLUNTEER DRIVERS, DRIVING,TIME, AND STUDIES" PERFORMED
Driver
Driver
Driver
Driver
Driver
Driver
Driver
Driver
- -
~. . . . ..-
AT DAYTONA INTERNATIONAL SPEEDWAY
-
Subject
Elapsed time
DriverA...............
DriverB...............
Driver C . .
. . . . .
DriverD...............
Daytona Continental Race
...............
...............
........
i ......
...............
...............
...............
...............
...............
3 hr 51 min
10 hr 30 min
8 hr 25 min
8 hr 25 min
13 hr 00 min
10 hr 45 min
9 hr 45 min
9 hr 45 min
"Studies performed:
Glucose, BUN, CO2 combining power, cholesterol,
SGOT, SGPT, LDH.
Steroid excretion in urine.
Blood volumes.
Passive tilt.
Body temperature, blood pressure, pulse rate,
weight loss.
Telemetry on in-car recording of ECG, respiration,
temperature.
13

TABLE 2.- VITAL STATISTICS OF SUBJEC,TS IN RACE AT DAYTONA
Driver
Driver A
Driver B
Driver C
Driver D
Driver E
Driver F
Driver G
Driver H
Driver I
Driver J
Driver K
Driver L
Physical description
T
Weight
148
215
166
194
166
175
180
230
1.87
190
140
145
Height
Age
5 ft
5 ft 2 in.
5 ft
5f-t
5
ft 10 l/2 in
6 ft 2 in.
5
ft 10 l/2 in
6 ft 3
in.
5
ft
9
in.
6 ft 2
in.
5
ft 10 l/2 in
5
ft 9 in.
27
44
Cattle
rancher
Car dealer
No
5
yr college
Sports
Yes
2 children
37
34
36
Lumberman
Radio
announcer
Ship repair
industrialist
Yes
3
chi
No
No
35
Race driver
Yes
1 child
38
Auto salesman
Yes
4 children
27
36
Real estate
broker
Industrial
caterer
Race driver
No Sports
Yes
2 children
32
Yes
4 children
26
Race driver
Yes
2 children
41
Auto dealer
Yes
2 children
Occupation
-
arital status
and
o. of children
ldren
T
Education
None after
high school
Training
Industrial
training and
economics
Degree in metal-
lurgy and indus,
design
3
yr college
Racing ex
Type
Sports
7
8
Sports
8
Sports
3
Drag
14
Sports
14
Sports 12
Sports
8
Sports
9
6
Sports
Stocks,
Grand Prix,
Ind.
Sports
8
5
Sports
4
11
rience
No. of
years
Rest prior
to race
1 l/2 hr
rest
7 hr
sleep
9
hr
sleep
7 hr
sleep
6
hr
sleep
8
hr
sleep
7 hr
sleep

Daytona Continental Race
I
I
FFZferen
L
9
I 10
-F
3
car
t”
*
*
‘L
I *
AZ
*
11
7*
1
1’
12
13
--T
L
Legenh
Period of driving
* Post driving studies
# Drove different car - no record of periods of driving
Figure l.-
Driving periods, Daytona International Speedway.

Pre- and post-race temperature, pulse, and blood.pressure (tables 3
and 4).-
These factors are expected to vary in response to environmental
conditions, physical exertion, and emotional stress.
The values in these tables
are
obtained before and after each race
and do not reveal in-race changes which were recorded by telemetry and
in-car recorders. The ambient temperature during the first race on Feb-
ruary 14, 1964, was 75’.; during the second race on February 15, 1964, the
ambient temperature varied from 65O to 78O. The temperature, pulse, and
blood pressure of drivers have been of interest chiefly in mid-summer events
when ambient temperatures of over 105',
cockpit temperatures of over 130°,
closed cars, and flame-proof driving suits may contribute to stress. In
the Daytona events,
climatic conditions were ideal.
No impressive changes
occurred, but this event offers a baseline for comparison with later events
under more severe conditions.
In Race 1, of 2 l/2 hours duration, the variations for all four
drivers in temperature, pulse, and blood pressure are within limits for
common occupational limits.
In Race 2, of 13 hours duration, with two drivers to relieve each
other, Driver L showed a temperature rise from 98.4' to 103.4O F. This
was in a closed car with an outside temperature of 75'. There was no
associated malaise or evident impairment of performance. It raises a
question for future consideration as to a possible variation in efficiency
of body cooling as between individuals.
The co-driver (Driver K) had a
temperature rise from 98.8' to 101' F.
One other driver (F), in an
open car, showed a temperature rise from 97.8' to 101.0' F.
Blood pressures and pulse rates, pre- and post-race, are not inform-
ative for the participants in these events. Monitoring of blood pressure
and pulse rate during tilt table testing is discussed separately.
Monitor-
ing of pulse and temperature during the race are on records in the pos-
session of NASA personnel.
16

TABLE 3.-
PRE- AND POST-RACE TEMPERATURE, PULSE, AND BLOOD PRESSURE READINGS .OF DRIVERS IN THE
AMERICAN CHALLENGE CUP RACE AT DAYTONA INTERNATIONAL SPEEDWAY
Time
Temperature, -OF Blood pressure
Pulse rate
Driver
Pre-race Post-race Pre-race
Post-race Pre-race
Post-race
be-race
Post-race
Driver A 11:30 3:40 99.8 100.2 ‘108/70 120/70 112 108
Driver B 11:40 3:55 100.4 100.0 140/90 115/86 112 107
Driver C 11:20 4:20 99.7 100.0 110/80 115/85 112 112
1 1
Driver.D 1O:lO 4:20 98.2 - 110/70 100/80 88 112
&88/70
'a1o2
'Blood pressure and pulse rate taken after development of syncope.

TABLE 4.-
PRE- AND POST-RACE TEMPERATURE, PULSE, AND BLOOD PRESSURE READINGS.OF DRIVERS
IN THE DAYTONA CONTINENTAL RACE AT DAYTONA INTERNATIONAL SPEEDWAY
-
1
3river
D:
river E
Dl
river F
Ck
ianged
car
river G
DI
river H
river I
river J
Dl
Dl
Dl
DI
D1
-
river K
5ver L
Place
(a)
H
P
H
H
H
P
P
H
H
H
P
H
H
P
H
H
P
P
H
H
P
P
H
H
P
H
H
P
P
H
Time
Temperature,
OF
9:20
1:50
2:35
3:15
99.2
100.5
8:45
.1:50
2:30
2:35
97.8
100.2
101.0
8:30
98.0
8:45
98.6
2~16
99.2
6:35
99.2
8~20
98.2
2~50
98.0
6:40
98.4
8:35
99.4
1:40
100.2
2:54
99.6
l:oo
99.2
0:30 98.0
1:24
98.5
4:38
98.0
8:55
97.8
0:20
98.8
2:15
101.0
7:45
99.1
g:oo 98.4
2:oo 101.7
3:50
103.4
7:45
97.8
Blood pressure
Pulse rate
Weight
118/58
72
166
164
118/68
72
112180
60
175
122/68
92
140/70
96
110/72 84
110/80
84
118/60
96
130190
112
172.5
172
180
179
229.5
228
188
113/66 82
187
120/70
60
187.5
130/85
88
184.5
120/80
80
136.5
110/85
100
134.5
140/76
80
147
135/70
100
141
?H - Hospital (testing area).
P - Pit area.
18

Weight-change studies conducted on drivers at Daytona International
Speedway (table 5>.-
Table 5 indicates a maximum weight loss of 6 lb or
4.1 percent of initial body weight by one driver (L) in a closed car during
Race'2.
Two drivers in open cars during Race 1 lost 4.5 lb or 2.1 per-
cent (B) and 2.3 percent
(D).
Remaining drivers lost 1 to 3 lb but, since
fluid intake was not controlled, the values are not particularly informative.
However, it does suggest that,
under more stressful conditions, more impres-
sive values might be encountered with commensurate changes in blood chemis-
tries.
Rlood volume-and hematocrit (tables 6aand 7).- When blood volume and
hematocrit are recorded as single numerical volumes, some reliance is mer-
ited for purposes of blood replacement in bed patients.
However, the dy-
namics of circulation and fluid exchange across capillary membranes under
conditions of physical activity and stress, transform blood volume and
hematocrit into less tangible concepts.
The variables that determine vol-
ume of the closed circulation at any time are contraction or expansion of
capillary bed, the possibility of reservoirs not constantly in equilibrium
with the general circulation, dilatation and pooling in a dependent cap-
illary bed,
movement of fluid in either direction across capillary walls,
red cell reservoirs,
and red cell sedimentation.
19

TABLE 5.-
WEIGHT-CHANGE STUDIES CONDUCTED ON DRIVERS AT
DAYTONA INTERNATIONAL SPEEDWAY
Driver
Driving Control
time, hr
weight, lb
American Challenge Cup Race
Driver E
Driver F
Driver G
Driver H
Driver I
Driver J
Driver K
Driver L
Driver
A 2 148 144
143
-1
Driver
B 2.3 215
216.5 212
-4.5
Driver
C 2.5 166 166
165
-1
Driver
D 2.5 194 197 192.5
-4.5
Daytona Continental Race
166 164
-2
175
172
-3
180
179
-1
229.5
228
-1.5
188
187
-1
187.5
184.5
-3
136.5 134.5
-2
147
141
-6
20

TABLE 6.-
BLOOD-VOLUME STUDIES CONDUCTED ON DRIVERS IN THE
AMERICAN CI-IAIJXNGE CUP RACE AT DAYTONA INTERNATIONAL SPEEDWAY
Driver
Time
Blood
volume
AV
Plasma
volume
AV
Red cell
mass
AV Hct
A
Control
10 min 100
Tilt up
13 min
99.3
20 min
96.9
Tilt down
23 min 102.0
31 min 104.1
Post-race
10 min 100
Tilt up
18 min
97.4
Control
10 min 100
Tilt up
20 min 100.6
Tilt down
30 min 102.1
Post-race
10 min 100
Tilt up
18 min
98.7
Post-race
10 min 100
Tilt up
(Syncopel
Tilt down
13 min 100.1
(Syncope- No results)
-0.7
-3.1
+2.0
+4.1
-2.6
+0.6
+2.1
-1.3
+0.1
46.2
45.1
47.4
48.5
47.6
46.1
47.1
Driver A
Driver B
53.8
54.5
51.0
52.5
54.5
53.9
51.5
+0.7
-2.8
-1.3
+0.7
46.2
44.8
45.9
49.5
49.6
46.1
-2.4
45,.9
-1.4
-0.3
+3.3
+3.4
-0.2
-1.1
i-1.2
t2.3
+0.2
tl.O
-0.9
+2.1
-2.0
+0.2
52.7
51.8
54.8
51.5
49.5
47.3
48.5
46.3
48.5
49.8
47.3
48.8
47.3
48.5
49.2
+1.5
0.0
+0.7
45.6 45.6
45.5
-0.1 45.4
4-1.2
-1.0
t1.3
Driver C
54.4
54.6
-0.2
Driver D
21

Driver
Driver E
Driver F
Driver G
Driver H
Driver I
Driver J
Driver k
Driver L
TABLE 7;-
BLOOD-VOLUME STUDIES CONDUCTED ON DRIVERS IN THE
DAYTONA CONTINENTAL RACE AT DAYTONA INTERNATIONAL SPEEDWAY
Time
Post-race
10 min
Tilt up
18 min
Post-race
10 min
Tilt up
18 min
Post-race
10 min
.Tilt up
18 min
Post-race
10 min
Tilt up
18 min
Post-race
10 min
Tilt up
18 min
Post-race
10 min
Tilt up
18 min
Post-race
10 min
Tilt up
18 min
Post-race
10 min
Tilt up
18 min
Blood
volume
100
95.3
100
96.3
100
104.3
100
96.5
100
96.7
100
97.4
100
102.0
100
96.9
AV
-4.7
-3.7
+4.3
-3.5
-3.3
-2.6
+2.0
-3.1
Plasma
volume
AV
53.0
47.7
-5.3
55.9
52.4
-3.5
54.9
55.3
-0.4
51.6
48.1
-3.5
54.5
51.0
-3.5
52.0
50.3
-1.7
52.1
51.3
-0.8
46.1
46.2
+0.1
--
Red cell
mass
47.0
47.6
44.1
43.9
45.1
49.0
48.4
48.4
45.5
45.7
48.0
47.1
47.9
50.7
53.9
50.7
AV
-
-0.6
-0.2
+3.9
0.0
to.2
-0.9
t2.8
-3.2
Hct
A
47.0
50.0
+3.0
44.1
45.6
t1.5
45.1
47.0
t1.g
48.4
50.1
t1.7
45.5
47.2
t1.7
48.0
48.3
to.3
47.9
49.7
k1.8
53.9
52.3
-
-1.6
22

TABi 8.-
BLOOD-CHEMISTRY STUDIES CONDUCTED ON DRIVERS AT
DAYTONA INTERNATIONAL SPEEDWAY
Driver
Driver A
Driver B
Driver C
Driver D
Driver E
Driver F
Driver G
Driver H
Driver I
Driver J
Driver K
Driver L
.Normal
.
CO2 com-
Time
G1ucose BUN bin&g power Cholesterol
SGOT
SGPT LDH
American Challenge Cup Race
-
-
213
Pre
Post
214
Pre
Post
Pre
Post
2/2
Pre
Post
-7
Pre
Post
Pre
Post
Pre
Post
Pre
Post
Pre
Post
Pre
Post
Pre
Post
Pre
Post
-
76,
106
74
98
101
100
-7
15
15
15
25.5
189
6
4 400
24.0
223 13
8 440
17.0
240
19
14
420
13
25.0 2'15
4
6
11
25.5
208
13
8
13
18.5
309
28
16
2:
1410
112
95
g
24 24.0
175
11 6 420
24
18.0
203
16 10
780
13
24.0
223
10 8
i4
21.0
254
8
13
15 18.8
326
22
12
g::
790
Daytona Continental Race
122
116
~-
18
17
24.0
2’40
14 '10
23.0
215
11 12
22
25.0
240
6
22
24.5
237
12
--
'5'00.
420
400
450
103
17
23.5
200 6
58
15 16.0
200
15
440
640
105
12
24.0
170
7
8
550
70
13
22.0
180
13
9
640
14
25.5
249
19
23
510
17
18.0
212 22
10 680
108
17
26.5
I-85
12
6 440
60
15
21.5
212
16
8 620
114
12
25.5
187
50
17
21.0
185
115
25
26.5
40
30
18.0
60-95 5-20
m3 mg
percent
percen'
24-30
me+
258
270
180-300'
units
12
15
14
17
8-40
units
8
450
8
640
8 440
16
550
5-35
units
LOO-350
units
-
--
23
- ---. --- .-
Figure
3(a)
and (b):
Three drivers in the challenge. cup race had ele-
vated glucose in the control study while six of the eight drivers studied
in the endurance race had elevated values in the control samples.
This may be due to the samples not being drawn during a fasting period.
Although some drivers had little change in glucose concentration post-
race, the general trend was toward a decrease with the average being in
the low normal value.
Figure 4(a) and (b):
The CO2 combining power began at low normal
and during the race decreased about 25 percent with the average post-race
value well below normal.
Figure 5(a) and (b):
The LDH had.the greatest change. Initial val-
ues were elevated in all individuals before the race and rose to a height
of 1410 units post-race in one driver.
Two drivers had a decrease in LDH
after racing while others driving for approximately the same period of
time had increases.
During such short periods of driving, driving time
may not be an adequate estimate of physical exertion.
Other factors, such
as handling of car, congestion of track and other factors, which may in-
fluence the amount of work ,performed, need be considered. The high LDH
values and the low CO2 combining power indicate a tendency toward sub-
clinical acidosis. The degree seems to be greater in some than others.
In general, the values would correspond to that seen in moderate acidosis..
No correlation can be drawn to the amount of driving nor the interval be-
tween active driving and follow-up. There would be an expected return
to normal values within 3 to 6 hours after racing.
Comparison of the
results obtained on the two drivers who had a delayed follow-up and those
obtained within a short period, indicate recovery within the parameters
studied-may be more prolonged than expected.
Figure 6(a) and (b):
The urea nitrogen showed no significant changes
except .in one individual. In this case the urea nitrogen rose from
25 mg percent, which is slightly above normal, to 35 mg percent.
Figure 7(a) and (b):
Cholesterol concentration does not seem to be
a good indicator of fat metabolism.
This is probably due to the large
amount of cholesterol present in tissues which may be liberated into the
circulation.
No correlation seems to exist between driving time of any
of the drivers and the direction of change in cholesterol concentration.
Figure 8(a), (b), (c>, cd):
SGOT and SGFT were within normal or
slightly below normal in all drivers before the race.
The general pat-
tern was toward an increase but stayed within the low normal range.
24

0
0
Driver L
0
l
Driver H
-A
Driver I
&-A Driver J
V-V Driver E
1-r Driver G
-+
Driver K
-x
Driver F
__--..
(a) Daytona Continental Race
,
0
0
Driver A
0
Q
Driver D
x-
Driver B
A-
Driver C
I
(b) American Challenge Cup Race
I
FYgure 2.-
Legends for blood chemistry figures.
25

150
150
100
E
r”
0
40
30
J
\
0”
5
20
IO
100
50
I.
I
I
I
a
--m---w
I
--------------
Ii
b
I
z
--------------------
- ----
I
control pre
P-t
pre
F-t
(a) American Challenge Cup Race.
(b) Daytona Continental Race.
Figure 3. - Blood chemistry, glucose.
I I
I
control pre
post
(a) American Challenge Cup Race.
P-t
(b) Daytona Continental Race.
Figure 4. -
Blood chemistry, CO2 combining power.

IO00
UJ
f
3
500
control pre
post
50
*
r”
25
0
1000
u)
.c,
Ei
(a) American Challenge Cup Race.
il
I ------------------_------
I
J
pre
P-t
(b) Daytona Continental Race.
Figure 5. - Blood chemistry, lactic dehydrogenase.
1
I
control pre
1
post
-em----- ------- -------____
E &e&C
e
mm
I, .
-------_ ---------- ---_- _ _ ---
(a) American Challenge Cup Race.
(b) Daytona Continental Race.
Figure 6. - Blood chemistry, blood urea nitrogen.

control pre
post
(a) American Challenge Cup Race.
100 1
I
I
pre
Post
(b) Daytona Continental Race.
Figure 7. -
Blood chemistry, cholesterol.

control pre
post
(a) SGOT, American Challenge Cup Race.
(b) SGOT, Daytona Continental Race.
30
;I
control pre
post
(c) SGPT, American Challenge Cup Race.
Figure 8.
30
20
IO
l
C
s
,
r
AYA
4o 9
E
z
A
.- --e-s_--
-----.. ---me
I
pre
I
P-t
I
-__- ----------------------- ----
I t
30
20
a
E
b
2
IO
! ii&
1
V
n ---------
-s_----- ----
--
C
c
X
me
post
(d) SGPT, Daytona Continental Race.
Blood chemistries.

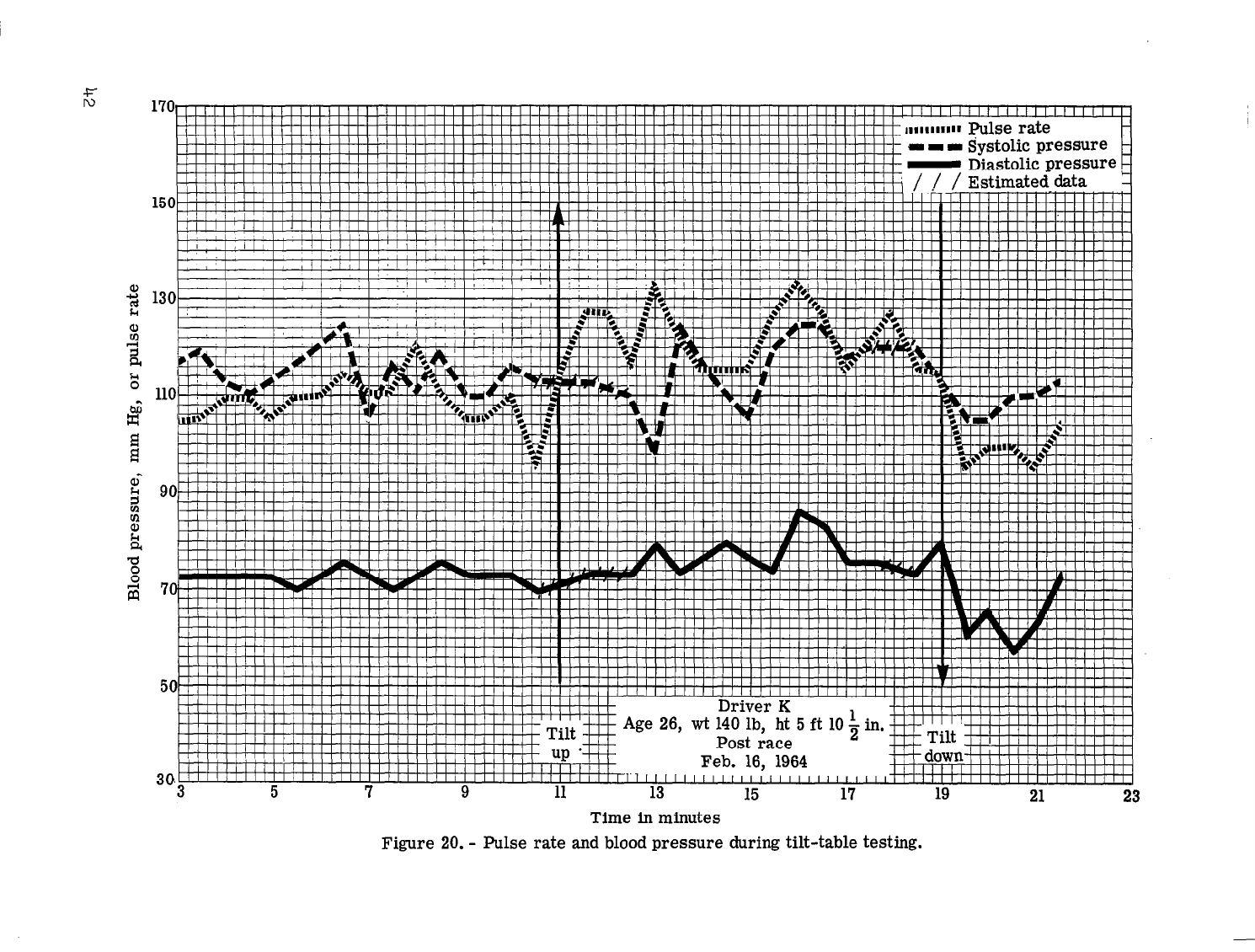
Comments. on tilt table tests, Daytona race._(figs. 9 through 22).-
Two of-the Daytona drivers have pre-race control studies and post-race
studies suitable for direct comparison. A third driver showed syncope on
tilting in his control.and is unsuitable for comparison.
In the control studies both Drivers B and A have a cardiac output
that is adequate to maintain an almost level systolic pressure on tilting
up.
However Driver B maintains systolic pressure without an appreciable
increase in pulse rate and therefore must accomplish this by an increase
in stroke volume.
Driver A maintains systolic pressure by a rise in pulse
rate from 115 to 160 and therefore is assumed to rely upon a lesser stroke
volume with this increase in pulse rate.
Post-race, both drivers show an immediate rise in pulse rate which is
maintained throughout the tilt at approximately 136 by Driver B and ap-
proximately 150 by Driver A. Driver B shows a momentary fall of systolic
pressure and pulse pressure,
with the recovery apparently by increasi.ng
stroke volume.
Driver A shows a sloti fall in systolic pressure and pulse
pressure with a slow recovery,
also apparently by increasing stroke volumes.
The remaining nine drivers were not available for control studies and
only post-race tilt table studies were made.
Diastolic pressure is main-
tained or rises in seven of the nine,
indicating effect of vasomotor re-
sponses following the stress of driving. Two of the nine who showed a
fall in diastolic pressure, indicating a failure of vasomotor reflexes,
were under the greatest handicap. Driver C had worked on his race car
all the preceding night and had 1 l/2 hours of sleep.
He maintained dia-
stolic pressure for approximately 1 minute when tilted up, then diastolic
pressure and vasomotor control failed resulting in syncope. Driver I
had driven 7 l/2 hours with a 3 l/2 hour drive in darkness just before
testing.
He maintained diastolic pressure for approximately 4 l/2 minutes
in tilt and then lost diastolic pressure and vasomotor control.
The tilt
was ended to prevent syncope.
Both initially maintained systolic pressure and then showed a sudden
loss in both systolic pressure and pulse pressure. Driver C had maintained
his systolic pressure at 100 mm of mercury for approximately 1 minute, by
rise in pulse rate from 100 to 150.
The pulse rate of approximately 150
is maintained even after systolic pressure begins to fall, indicating a
diminution in stroke volume.
Driver I maintains systolic pressure at approximately 100 rmn of mer-
cury by rise in pulse rate
from
approximately 75 to 112. A fall in pulse
rate to 54 preceded the fall in systolic pressure with no corrective re-
sponse by way of an increase in pulse rate to offset the fall in systolic,
diastolic,
and pulse pressures.
Three drivers (F, H, and G) show a notably stable pattern through the
tilt table test with a rise in diastolic pressure indicating a strong vas-
omotor response,
a moderate increase in systolic pressure by means of a
moderate increase in pulse rate, and, by inference, an increase in stroke
volume.
Four drivers (J, L, K, and E) have a comparable response pattern to
tilt except for a more marked increase in pulse rate to maintain the sys-
tolic pressure and, inferentially, a smaller stroke volume.
30

mrlmm
Pulse rate
I I
I I I
I I
I I I I I I
I
I I I I I I I
I I I
I I I I
I I I I I
I, I I
Time in minutes
Figure 9. -
Pulse rate and blood pressure during tilt-table testing.

151
3
. .
I Il.
r
t
110
I
; i i
IllI
VW
,3 5 7 9 11 13 15 17 19 21 23
Time
in minutes
Figure 10. -
Pulse rate and, blood pressure during tilt-table testing.

160
.I I I ;sysroiic pressure
- Diastolic pressure
/ / / Estimated data
6
6
a 24
26
28
Time in minutes
Figure 11. -
Pulse rate and blood pressure during tilt-table testing.

.--
-.I
--
-A
--
---
--,
--
--
4~zz-----
--‘-‘--l----++, I I I I I I 1-1-1 1-1 I I’l I I I I I I I I I I ‘i---ytttH~~$ti-’
4 6
a
10 12 14 16
24
Time in minutes
Figure 12. -
Pulse rate and blood pressure during tilt-table testing.

~~~~~~~~~~IIIIIIIIJIIIIIIIII~II~I~IIIIIII~IIIIIIIIIIII~IIIIIIIIIIIIIII~IIIII~III~III~II~~~~~~ I
2O~II’I’II~“I’II’III~“I’I’~‘I”I””~””I”I’~III”II”“‘I”III’I’I~”~~~~~~~“~~“~~~‘~~~~~~~~~~
3
5 7
9 11
13 15 17
19 21
23
Time in minutes
Figure 13. - Pulse rate and blood pressure during tilt-table testing.

i i i i7-i i i i i I i i i FJ_ i Pi i i i 72 i i i i
*
rJ I
7 m.,.-
!
Age 36, wt 187
lb, ht 5 ft 9 in.
Post
race .
10”“““““““““““““““““““““““““““““”””””””’~~’~~~”“~~~~~~~~~”’~”~
0 2
4 6 a
10 12
14 16
ia
Time in minutes
Figure 14. -
Pulse rate and blood pressure during tilt-table testing.

1 I I Systolic pressure 7
Diastolic pressureE
/ / / Estimated data
r
r I
--
--
--
Time in minutes
Pigure 15. -
Pulse rate and blood pressure during tilt-table testing.

201-L
---- -I
El I I I 11 I 1 I I I 11 I 11 I I I I I I 1 I I I I I iii
-7-
--- -- ilii i i
--
i ii 1
Zl
i 1.1 ii i ii 11
3 5 9 11 13 15 17 19 23
Time in minutes
Figure 16. -
Pulse rate and blood pressure during tilt-table testing.

w
ul
Time in minutes
Figure 17. -
Pulse rate and blood pressure during tilt-table testing.

3
5
7
9
11
13 15
17
19
21
23
Time in minutes
Figure 18. - Pulse rate and blood pressure during tilt-table testing.

Estimated data
Time in minutes
Figure 19. -
Pulse rate and blood pressure during tilt-table testing.
1-1 !hatnlir
nwssure
- l3instnliC pressure
Ited data
liiii iii / / / / /i / ii iL,
IllllllllllllllllllIII1IIIIlII1I
II IllI IllIIlIIIIIIIIIIIlIIIIIIrlIIITIII~lr~
Feb. 16, 1964
303
III III III1
I I I I I I I I I I L
5 7 9 11
13
15 17
in,
B
III
II I I I I I I I II I III1 I II II II II
19
21
23
Time in minutes
Figure 20. -
Pulse rate and blood pressure during tilt-table testing.

160
rate
140
120
100
80
60
40
20
Time in minutes
Figure 21. -
Pulse rate and blood pressure during tilt-table testing.

/ / / Estimated data
I
, / I
120
I I
I I
I
A
T I
/ I
I,!:
I I I I
I
kontrol
Feb. 2,
I I I I I I I
teh
1964
Time in minutes
Figure 22. - Pulse rate and blood pressure during tilt-table testing.

GALVESTON SPORTS CAR RACE, JULY 1964
Comment on figure 24(a) and 24(b).-
Glucose: The pre-
and post-race serum glucose concentrations showed
a consistent increase in the seven studies obtained. The maximum increase
the first day was 87 percent with the lowest being 30 percent. Two of the
same drivers were studied the second day and indicated a more profound in-
crease in glucose concentration.
The maximum increase for the second day
was 303 percent with the lowest being 24 percent.
Comment on figure 25(a) and 25(b).-
Cholesterol: The pre- and post-race cholesterol values again indi-
cate variable response.
It is interesting to note that a decrease in
cholesterol level was noted both days on the same driver. Others consis-
tently had increases.
Whether this is an individual variation can only
be speculated. Only one driver had a significant elevation and this was
in his pre-race sample. It was not possible to obtain a follow-up on
this driver.
Commenton figure 26(a) and 26(b).-
Uric acid: Pre- and post-race uric acid concentrations showed vari-
able response. Three of the seven studies performed had essentially no
change while two had increases and two decreased.
Two of the drivers who
had no change the first day were followed the second day with significant
decreases in uric acid concentration post-race.
Comment on figure 27(a),and 27(b).-
Creatinine: The predominant direction of change in the creatinine
concentration was toward an increase.
Six of the seven studies indicated
an increase while one had a decrease on the first day but on the next day
he had a significant increase.
Although the normal values stated are
lower than the pre-race control values, the serum creatinine may have val-
ues up to 1.8 mg percent under normal daily activity.
The activities of
these drivers up to the time the control samples were drawn cannot be
classified as normal daily activity; therefore,
the high pre-race values
are not significant.
Comngk on figure 28(a) and 28(b).,
Chloride:
The principle change was toward an increased chloride con-
centration probably associated with increased retention. Two drivers, showed
decreases. This may be associated with high fluid loss (perspiration)
without retention as both had pre-race levels above normal.
Comment on figure 29(a) and 29(b).-
Phosphorus:
The most consistent change- observed was a decrease in
inorganic phosphorus.
This is probably a result of an increase in carbo-
hydrate metabolism and increased excretion of acid phosphates by the
kidneys.
45

a
Driver H
0
Driver J
u
Driver E
A
Pre race studies on
additional drivers
(a) July 4,
1964
8
l
Driver H
o-------------O Driver E
- Driver G
- Driver D
P
Driver L
(Post race only)
(b) July
5, 1964
Figure 23.-
Legends for blood chemistries,
San Jacinto Regional Race,
Galveston, Texas
46
. . . . .

400
.---o--e
----_-_
I
I
Pre
Post
(a) July 4, 1964.
Figure 24. -
Blood chemistry,
glucose,
San Jacinto Regional Race.
t
0
400
I
I
Pre
Post
(b) July 5, 1964.
200
200
--m---
I
I
Pre
Post
(a) July 4, 1964.
t
I
I
Pre
Post
(b) July 5, 1964.
Figure 25. -
Blood chemistry, cholesterol, San Jacinto Regional Race.
f

I
2
de
2
1
Pre
(a) July 4, 1964.
Post
de
2
A-----
I
Pre
u
I
Post
(b) July 5, 1964.
Figure 26. -
Blood chemistry, uric acid, San Jacinto Regional Race.
-J !F==z E 2
s------e---- m----e-----
Norm.
1
- ---------------------
3
Pre
(a) July 4, 1964.
Post
’ Norm.
,- ---------------------
t
I
I
Pre
Post
(b) July 5, 1964.
Figure 27. -
Blood chemistry, creatinine, San Jacinto Regional Race.

I
i
-
Vorm.
I
Pre
I
Post
I
200 :-
T
i
-h==yda ’
100 -=
-a- m-b--
----
f
--v
-----------
Norm.
I
Pre
I
Post
(a) July 4, 1964.
(b) July 5, 1964.
Figure 28. - Blood chemistry, chlorides, San Jacinto Regional Race.
I
I
I
I
Pre
Post
Pre
Post
(a) July 4, 1964
(b) July 5, 1964.
10
Figure. 29. - Blood chemistry, phosphorus, San Jacinto Regional Race.

TABLE 9.-
VITAL STATISTICS OF SUEUECTS IN RACES AT GALVESTON, TEXAS, IN
1964
Driver
Iriver A
Driver B
Driver C
Driver D
Driver E
Driver
F
Driver G
Driver H
Driver I
Driver J
Driver K
Driver L
Physical description
T
(eight
Height
ge
156
200
170
180
190
173
193
165
180
200
160
5 f't 9 l/2 in
5ft2
in
5 ft 9 in
5
ft 10 in
6
ft
2 in
5 ft 11 in
6
ft
2 in
5
ft 10 in
5 ft 10 in
5 ft 9 in
61% 2
in
5
ft
8 in
37
Photographer Yes
(commercial)
2 children
34
Business
Yes
executive
1 child
51
M.D. (Radio- Yes
M.D.
logist)
3
children L.L.B.
47
Retired Col.
28
Mechanic and Yes
sales
2 children
35
Electronics Yes
business 4 children
39
Airline
Yes
Business
pilot 2 children
math. major
33
Chemical
Yes
1 l/2 yr
operator
4 children Jr. College
51
Auto
Yes
mechanic
1 child
32
M.D.
43
43
Personnel
Yes
Director 1 child
Investor
Occupation
Barital status
and
10.
of childrer
Yes
West Point
2 children graduate
Yes
2 children
Yes
3 children
l-
Education
M.S. in pho-
tography
4 yr college
1 yr college
G.M. Train.
Center
M.D. Sports
High school
2
yr college
Racing
5Pe
Sports
5
Sports 8
Sports
3
Sports
1
Sports
3
Sports
Sports
Sports
6
Sports
12
3
4
3
1
10
mxperience
No. of
years
Rest prior
to race
6 hr sleep
7
hr sleep
7 hr sleep
9 hr sleep
5
hr sleep
8 hr sleep
No sleep
before
racf
working ant
drive
'j' hr sleep
5 hr sleep
5
112
hr
sleep
7 hr sleep

TABLE lO.-
PRE- AND POST-RACE TEMPERATURE, PULSE, AND BLOOD PRESSURE
READINGS OF DRIVERS IN THE RACES AT GALVESTON, TEXAS
Name
Driver A
Driver B
Driver D
Driver E
Driver E
Driver F
Driver G
Driver H
Driver H
Driver I
Driver J
Driver K
Date
7-4-64
7-5-64
7-5-64
7-4-64
7-5-64
7-5-64
7-5-64
7-4-64
7-5-64
7-4-64
7-4-64
7-4-64
_ .-
p
Ti
-= --:-
Pre-race
__.~. -~.- ~~
4:35
11:50
11:30
4:45
11:oo
11:55
3:oo
1:45
9:45
2~23
4:lO
2:lO
e
Post-race
/
3:30
5:40
3:45
2:30
3:25
12:40
4:30
5:lO
4:oo
I
Temper
Pre-race
99.0
99.0
99.4
99.6
100.0
99.0
97.2
99.8
99.2
98.6
98.6
99.0
are, "F
Post-race
l-
100.2
99.2
99.8
101.0
100.8
99.2
101.0
100.4
100.2
99.4
99.2
BlOOd F
4ssure
Pre-race Post-race
110/70
128/80
138/9o
130/80
130/80
118178
130/70
lO4/78
‘I
l38/110
150/100
140/80
130190
Comment:
The maximum ambient temperature was 102' F with intermittent cloudiness and
light breeze so that this day was not oppressively warm. Of 11 drivers only 4 showed a rise
in body temperature of more than lo during & race. The maximum body temperature recorded was
101.O" F but this represented a rise of
3.8O
for one driver.
Three drivers with blood pressures before and after racing all showed a slight increase
in both systolic and diastolic pressure with pulse pressure remaining constant in two and
narrowing slightly in one driver.
51

TABLE 11.- WEIGBT-CHANGE STUDIES CONDUCTED ON DRIKERS
IN THE GALVESTON RACES IN 1964
Driver
Date
Pre-race
Post-race
Weight
weight
weight
loss, lb
Percent
Driver A
Driver B
Driver D
Driver E
Driver E
Driver F
Driver G
Driver H
Driver H
Driver I
Driver J
Driver K
7-4-64 153
-mm --- ---
7-5-64
so-
--w ---
---
7-5-64 180
180 0
7-4-64 186
--- --- ---
7-5-64 183
182 1 .5
7-5-64 ---
173 --- ---
7-5-64 196
193 3 1.5
7-4-64 160
159 1 .6
7-5-64 160
157 3 1.9
7-4-64 155
154 1 .6
7-4-64 177
177 0
7-4764 1%
195 3 1.5
Comment: Three drivers each showed a weight loss of 3 lb. The percentage losses
of body weight paired with temperature changes were: 1.9 percent and +l.O" F, 1.5 per-
cent and +O.2" F, and 1.5 percent and +3.8" F.
No correlation can be attempted but future observations with larger numbers of
subjects and closer attention to details of cockpit temperature, car construction,
and'clothing may be profitable.
52

TABLE 12.- BLOOD-CHEMISTRY STUDIES CONDUCTED ON DRIVERS .
IN THE RACESATGALVESTON, TEXAS
Driver Time
Glucose Cholesterol Uric acid Creatinine Chloride
Phosphorus
Driver A
.
Driver C
Driver E
Driver H
Driver I
Driver J
Driver K
Driver D
Driver E
Driver G
Driver H
Driver L
Normal
Pre-race
Post-race
250
2.8
1.47
184
6.9
Pre-race
Post-race
42 208
5.5
1.68
117 4.5
Pre-race
Post-race
Pre-race
Post-race
a2
153
91
118
be-race
Post-race
120
208
116
208
332
258
Pre-race
72
124
Post-race
122
214
Pre-race
Post-race
70
378
Pre-race
Post-race
Pre-race
Post-race
Pre-race
Post-race
h-e-race
Post-race
Pre-race
Post-race
92
253
84
179
84
104
2;:
227
236
7.7
7.5
6.3
3.3
2.7
4.9
2.8
1.9
2.02
2.53
191
173
160
218
145
182
2.00
2.36
1.47
1.92
1.37
1.81
282
1.3
2.63 112
3.5
70-105 120-160
3.5-6.0 0.6-1.3
mg w
mg
w
percent
percent
percent
percent
July
4, 1964
2::
2.5
2.4
2.3
c-z
.
26.0
July
5, 1964
1.79
2.00
1.68
1.47
1.58
223
110
104
120
111
C::
5.6
2.7
2.7
1.52
123 3.7
1.68
113
2.8
1.58
116
3.6
125
137
125
130
117
124
98
109
loo-106
m-x/l
2.7
2.2
4.0
3.4
4.1
3.8
3.1
2.2
3.0-4.5
w‘
percent
53

Comment on table 13.-
Sugar:
Pre-race urine samples all had sugar present except that
from one driver. The qualitative amount ranged from a'trace up to 2+.
post-
race samples indicated either no change in excretion of sugars‘or increases
up to 3+.
One driver had a decreased excretion during competition, falling
from 2+ to trace amounts.
His pre-race serum concentration was 70 mg per-
cent at the same time his urine sugar was 2+.
This pattern may be expected in non-fasting individuals if at one
time he had a high intake of glucose with no voiding until the time the
samples were taken.
Sodium:
All drivers from whom we were able to obtain pre- and post-
race urine samples during the second day of racing had a decreased sodium
concentration.
The percent decrease ranged from 5 to 35 percent.
There
is close correlation between the percent decrease in sodium excretion and
the percent increase in chloride concentration in the blood.
Potassium:
An increased potassium concentration was observed in
three of the four drivers studied.
The fourth had no change. Driver F
had mechanical trouble while on the track and there was a long delay
before return to the testing area. This may account for a return to
normal potassium concentration in the urine.
Apart from this individual,
the magnitude of increase appears to be associated with the magnitude of
decrease in sodium concentration.
Osmolality:
The total concentration of solutes in the urine appears
to be quite variable with maximum changes toward a decreased concentra-
tion.
This correlates with the decrease in sodium concentration in the
urine being greater than the increase in potassium. A decreased ex-
cretion of other materials may account in part for some of the observed
increases in plasma concentration.
Additional information on creatinine excretion and uric acid ex-
cretion may be useful.
Creatinine is not reabsorbed and the concen-
tration in the urine may indicate the water concentration.
54

TABLE 13.-
PRE- AND POST-RACE ljRINALYSES OF DRIVERS
IN THE RACES AT GALVESTON, TEXAS
_.- - .-. - -.~
Name Time Sugar
Na, Na,
meq/l
me& Osmolality
July 4, 1964
Driver A
Driver E
Driver H
Driver I
Driver J
Driver K
1.
Driver B Pre-race
Post-race
1+
2+
---
---
132
66
---
869.2
Driver E Pre-race
Trace
124
112
830.5
Post-race Trace
118
116
854.3
Driver F Pre-race
Trace
184
72
Post-race
Trace
120
72
Driver G Pre-race Trace
116
Post-race l+
88
Driver H
80
98
76
100
“8$*0”
.
846.7
922.6
Pre-race
Trace
176
Post-race
2+
116
1110.3
922.6
Driver L
Post-race Trace
108
82
992.4
Pre-race
Post-race
Trace
---
Pre-race
Post-race
Trace
Trace
Pre-race
Post-race
Trace
l+
Pre-race
Post-race
1+
3+
Pre-race
Negative
Post-race
Trace
Pre-race
2+
Post-race Trace
---
---
---
---
---
---
---
---
m-m
---
---
---
July 5, 1964
---
---
---
---
---
---
---
-we
-mm
---
-em
---
m-e
---
---
---
-es
---
-mm
---
---
---
---
---

Comment on tilt table tests -
Galveston, Texas (figs.
30
through
38).-
Driver I:
In the control test there is delay and temporary fall in
systolic
pressure
which in general is maintained by only a slight rise in
pulse rate,
indicating an appropriate stroke volume response. The
diastolic pressure rises slightly, indicating a satisfactory vasomotor
response.
The post-race tilt table test shows a dramatic change. The pulse
pressure is very narrow due principally to a drop in systolic pressure
despite a rise in pulse rate.
This must mean a poor stroke volume
response.
Diastolic pressure falls only slightly which may be taken to
indicate a fairly satisfactory vasomotor response.
This distinctive pattern is the only one of its type that we have
seen. This subject,
age
51,
has been quite successful in competitive
driving.
Driver H has two tracings, both following races, one of which he won.
There was no control test.
In general this man maintains his systolic
pressure well with only a very slight rise in pulse rate, indicating a
good stroke volume.
He maintains a good diastolic pressure, indicating
satisfactory vasomotor response. This 33-year-old man shows the response
that is expected of a man in good condition whose occupation is an
airline pilot.
The graphs of Driver E and B are both post-race. No controls are
available, but they show a sharp contrast.
The older individual,
Driver B, age
35,
shows good maintenance of systolic pressure with only
a small rise in pulse rate. The pulse pressure is well maintained.
Diastolic pressure rises slightly during the tilt. Driver E, age 27,
the younger individual by
8
years,
shows a very narrow pulse pressure
with a falling diastolic pressure despite a rise in pulse rate, indi-
cating a poor stroke volume response. His diastolic pressure is well
maintained,
indicating a satisfactory vasomotor response.
Driver J, a 32-year-old physician, shows a temporary fall in systolic
pressure with only a slight rise in pulse rate, indicating perhaps an
inadequate stroke volume response.
The diastolic pressure rises sharply
producing momentarily a very narrow pulse pressure.
Driver F, age
35,
shows a small fall in systolic pressure and a
slight rise in pulse rate,
indicating a reasonably satisfactory combined
response of pulse rate and stroke volume. A level diastolic pressure is
maintained, indicating a satisfactory vasomotor response. This man is a
very competitive driver.
Driver D, age
47,
shows well maintained systolic and diastolic
pressure with only a small increase in pulse rate, indicating a good
stroke volume response and a good vasomotor response although the pulse
pressure narrows appreciably during the tilt. This man is believed to
have diabetes and hypertension under medical treatment.
56

Time in minutes
Figure 30. -
Pulse rate and blood pressure during tilt-table testing.

160
2a
I
0
2
Driver I
,t 155 lb, ht 5
Post race
July 4, 1964
==-v
ft 10 i in.
Time in minutes
Figure 31. -
Pulse rate and blood pressure during tilt-table testing.

0 2
4 6
8 10
12 14 16
18
Time in minutes
Figure 32. -
Pulse rate and blood pressure during tilt-table testing.

160
JllIlJlllIlllllllll,lll,lLll,/J/ll\l,lllLl,lJll\llll/lIJI,llIlIl/lJllll~l,ll
- - - Systolic pressure
- Diastolic twessure
/ / / Estimated data
Driver H
LAge33, wt165lb,
L
Post race
--
207-----I
d
11 ‘1 ” ’ “1 11
11 11 1 I ’
Time in minutes
Figure 33. - Pulse rate and blood pressure during tilt-table testing.

:-
, 11L ” Lb Y Au.
40
0
Time in minutes
Figure 34. - Pulse rate and blood pressure during tilt-table testing.

I I I I I I I I I I I I I I I I I I I I I I II
Driver B
lll1llllI11lllll~ll I:‘!;IIIIlllll I llI/l/II l/III ‘1
wt 200 lb, ht 6 ft
Post win
July 5, 1964
6
8
10 12
14 16
18
20
Time in minutes
Figure 35. -
Pulse rate and blood pressure during tilt-table testing.

- Diastolic pressure i
/ / / Estimtted data
1
8
Time in minutes
Figure 36. -
Pulse rate and blood pressure during tilt-table testing.

L--e---
-i-
-----d-y
----
0
2
4 6
8
10
12
14 16
18
Time in minutes
Figure 37. - Pulse rate and blood pressure during tilt-table testing.

- - - Systolic pkessure
,, , 1 ,,k’ I , , , / , , , , , , ,
w
‘I! iI;,
IIll 1111111111111/,1ll,1111
-1 ‘IICL1 !
c
I’l!ll!illlllllll~lII~‘,!I~‘~ II/I(IlIII(/IllIl///~il
80
60
Age 47, wt 180 lb, ht
Post race
+W UP II down
I I I I
20
0
2 4
6
8
10
12 14
16
18
Time in minutes
Figure 38. -
Pulse rate and blood .pressure during tilt-table testing.

Comment on telemetry record - Driver E (fig. 39).- The dominant
events during this in-race telemetry record of heart rate are numbered
on the graph.
(1) The pulse is approximately level at 110 while the drivers are
waiting in their cars on the line for a plane to take off from an adjacent
runway.
(2) At the signal
"start your engineslr
the pulse rate rises
sharply to
146.
suddeL3?is!?E %
f1
ag
falls and the race starts there is another
. Throughout the.race this driver held second
place with very little fluctuation in the pulse rate between 170
and
186.
(4) At index 4 there was malfunction and his car was suddenly
out of competition.
/F\
Thereafter the pulse rate dropped precipitously
\// .
(5)
As the car and driver retire to the pits the heart rate
promptly falls.
A longer period of observation would have been desir-
able but the driver has usually disconnected before he can be reached
to hold him for a record of return to baseline.
66

200
180
160
140
120
100
I
I I I I / , / /
IllI I I ~lliiiiiiiiiiiiiiiiiiiiiiiiiiiiiiiiiiiiiiiiiiil
12
Time in minutes
Figure 39. -
Pulse rate history during race.

AUSTIN SPORTS CAR RACE, AUGUST
1964
The course for this event was laid out on the city streets of
Austin, around the City Auditorium in Austin. This is unusual for this
part of the country; narrow roads, curbs, tight corners contribute some
additional hazards and a large enthusiastic crowd tends to heighten ex-
citement.
The temperature varied during the day because of cloudiness
with a maximum of 101" F but a high humidity because of heavy rain the
previous night.
On this occasion the Hamilton Standard Company had provided a "cool
suit" for testing. Two individuals (Drivers B and C) each ran two races,
one with and one without the suit.
One driver (F) accepted the "cool
suit" and rejected the medical testing apart from pre- and post-race
oral temperatures.
This garment is well enough known to require only
brief descriptions;
it is a two piece set of thermal underwear lined
with fine plastic tubing through which ice water is circulated by an
electric fuel pump from a reservoir filled with ice water.
No regulation
of flow or temperature was possible and the initial effect on the wearer
was one of shockingly effective cooling.
In-car records of ,electrocardiograms and temperature were obtained
by a s-channel recorder (PEMCO model 110) and by telemetry equipment
provided by NASA.
Pre- and post-race tilt table tests were carried out
for comparison of the effects of driving with and without the "cool
suit."
Driving without the cool suit,
drivers showed minimal temperature
rises of l.O', 0.6", and 1.2". With the cool suit the same drivers
showed respectively temperatures rises of 2.0", 1.4", and 0".
The number of drivers and the minor heat stress provided in the
day preclude a useful impression of the effect on body temperature.
However two drivers showed a greater rise in body temperature with the
cool suit than without. It might be anticipated that for short periods,
abrupt cooling of body surface would result in a superficial constriction
and conservation of body heat with a temporary rise in internal tempera-
ture.
The blood pressure readings before and after racing, with and with-
out the cool suit, do not provide an adequate basis for comment, but-
interesting correlations with temperature and tilt table testing should
be found on future observations.
68
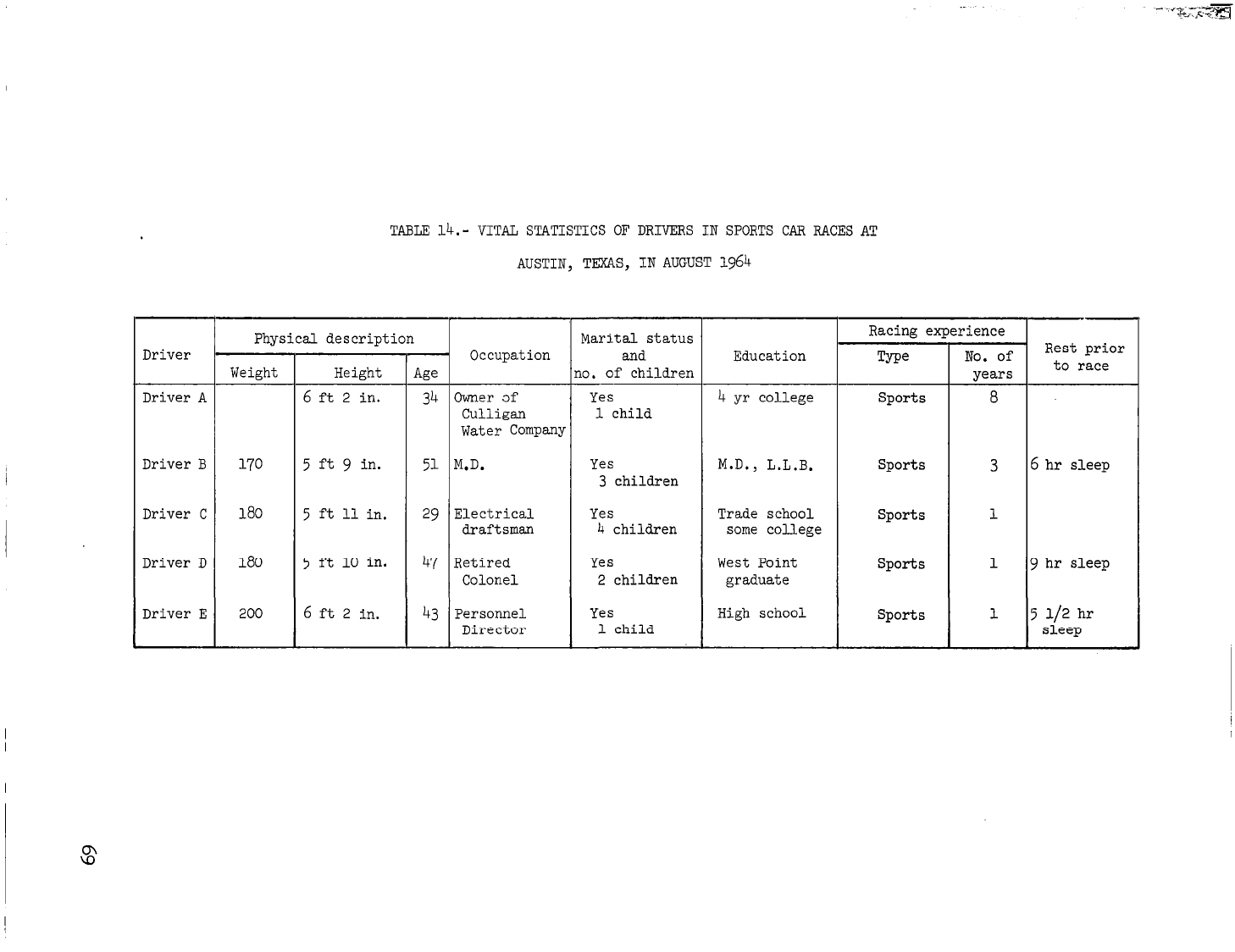
TABLE 14.- VITAL STATISTICS OF DRIVERS IN SPORTS CAR RACES AT
AUSTIN, TEXAS, IN AUGUST 1964
--
Physical description
Marital status
Racing experience
Driver
I
Occupation
and
Education
Q-w
No. of
Rest prior
Weight
Height
Age
no.
of children
to race
years
Driver A 6 ft 2 in. 34 Owner af Yes 4 yr college Sports 8
Culligan 1 child
Water Company
Driver B 170 5 ft 9 in. 51 M.D. Yes M.D., L.L.B. Sports 3 6 hr sleep
3 children
Driver C 180 5 ft 11 in. 29 Electrical Yes Trade school Sports 1
draftsman 4 children some college
Driver D 180 5 ft 10 in. 47 Retired Yes West Point sports 1 9 hr sleep
Colonel 2 children graduate
Driver E 200 6 ft 2 in. 43 Personnel Yes High school Sports 1 5 112 hr
Director
1 child
sleep

TABLE 15.-
PRE- AND POST-RACE TEMPERATURE READINGS OF DRIVERS
IN SPORTS CAR RACES AT AUSTIN, TEXAS, IN 1964
Driver
Driver A
With ice-cooled suit
Without cooled suit
Driver B
With ice-cooled suit
Without cooled suit
Driver F
With ice-cooled suit
Without cooled suit
Temperatures
Blood pressure
Pre-race,
Post-race,
OF
"F
99.8 101.2
99.6 100.2
98.0 99.8
99.0 100.2
,
I
98.8 100.0
98.0 99.0
Pre-race
1
Post-race
I
124196
110178
13o/78
130178
---
22170
120170
142175
---
I
---
--- ---

TABLE 16.- WEIGHT-CHANGE STUDIES CONDUCTED ON DRIVERS IN SPORTS CAR RACES
AT AUSTIN, TEXAS, IN AUGUST 1964
Driver
Pre-race Post-race
Loss Percent of weight
weight
weight
in lb
loss
Driver A
With cool suit
201
Without cool
(
198.3
2.5
1.2
198
-mm
suit
Driver B
With cool suit
---
169
---
Without cool
173
169
4
2.3
suit
Driver C
Without cool
suit
180.5
179.5
1
.6
Driver D
Without cool
suit
177
175
2
1.1

TABLE 17.- BLOOD-CHEMISTRY STUDIES CONDUCTED ON DRIVERS
IN SPORTS CAR RACES AT AUSTIN, TEXAS, IN AUGUST 1964
Driver Time
Glucose
I
Cholesterol Uric acid
I
Creatinine
Driver A
Pre-race
156 185
With cool suit
Post-race 6
107
118
Without cool suit Post-race 12
105
147
Driver B
Pre-race
121
196
With cool suit Post-race 10
91
200
Without cool suit 1 Post-race 4
123 239
Driver D
Pre-race
123
235
6.8
1.79 125
2.4
Post-race
144
147 7.3
1.79
128
1.7
5.3
2::
4.5
::“4
4.42
2.00
1.96
1.28
.24
3.5
1.92
129
2.0
2.95
126
1.6
Chloride Phosphoxxs
I I
124
3.5
125
2.2
3.8

Comments on figures, 41 through 46.-
Glucose (fig. 41):
The three drivers showed pre-race blood sugar
levels at or.above the usual upper limits of normal fasting values.
However these were taken at the site of the race, after breakfast, and
after varying exertions.
Post-race, one driver (B) shows the slight rise
that is commonly seen with stress of short duration, then a fall after
his second race.
A second driver (A) showed a fall to fasting levels
after his first race (with cool suit) which is closely maintained after
his second race (without cool suit). A third driver (D) (who did not
wear a cool suit) showed a rise from 123 to 144 mgm percent over a period
of 6 hours spanning two races.
These values demonstrate only the labile nature of serum glucose
levels under the effect of stress and exertion and indicate that useful
information might be gained from several samples closely coordinated with
glucose intake and hematocrit estimations.
Cholesterol (fig. 42):
The cholesterol values stayed within nor-
mal limits throughout the period of observation with only small changes
of inconstant direction.
Uric acid (fig. 43):
The uric acid concentration increased through-
out the day in all three drivers. Driver B did not have an increase
during his first race but did show a 2.0 mg percent increase after the
last race.
This was the maximum increase observed.
Creatinine (fig. 44):
Three subjects showed the possible varia-
tions,
one rose, one fell,
and one remained level.
The only comment is
that the blood chemistry might be of value if the baseline observations
were greatly extended before and after the period of stress.
Chlorides (fig. 45):
The chlorides showed very slight increases
in all three drivers.
Pre-race values were all elevated between 16 and
18 percent.
A slight increase was continuous throughout the day reaching
22 percent above normal.
Phosphorus (fig. 46):
The pattern of changes in the phosphorus
concentration varied from individual to individual.
All values were be-
low normal except the pre-race in one driver and after the final race
in another.
No explanation for the increase in concentration observed
in Driver A can be offered.
73
I

0
0
Driver B
0
0
Driver A
Figure 40.-
Legends for blood chemistries,
Alamo Regional Race,
Austin, Texas,
August 16, 1964.
74

200
I
g 1oo
I
AL;~-~~~ --------
--
f
e---w-- -_----------------------
Pre
Post-l Post-2
Figure 41. -
Blood chemistry, glucose,
Alamo Regional Race, August 16, 1964.
10 -
dc
2
--&I!~-----
s-
--- ------L---------------
f
I
I I
I
Pre
Post-l
Post-2
Figure 43. - Blood chemistry, uric acid,
Alamo Regional Race, August 16, 1964.
2
I
I
I
I
Pre
Post-l
Post-2
Figure 42. -
Blood chemistry, cholesterol,
Alamo Regional Race, August 16, 1964.
: xP
-- L --
----------------
1
t
Norm.
t
_ ---_----------------_
f-
L
I
I
I
Pre
Post-l
Post-2
Figure 44. -
Blood chemistry, creatinine,
Alamo Regional Race, August 16, 1964.

20
J
.
z
It
.-
i
-----------------------
-T-----w--
-w-------------
t
Norm.
I
Pre
I
I
Post- 1
Post-2
Figure 45. - Blood chemistry, chlorides,
Alamo Regional Race, August 16, 1964.
Pre
Post-l
Post-2
.
.-
_t
----,-----------------
Figure 46. -
Blood chemistry, phosphorus, Alamo Regional Race, August 16, 1964.
76

Urine excretion and chemistries - Austin (table 18).- Urine samples
were collected on four drivers. Two were followed throughout the day
for total excretion, excretion rate, glucose, and acetone concentrations.
The other two had single specimens collected. A urine sample was col-
lected on each driver and studied immediately on his return to the test-
ing area after active racing.
One driver, A, was unable to relate the time of voiding prior to
the first sample collected; therefore only the late morning and after-
noon specimens were considered in determining excretion rates. Over a
period of 6.6 hours, he excreted 160 ml of urine, an average excretion
rate of 24 ml per hour.
During the same time of day, but over a
7.8-hour period,
Driver B excreted 156 ml, an average excretion rate of
20 ml per hour.
This was a decrease from the 47-ml-per-hour excretion
rate observed in his first collection period. Similar low excretion
rates are indicated by the other two drivers who excreted 43 and 47 ml,
respectively, over a period tihich was probably greater than 2 hours.
The decrease in urine excretion rates correlates well with an ex-
pected decrease in ERPF and GFR along with an increased reabsorption.
This is probably in an attempt to conserve body water during periods of
excessive loss of water by perspiration.
Sugar and acetone concentrations were determined on each urine
ssmple collected.
Driver A had an increase in urine sugar concentration
with no increase in acetone. Driver B exhibited an increase in urine
acetone with no corresponding increase in urine sugar.
A moderate amount
of acetone was present in the post-race urine of one of the other drivers.
The other was essentially negative although in a previous race he had a
significant increase in urine glucose and is a known diabetic.
Although glucose and acetone are not normally present in the urine,
sufficient elevations in blood glucose concentrations were present, even
prior to racing, to have some "spilled" into the urine.
This
"spilling"
of glucose and acetone into the urine prior to racing is evident by
small amounts of each being detected in the first samples of urine col-
lected.
The result of body water conservation by the kidneys is the
production of a more concentrated urine. The concentrating effect may
have been sufficient to produce increased urine sugar and acetone con-
centrations.
77

TABLE 18.- URINE VOLUME AND CHEMISTRY STUDIES CONDUCTED ON DRIVERS
IN SPORTS CAR RACES AT AUSTIN, TEXAS, IN AUGUST%64
Driver
Time, hr Volume, ml
Volume/hr, ml
Glucose Acetone
Driver A -11:20 54 -- Trace Small
11:20-3:35 110 26 Trace Small
3:35-5:55 50 21 1+ Small
Totals": 6.6 160 Average 24
Driver B 6:30-9:40 150 47 Trace Small
9:40-2:50 ;: 19 Trace Small
2:50-5:30 22 Trace Moderate
-
Totals: 11 306 Average 28
Driver C -2~30 47 -- Trace Moderate
Driver D -10:55 43 -- Negative, Small
"The total time, volume, and average excretion rate is taken from the last two
periods.

Comment -on tilt table-testing
-.- -
- Austin, Texas (figs. 47 through 54).-
Figures 47 and 48:
These two records compare the cardiovascular
and vasomotor response after racing, with and without the cool suit.
Without the cool suit, the pre-tilt resting pulse rate fell from
175 to 130.
Then, on tilting up, it climbed to 174. This maintained
the systolic pressure at the level of 100 except for a momentary fall
to 80. Assuming some increase in cardiac output to maintain systolic
pressure, this is due, and possibly largely, to the increase in heart
rate rather than an increase in stroke volume.
On tilting back to
horizontal, a rise in systolic pressure
f?om
96 to 135 coincides with a
fall in pulse rate from
174
to 150, suggestive of an improved stroke
volume.
Diastolic pressure , pre-tilt, was-less than 40, and during the tilt
rose as high as 62.
The increase is small but firm, and on tilting back
to horizontal there is a decrease in diastolic pressure back to a low
of 30.
The principal evident response to the severe heat stress is the
heart rate ranging up to 180.
Nevertheless systolic, diastolic, and
pulse pressure are well maintained by this response together with an
effective peripheral vasomotor response.
By comparison, the tilt table test after racing, while wearing the
cool suit,
is much closer to the pattern of'a resting control.
On tilt-
ing up,
a pulse rate increase from 105 to
140
maintains a systolic pres-
sure level in the range of 100 to 120. Diastolic pressure rises during
the tilt from a low of 48 to a high of 84 and promptly falls on resuming
horizontal.
Figures 49 and 50 compare Driver A's tilt table response with and
without the use of the cool suit. The difference is striking but in a
different pattern than that of B in graphs 1 and 2. Pulse rate without
the cool suit rises from a resting 95 to 114 during the tilt and falls
as promptly to previous levels on tilting down. This maintains a sys-
tolic pressure between 150 and 170 except for a momentary dip to 122.
The small rise in pulse rate suggests an important increase in stroke
volume.
The resting diastolic pressure rises from 70 to the level of 100
with a peak at 132.
The principal feature is high systolic and diastolic pressure with
a rather narrow pulse pressure and relatively slow pulse rate.
With the
ice-coaled suit all elements are remarkably level. Pulse rate is level
at 120 to 140, appreciably higher than without the cool suit. Both
systolic and diastolic pressure are much more stable and pulse pressure
is particularly wide.
Both Drivers B and A demonstrated a more stable tilt table response
after wearing the cool suit,
than after racing without it.
79
Figures
51
and
52 compare Driver D in
tilt table tests, after
practice (lacking a resting control), and after
racing*
The post-race tilt table test shows a comparable pulse rate in the
vicinity of
140
maintaining a systolic pressure of 150 to
160,
as com-
pared to a systolic pressure of about 120 at lesser stress, post-practice.
The post-race diastolic pressure shows a swinging response with a rise
from 92 to 140 down to 104 and back to 132 before tilting down and re-
suming horizontal diastolic pressure at approximately
80.
The post-practice systolic, diastolic, and pulse pressure records are
much more stable.
Figure
53:
In a single tilt table test, post-practice, Driver C
(age 27) shows a rise in pulse rate from 114 to
180.
This maintains
systolic pressure at 120 to 140 and should mean very little change in
stroke volume.
A strong rise in diastolic pressure from
64
to a peak
of 124 indicates a strong 'peripheral vasomotor response and is respon-
sible for a very narrow pulse pressure during tilt.
Figure
54:
The single tilt table test of Driver E, done as a
pre-race control, is unusual in the rise of systolic pressure from
120 to
148,
and of diastolic pressure from
90
to a maximum of
118
during the tilt, with a pulse rate which levels off at 102. This should
indicate that an increase in cardiac output during tilt is dominantly
by stroke volume.
Driver E did not finish this race and his response
to stress must be obtained on another occasion.

20
-0
lown
II
8
Time in minutes
Figure 47. - Pulse rate and blood pressure during tilt-table testing.
81
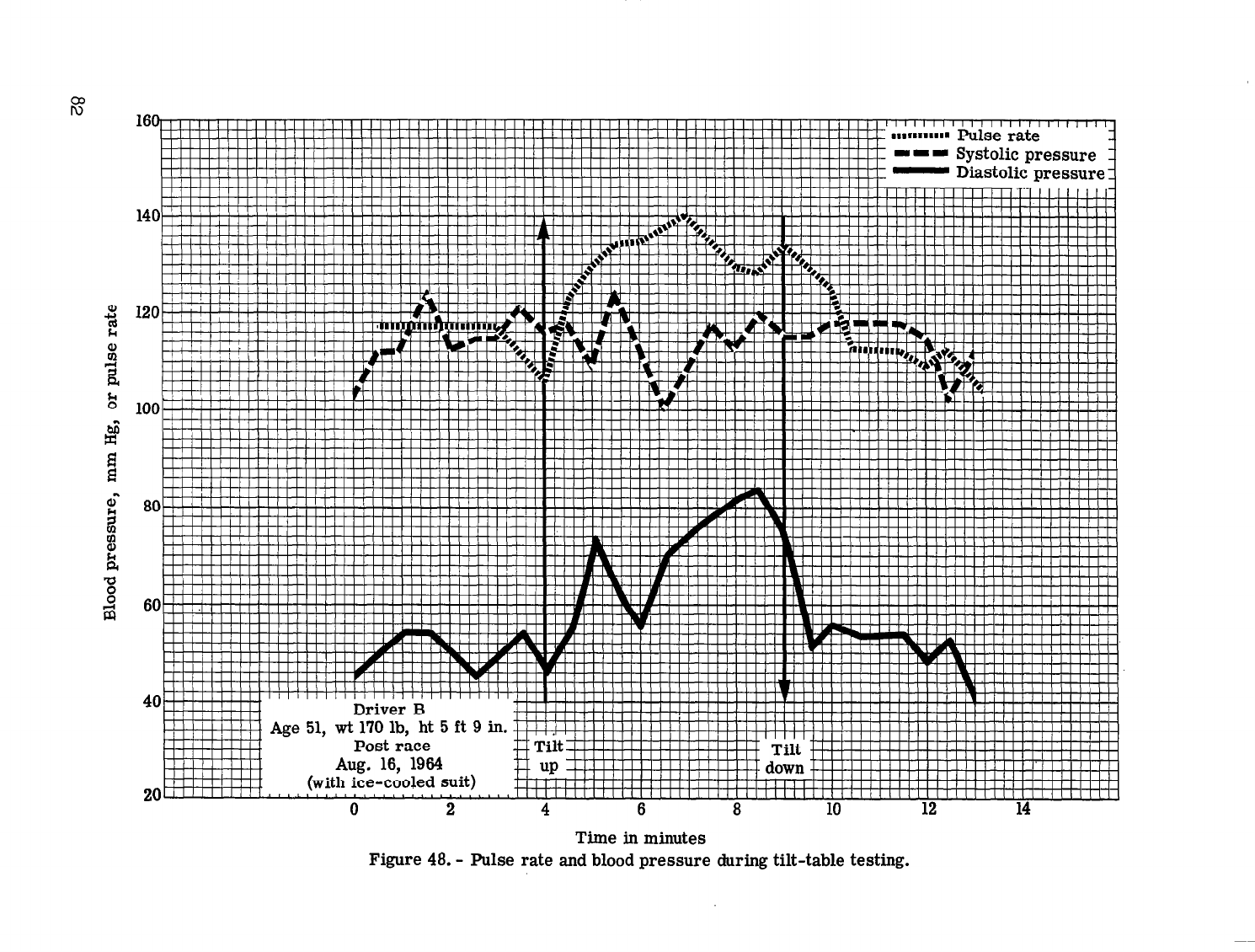
16
80
60
40
20
0 2 4
6 8
10
12 14
Time in minutes
Figure 48. -
Pulse rate and blood pressure during tilt-table testing.

180
80
60
0
2 4 6 8
10 12 14
Time in minutes
Figure 49. -
Pulse rate and blood pressure during tilt-table testing.

160
I I I Systolic pressure
--iA--
--
-y
-L---
_---
Time in minutes
Figure 50. -
Pulse rate and blood pressure tiring tilt-table testing.

160
20
0 2 4 6 8 10 12 14 16
Time in minutes
Figure 51. -
Pulse rate and blood pressure during tilt-table testing.

P
8
E
180
Pulse
I I I I I I I I I I 1-I I I I I I I I I I I I I I I
I I
I I I I I I I I I IJ mm- Sv&-Jic Dressure q
1601
140
120
100
I IIll III I II II/I I II II II/l 1
I I I , I I I I I I I I
III\ I III1 I I I I I I I I I I I III
III Ill II II I I III I IIll I III
80
60
-. -
Driver u
Time in minutes
Figure 52. -
Pulse rate and blood pressure during tilt-table testing.

I I I I , I I I I I I I I I I I I I I I I
I, I I,
I / I I I I I I
, I I I I I
I I I I
I I I I I I I
I I I
I I I I I I I I I I
I I I I I I
I III
I I I I I I I I I
” ” ” ” ” ” ” ” “I’ ” ” ‘I”” ” ” ” ” ” ’ ““I ” ” ” “““I’ ” ” ” ” ” ” ” ” ” ” ” ” ” ” ” ” ““I’ ’ I
0
2 4
6
8 10
12
14
Time in minutes
Figure 53. -
Pulse rate and blood pressure during tilt-table testing.

180
-J ------ =- ----_ -
-. .__ 1
IIlIIIIIIIlIlllllllllllllllllllIlIIIIIIIIlIlIIIIIl
I ,111 / I I / I I I I I / /a
2
a
‘5!
--
llllllllll’l’llllll’lll!ll’llllllllllllllllll~
I.IIIIIIlill
60
Pre-race control
40~,““““““““““““‘1”“““‘t
0
2
4 6 8
10 12 14
Time in minutes
Figure 54. -
Pulse rate and blood pressure during tilt-table testing.

In-race telemetry record of heart rate and temperature
(figs. 55 and 56).- Two graphs compare the in-race records of heart rate
and temperature of one individual (A), figure 55, without the benefit of
the "cool suit" and, figure 56, while wearing the 'jcool suit."
Roth tracings show the now familiar sudden acceleration in heart
rate at the instant starting of the race.
Without the ice-cooled suit
the rise is in the range of 120 to 170; heart rate is maintained at an
average of about 160 through the race;
at the finish of the race there
is a return to the pre-race level of 120 over a 4-minute period.
When.
the driver is wearing the ice-cooled suit the initial rise in heart rate
is from 130 to 180; the rate is maintained at an average of about 170;
at the end of the race there is a precipitous fall in pulse rate from
165 to 120 in approximately 1 minute.
Without the benefit of the cool suit the pulse is maintained at
about 10 beats per minute lower.
One observation does not justify a
conclusion, but the heart is bearing a greater burden of body cooling.
The sudden decrease in heart rate at the finish of the race may in-
dicate that no oxygen debt was incurred by the degree of physical exer-
tion required for racing.
Recovery is slower when the driver is not
protected from heat by the ice-cooled suit. This may reflect a greater
fatigue under this condition.
Without the cool suit, temperature rose from 99.5" to 101" F dur-
ing the first 10 minutes of the race and was maintained at this level
for the duration.
Wearing the cool suit, the driver's temperature rose more gradually
from 99.5" to 101" F over a period of 15 minutes.
89

0
5 10 15
20 25
Time in minutes
Figure 55. -
Pulse rate and body temperature.
103
102
101
100
99
98

llIlllilll/IlilllilIIIliliililiilIIlilllllIlIlllIllIlIIlllllillllilllllllllilllllllllllllllllllllll
I’ ---Pulse rate
- Body temperature
103
102 tg
G
lo1 :
%
98
-5
0
5 10
15
20
Time in minutes
Figure 56. -
Pulse rate and body temperature.

HOUSTON SPORTS CAR RACE, OCTOBER 1964
Tilt table tests - Houston Race, October .1964.- Figures 57 through
65 show tilt table tests of six indiqduals including 'a 21-year-old
woman driver.
All can be considered as within the range of variation of
satisfactory responses.
The first, a 23-year-old'man (fig. 57.) shows a wide pulse pressure
maintained through the tilt.
Systolic pressure is maintained at about
140 with a rise in pulse 'from 100 to a maximum of 120. Diastolic falls
gradually within the period of tilt from 80 to 50 with only slow recovery
during the post-tilt record.
The second, a 29-year-old man (fig. 58) shows a mild narrowing of
pulse pressure during tilt due to maintenance of a relatively level
systolic pressure with a 'rise in diastolic pressure.
The systolic pres-
sure is maintained by a rise of pulse rate from,84 to 114. Post-tilt
there is an increased.pulse-pressure due to a continuance of a slightly
high systolic pressure and slightly lower pulse pressure.
The third subject (fig. 591, a 21-year-old woman maintains a virtu-
ally level systolic and diastolic pressure with a rise in pulse rate
from 110 to 120 during tilt. Post-tilt there is a tendency toward fall
in systolic pressure, diastolic pressure, and pulse rate, and a slight
increase in pulse pressure.
The fourth subject (fig.
60) a 24-year-old male shows a narrowing
of pulse pressure due to an initial sharp fall in systolic pressure with
a gradual recovery and an initial rise in diastolic pressure. which grad-
ually falls off.
Pulse rate during tilt rises from 115 to 130 but
following tilt shows a precipitous fall to below pre-tilt levels.
At this time none of these subjects had control resting tilt table
tests.
The fifth subject, a.51-yeas-old male,
is presented with two controls.
In the post-race tilt (fig. 61) there is a sharp drop in systolic pres-
sure with a gradual recovery associated with a rise in pulse rate from
105 to 120.
Diastolic pressure shows a slight but definite rise during
tilt and then resumes the previous level.
Two resting controls (figs. 62 and 63) are similar to each other in
pattern but differ from the post-race pattern. Instead of the precipi-
tous drop in systolic pressure on tilting up, both show a prompt rise in
systolic pressure of 25 to 30 mm Hg associated with an increase in pulse
rate of about 30 pulses per minute.
The diastolic pressure shows a com-
mensurate rise during tilt to maintain an essentially stable pulse pres-
sure during and after tilt.
The sixth subject, a 24-year-old male, has both control and post-race
tilt table tests (figs. 64 and 65).
92

In the control there is a slight rise in systolic and diastolic
pressure with little change in pulse pressure. Pulse rate shows an in-
crease in the range of
75
to 95. In the post-race tilt table test,
there is a slight fall in systolic pressure (150 to -130) and a moderate
rise in diastolic pressure
(80
to 110) with some narrowing of pulse
pressure.
Pulse rate increases in the range of
85
to
115.
Control testing tilt table tests are clearly necessary to recognize
the influence of stress and these are being filled in during the present
season.
93

Driver A
Age 23, wt 165 lb, ht 5 ft 7 i in.
I I I I I I I I I I I I I I I I I
I
I
L
- - - Systolic pressure
~!!l!l!lll!!ll!l!ll1!!!!1!!!!!!!!!!!11IIIIIIIII ~-Diastolicpressure
IIIIIIIIIII Pulse rate
/ / / Estimated data
---
--
---
-li-7
---
mm-------
-------,
Time in minutes
Figure 57. -
Pulse rate and blood pressure during tilt-table testing.

-
-
I - I Systolic pressure 1
- Diastolic pressure 1
/ / / Estimated data
z
Time in minutes
Figure 58. -
Pulse rate and blood pressure during tilt-table testing.

-----_----
-~----
---
--
--
--
----,-
---AI-
---
fjO~~-v--.m----
---
---
--------s-P----
-
---
-
40-,‘,‘,“,,‘,,““‘.““, “’
0
2 4
6
8
10
12
14 16
18
Time in minutes
Figure 59. - Pulse rate and blood pressure during tilt-table testing.

---
I I I 8 4
~IIII~III~~ pulse rate
- - - Qyr=+filic pressure
II- VJYC”
160
t
,
- :‘. ‘,
: ‘,
I ! I I I I
I : i ! II 1 ! j I I I II I I I
III! f,Il!I
80
60
0 2 4 6 8 10 12 14 16 18
Time in minutes
Figure 60. - Pulse rate and blood pressure during tilt-table testing.
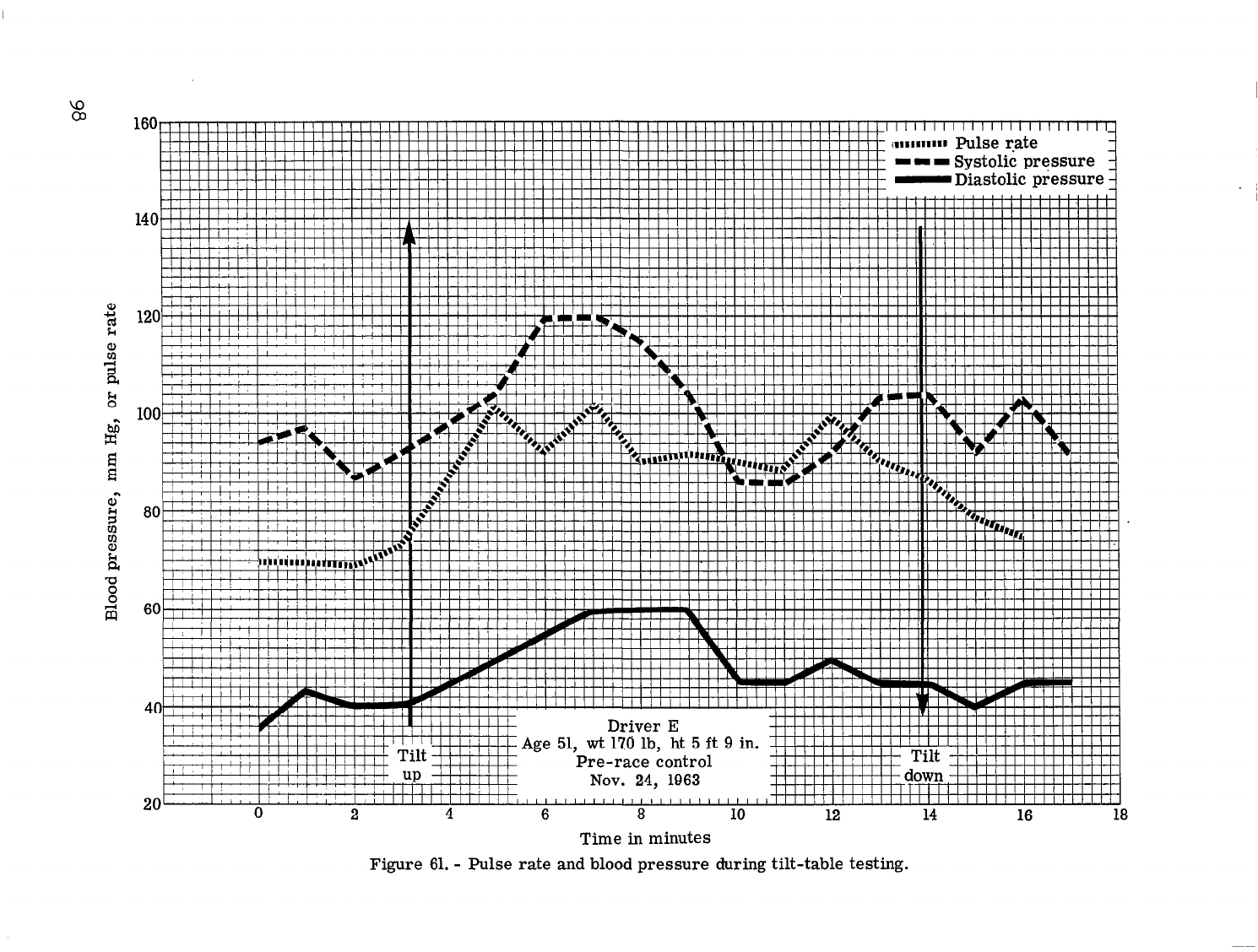
160
Il’lI”lII llll’llllllllllllllilllllllll’llll~Illlllllllllllllllllllllllllllllllll1lllll
80
I I i i i i i i i i i i i i I
60
I’m pfj-pfJ -
.Pre-race control
I !
2
4
6
8
10
12 14
16
18
Time in minutes
Figure 61. - Pulse rate and blood pressure during tilt-table testing.

180
160
140
120
100
80
60
40
0 2
4
6
8
10
12
14
16
18
Time in minutes
Figure 62. -
Pulse rate and blood pressure during tilt-table testing.

180
I i i i I I I I I P
IAge 51, wt 170 lb, ht 5 ft
9
in.
Post race
Oct. 11, 1964
40 ’ I I I ’ I I I ” I I I I I I ” ” I
”
’ ”
0 2
4
6 8
10
12
14 16
18
Time in minutes
Figure 63. -
Pulse rate and blood pressure during tilt-table testing.

I I I Systolic pressure
i--
100~~, --
~-
--
--
80
60
40
20
0 4 8 12 16 20
Time in minutes
Figure 64. -
Pulse rate and blood pressure during tilt-table testing.
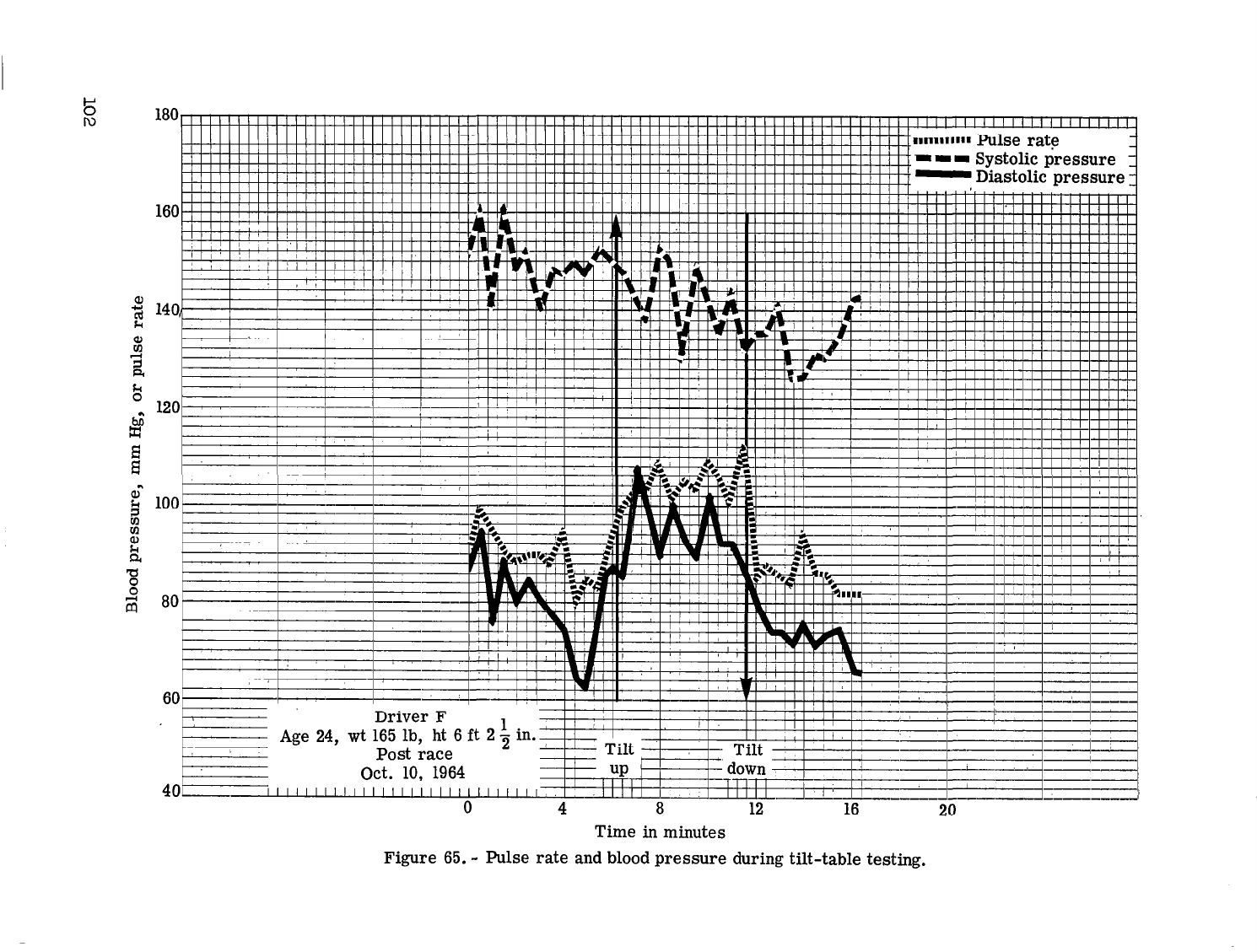
I
0 4
8
12 16
20
Time in minutes
Figure 65. -
Pulse rate and blood pressure during tilt-table testing.

In figure 66 heart rate is monitored during a-race by an in-car tape
recorder. The ECG signal is recorded.and at a later time reaaout as a
cardiotachometric tracing to permit recognition of rapid changes in
heart rate.
The recording shows an abrupt increase in heart rate from 140 to
180
beats per minute at the start of the race (1). This is maintained until
a minor accident (2) damages a wheel, necessitating.a slower pace. As
the driver continues at .reduced speeds, and no longer in competition, the
heart rate slows. A second accident
(3)
removes the two leading cars
from competition and, with the prospect of winning or placing restored,
speed is increased and heart rate obediently rises.
At the end of the
race (4) the heart rate abruptly falls.
An in-race heart rate of the order of
180
is commonly recorded and
there are frequent examples of over 200. This is of particular interest
since the physical exertion involved in driving is far below the level of
energy expenditure which in a runner might predictably evoke such rate.
It may be deduced that this rate is not due to oxygen consumption and
that cardiac output is not greatly increased.
That no oxygen debt accrues
is suggested by the sudden decrease in rate at the end of the race. A
question that arises as to what purpose is served by such increase in
heart rate. The answer may be sought in comparing the heart rates of a
large group of drivers and relating this to the variables of age, phys-
ical condition, experience, and performance.
It may not be assumed that
lower rates are optimal without consideration of performance, which must
be evaluated at the next stage in this investigation.
103

speed reduced.
3. Two leading cars damaged
and out of competition.
Speed increased.
4. End of race.
Time in minutes
Figure 66. -
Pulse rate history during race.

-
T
Driver
Driver A
Driver B
Driver C
Driver D
Driver E
Driver F
TABLE 19.-
VITAL STATISTICS OF SUBJECTS IN RACES AT HOUSTON, TEXAS, IN 1964
Physical description
Weight
165
130
180
160
170
165
Height
5 ft 7 l/2 ir
5
ft
6 in
5 ft 11 in
5 ft 9 in
5 ft 9 in
6
ft
2 1-12
ir
ke
-
23
21
29
24
51
24
-
J
Occupation
Student, car
sales
College student
Electrical
draftsman
Salesman
M.D.
Circuit eng.,
college stu-
dent
lilarital status
and
no.
of children
No
Yes
no children
Yes
4 children
Yes
no children
Yes
3 children
Yes
no children
Education
Student, Jr.
Math. major
Trade school
some college
M.D., L.L.B.
Attending colleg'
Racing experience
Three
Sports
Sports
Sports
sports
No. of
years
3 l/2
Less thar
lYr
1 yr
4 yr
3 yr
Rest prior
to race
6 hr sleep
8 hr sleep
6 hr sleep
4 l/2 hr
sleep
5 hr sleep

TABLE 20.-
BLOOD-CHEKIXCRY STUDIES CONDUCTED ON DRIVERS
IN THE RACES AT HOUSTON, TEXAS
Driver Glucose
I
Cholesterol
I
Uric acid
I
Creatinine
1
Chloride
I
Phosphorus
I
Driver C
Pre-race
Post-race
76
200
114
192
;:‘6
1.5
1.5
2.3
2.4
Driver D
Pre-race
Post-race
76
252
74 252
?;
.
1.2
1.0
3.0
2.5
Driver F
Pre-race
Post-race
56
270
5.5
1.0
71
288 6.0
1.2
117
140
I
109
109
114
110
2.3
2.5
Glucose -
Pre-race values two drivers were low normal and one was below normal.
Post-race,
one was elevated to upper limits of normal and two were in
normal range.
Cholesterol
- No significant changes occurred during the race. One driver's
cholesterol levels were above normal.
Uric acid - The
pre-
and post-race uric acid concentrations were within normal
limits.
Chlorides - Pre-race values of ‘all three drivers were just above normal.
Only
one driver showed a 20 percent increase during the race; two showed
no change.
Phosphorus - The pre-race levels were at low normal or below normal and were
essentially unchanged after racing.

SUMMARY
The field of sports presents a broad opportunity for physiologic
observations under conditions of physical and mental stress that vary
greatly with the particular type of activity. Competitive auto racing
has certain distinctive characteristics that lead to initiating this
investigation.
(1) There is an environment of stress involving only moderate phys-
ical exertion but a relatively h,igh element of danger.
(2) In this environment the individual must exercise mechanical con-
trol of a vehicle and judgment-as to factors of motion, speed, and dis-
tance that are acquired skills far removed from instinctive or reflex
responses that are utilized in other stressful sports.
(3) There is an element of motivation to aggressive action, which
cannot be simulated under laboratory conditions, that may influence re-
sponses and performance.
(4) It is considered that these factors simulate in some degree
the stress environment of space flight, particularly on launching or re-
entry.
The present investigation explores a variety of physiologic re-
sponses to this particular type of environmental stress as the first of
two parts of the total study.
The importance of the study lies in how
alterations in physiologic status may alter performance. The evaluation
of performance is the second part of the study presently in the planning
stage.
In field research of this type there is a tenuous control of
strongly individualistic subjects, race cars operating beyond intended
capabilities, and laboratory equipment exposed to the elements.
The ques-
tions revealed in these circumstances may be studied more meticulously
at a later date in the controlled environment of the laboratory.
The study includes observations on four auto races during
1964
(Daytona,
Galveston, Austin, and Houston), and 29 subjects, some of whom
have participated more than once.
Tilt Table Tests
Tilt table tests were obtained on 29 individuals immediately after
racing, sometimes more than once. Where possible, resting controls were
obtained prior to or after race day;
where controls are missing they may
still be obtained when opportunity presents.
The stress of auto racing induces changes in the pattern of the tilt
table record which vary in magnitude and type.
107

Patterns encountered among tilt table test subjects:
(1) Decrease in both systolic and diastolic pressure:
Driver A Figure 57
Driver B Figure 12
Driver C Figure 13
Driver D
Figure 22
Driver I Figure 14
Three of five (C, I, and B) showed an increase in heart rate of over
30.
All of these were after stress and Drivers D and C showed syncope.
It is observed that whenever diastolic pressure falls, systolic
pressure also falls.
This apparently indicates a failure or inadequate
response of peripheral vasomotor reflex construction with pooling in
dependent spaces.
Diminished venous return to heart would preclude an
increase in cardiac output.
This must be overcome or syncope occurs as
it did in three of these subjects, D, C, and I.
(2) Decrease in systolic pressure and increase in diastolic pres-
sure:
Driver A
Driver B
Driver B
Driver D
Driver D
Driver F
Driver F
Driver H
Driver I
Driver I
Driver J
Figure 10
Figure 63
Figure 47
Figure 38
Figure 60
Figure 37
Figure 65
Figure 32
Figure 30
Figure 31
Figure 36
This is the common post-race pattern apparently showing a stress
effect adequately compensated by a strong peripheral vasomotor reflex
constriction of the capillary bed.
Only Driver I showed the drop in
systolic pressure in his control tilt and this may be related to his
bizarre post-race tilt record with a remarkably narrow pulse pressure.
(3) Increase in both systolic and diastolic pressure:
Driver A
Driver B
Driver C
Driver D
Driver E
Driver E
Driver E*
Driver E
Figure
9
Figure 35
58
Figure
Figure 52
Figure
62
Figure
61
Figure 21
Figure
54
Driver F*
Driver G*
Driver H
Driver H*
Driver J*
Driver K*
Driver L*
Figure 15
Figure 17
Figure 33
16 Figure
Figure 18
Figure 20
Figure 19
108

This is presumed to represent the optimum tilt response and the
most effective effort to maintain cerebral circulation by increased
cardiac.output and by peripheral vasomotor reflex constriction and ade-
quate venous return. It is notable that all the.professional race car
drivers* fall in this category.
(4) Ten individuals. showed a moderate to marked decrease in pulse
pressure:
Driver A
Driver B
Driver C
Driver C
Driver D
Driver D
Driver E
Driver I
Driver I
Driver J
Figure 10
Figure 12
Figure 53
Figure 13 syncope
Figure 52
Figure 22
Figure
syncope
34
Figure 31
Figure 14 syncope
Figure 36
A prominent decrease in pulse pressure may call for a more thorough
investigation of the individual's cardiovascular status.
Driver I's ex-
tremely narrow pulse pressure, post-race,
is unique in this series.
Driver D has been treated for hypertension and diabetes. Drivers C and
E are very young individuals in apparent good health but both are partic-
ularly tense and responsive to their environment.
Drivers C, B, and J
tend toward overweight.
Driver A is of American Indian stock, slender,
wiry and calm in manner.
(5) Heart rate:
The range of increase in heart rate on passive tilt to the ortho-
static position in 40 tests on 26 subjects, ranged from 0 to 68, with a
mean of 27.
A correlation was sought with age or apparent physical con-
dition but no evident relationship was found. Initial heart rate in the
recumbent position before tilting was not consistently related to in-
crease in heart rate on passive tilt.
Of individuals with an initial
rate of less than 90, five of seven showed an increase above the mean.
Of individuals with an initial rate between 90 and 150, 16 of 31 had an
increase above the mean.
Two individuals with an initial rate over 150
had increases above the mean.
Of those subjects with control tilts (E,
I, F, B, and A) all but one showed a higher heart rate in the recumbent
position after stress than in the resting control, and a greater in-
crease in heart rate on tilting after stress than in the control.
109
There were 10 tilt tests in which the systolic pressure showed a
fall.duri,ng passive tilting. All but one of these showed an increase
in pulse rate during tilting which tias less than the mean.
There were 14 subjects who showed sn increase in systolic pressure
during passive tilt.
This was always associated with an increase in
diastolic pressure.
These subjects uniformly showed an increase in
pulse rate during tilting which was greater than the mean.
In-Car Recordings
The in-car recordings of electrocardiogram and temperature obtained
at Daytona are in the hands of NASA personnel.
This report contains the in-car records of three subjects E
(fig. 39), A, with and without the cool suit (figs. 55 and 56), and E
(fig. 66).
The dominant features of interest are the instantaneous rise at the
start of a race to levels of 169 to 183 beats per minute. This level
tends to be maintained during races lasting up to 30 minutes and then
falls almost as suddenly to pre-race levels. Although driving is mod-
erately strenuous exertion,
it is not such as to greatly increase oxy-
gen consumption and the purpose served by the high pulse rate is not
clear. It may be explained as anticipatory but is more prolonged than
is expected on this basis. Oxygen consumption studies during this type
of driving would be feasible for a trained individual and would be of
interest in explaining this phenomenon.
Observations on one individual racing in summer heat with and with-
out the cool suit show suggestive changes indicating diminished fatigue
with cooling. This portion of the study should be extended to more
individuals and for
more
protracted events so that the difference in fati-
guability might be more clearly demonstrated.
Blood and Urine Studies
Blood chemistries included glucose, CO2 combining power, LDH, urea
nitrogen, cholesterol, SGOT, SGPT, uric acid, creatinine, chloride, and
phosphate. Of these serum glucose may be of greatest importance because
of the possible influence of hypoglycemia on performance.
In short races
(fig. 24(a) and 24(b)),
a duration of the order of 30 minutes, there
was consistent elevation of serum glucose.
This is explicable on a basis
of mobilizing of glucose stores.
In endurance races where driving-stress
is of 2 hours duration or more, the trend is toward a decrease in serum
glucose post-race. This may be au@plented by irregular eating habits
110

I--
under the .existing conditions.
One individual (C, fig. 2(b) who showed
only a moderate drop in serum glucose during two races, (fig. 3(a) and
3(b)), had an episode of weakness and fainting at his hotel about 2 hours
after the race.
The clinical features were compatible with the hypo-
glycemic episode and he was revived with available carbohydrative fluids
without an opportunity to. obtain a blood sample.
CO2 combining power closely parallels the observations on serum
glucose.
Creatinine is the only other blood chemistry of apaarent signifi-
cance in this study (fig. 27(a) and 27(b)).
There is consistent trend
to increase during stress.
It is not suggested that the increase is
directly related to stress,
but rather that it may indicate alteration
in renal blood flow, since creatinine is cleared by the kidneys but not
subject to tubular reabsorption.
In continuing studies where heat is an important factor, sodium and
potassium values are important but rigid control of fluid and salt intake
and close observation of fluid loss as reflected in body weight change
are necessary.
This is difficuft under field conditions except for a
limited number of closely controlled subjects.
Urine chemistry determinations included sugar, acetone, sodium, po-
tassium, and osmolality.
There were urinary sugar determinations on
16
subjects with pre-
and post-race samples in 14 subjects.
Of a total of 30 specimens
28
showed a trace or more of sugar.
Of 14 subjects with pre- and post-race
samples, 7 showed an increase, 4 were unchanged, and
3
showed a decrease.
No significance can be attributed to these findings since the intake of
food and fluid was uncontrolled.
In four individuals with pre-
and post-race determinations all
showed a diminished urinary sodium post-race, and three of four showed
an increased urinary potassium (table 13). This correlates with the re-
tention of chloride in blood (fig. 28(b)).
Osmolality of the urine was
determined pre- and post-race. The elevated values obtained indicate an
attempt to conserve body water probably by a decreased effective renal
plasma flow or a high reabsorption of water in the renal tubules.
The
high pre-race values are probably a reflection of the samples being taken
after the morning practice.
111

Blood Volume
Blood volumes by the RISA technique were
done
in association with
passive tilt.
Two values were obtained, one recumbent prior to tilt,
and one in the orthostatic position.
In two subjects during the control
study,
a third value was obtained on return to the recumbent position.
In two control tilt studies,
one of the two subjects showed a de-
crease in the calculated blood volume which returned to above normal
upon again assuming the recumbent position.
In post-race tilt studies
8
of 10 subjects showed a decrease in calculated blood volume presumably
due to exclusion of pooled blood from the measured circulating blood.
The two subjects having an increase in calculated blood volume also
showed an increase in red cell mass.
The source of this increase in red
cells is not known.
Two subjects were lost to the study due to development of syncope
while in tilt.
The changes in blood volume recorded in tables 6 and
7
are
summarized:
Number of
Due to Due to red
studies plasma
cell mass
Control studies
(1) Blood volume increase on
tilting up
0
(2) Blood volume decrease on
tilting up
1
(3) No change
1
1
Post-race studies
(1) Blood volume increase on
tilting up
2
2
(2) Blood volume decrease on
tilting up
8
7
1
(3) No change
0
The further investigation indicated is to seek a correlation between
blood volume and hematocrit changes and the maintenance of diastolic
pressure in passive tilting.
112

CONCLUSIONS
(1) Competitive.aut.0 racing provides an opportunity for studying
the physiologic effects of stress which .differ from most other sports in
that there is an element of risk of injury and avoidance is by a learned
manipulative skill which is not served by the fight or flight mechanisms
of instinctive reflex responses.
(2) The passive tilt test is a useful index of alteration in cardio-
vascular responses following stress.
Three patterns are discerned:
(4
a temporary fall in systolic pressure with a rise in
diastolic pressure,
b)
a rise in both systolic and diastolic pressures, and
(cl
a fall in both systolic and diastolic pressures.
It appears that if diastolic pressure falls, systolic will also fall. If
systolic pressure rises,
diastolic will also rise. However a rise in
diastolic pressure is not necessarily associated with a rise in systolic
pressure;
a fall in systolic pressure is reversed if diastolic pressure
increases.
This suggests that peripheral vasomotor constriction is the
essential feature in maintaining an adequate venous return to heart, an
adequate cardiac output,
and an adequate blood supply to brain.
A greater number of subjects with repeated examination along with
more sophisticated analysis might determine whether the individuals are
characterized by varying adequacy of their peripheral vasomotor responses.
(3) In-race recording of ECG shows a prompt and marked increase in
heart rate coinciding sharply with the beginning and end of a race.
Variations during a race are apt to be related to incidents increasing
or decreasing stress.
A greater number of such in-race recordings is necessary to show
individual patterns of response as to magnitude of increased heart rate,
range of variation, and recovery.
(4) Of blood chemistries,
the serum glucose is most labile under
the conditions of this investigation and may be a sensitive index to
stress and an important influence on performance.
CO2 combining power
closely parallels serum glucose.
Creatinine was the only other serum
chemistry showing a consistent change. It may indicate a decreased renal
blood flow during stress.,
I-..

Of~urine'chemistries, the'only.notable finding is the consistent
spilling of.sugar but the significance is unknown under the varying-con-
ditions of food ingestion and fluid balance.
(5)
Blood volume determination on passive tilting tends to show a
decrease due to an apparent decrease in plasma volume.
Less commonly,
blood volume may show an increase on tilting up and this is due to an
apparent increase in red cell mass.
On resuming recumbent position after
tilt, blood volume of two subjects shows an increase, presumably due to
return of pooled blood.to the general ci&ilation and some augmentation
of either plasma volume or red cell mass.
The interrelation of altera-
tion in blood volume and hematocrit values with peripheral vasomotor
constriction and maintenance of diastolic pressure in passive tilting,
should be studied further.
114
NASA-Langley, 1966
CR-570

:: . .
NASA SCIENTIFIC AND TECHNICAL PUBLICATIONS
: ‘i
“, :. .
1
“The aeroxaufical and space arIivities of ihe Unded Sfates shall be
conducted JO as to contribute . . . to the expansion of hzcman know/-
edge of phenomena in the atmosphere and space.
The Administration
shall provjde for the widest practicable aud appropritite dirsemination
of information concerning it, activities aqd.the resrh thereof .I’
,)
-NATIONAL AERONAUTICS AND SPACE ACT OF 1958
i
-:
: :’
.: ,
,
-1
.’ ’
, : .
. i*’
TECHNICAL REPORTS: Scientific and technical information considered
important, complete, and a lasting contribution to existing knowledge.
TECHNICAL NOTES:
Information less broad in scope but nevertheless
7 of-importance as a contribution to existing knowledge.
D .J
V
TECHNICAL MEMORANDUMS: Information receiving limited distri-
bution because of preliminary data, security classification, or other reasons,
CONTRACTOR REPORTS: Technical information generated in con-
nection.with a NASA contract or grant and released under NASA auspices,
-
TECHN,&AL TRANSLATIONS: Information.‘published in a foreign
language considered to merit NASA distribution in English.
..
‘...
-
‘_
TECHNICAL REPRINTS: Information derived from NASA activities
and initially published in the form of journal articles.
SPECIAL PUBLICATIONS: Information derived from or of value to
NASA activities but not necessarily reporting the results .of individual
NASA-programmed scientific efforts.
Publications include conference
proceedings, monographs, data compilations, handbooks, sourcebooks,
and special bibliographies.
:’ :;
Detail; on
the
availability
of these
publications
may
be obtained
from:
SCIENTIFIC AND TECHNICAL INFORMATION DIVISION
:
t
NATIONAL AERONA-U’TICS AND SPACE ADMINISTRATION
Washington, D.C.
20546
