
Developed by OrthoVirginia Sports Medicine Physician Committee
ORTHOVIRGINIA.COM
Anterior-Cruciate
Ligament
Reconstruction Protocol
TABLE OF CONTENTS
Early Post-Op Restrictions ........................................2
Preoperative Rehabilitation Phase ............................2
Postoperative Phase I: 0-2 Weeks .............................3
Postoperative Phase II: 2-4 Weeks ............................4
Postoperative Phase III: 4-6 Weeks ...........................5
Postoperative Phase IV: 6-12 Weeks .........................6
Postoperative Phase V: 3-4 Months ...........................7
Postoperative Phase VI: 4-6 Months .........................8
Postoperative Phase VII: 6-9 Months ........................9
Appendices .................................................................10
ACL Scorecard............................................................12

ORTHOVIRGINIA.COM
Early Post-Op Restrictions
PATELLAR TENDON GRAFT
Follow protocol as outlined below.
QUAD TENDON GRAFT
Follow protocol as outlined below.
HAMSTRING GRAFT
No resisted hamstring for 8 weeks.
ALLOGRAFT
Brace is worn for 10 weeks with ROM 0-90
PWB at 30% for 0-4 weeks
WBAT for 4-10 weeks
MENISCUS REPAIR
Knee ROM 0-90 for first 4 weeks. Please refer to
MD order for repair type and weight-
bearing status for the first 6 weeks.
• For root repair or radial tear: non-weight bearing
(NWB) for 4 to 6 weeks (see MD referral),
brace locked in extension when not in therapy.
• For bucket handle, ramp lesion or partial tear
repair: Weight-bearing as tolerated (WBAT) (see
MD referral for any additional
precautions).
EXPECTATIONS FOR RETURN TO SPORT SHOULD BE NO SOONER
THAN 9 MONTHS POSTOPERATIVELY. THESE EXPECTATIONS
WILL BE PROVIDED ON AN INDIVIDUAL BASIS, THOUGH IT IS EXPECTED
NO SOONER THAN 9 MONTHS FOR BEST LONG-TERM OUTCOMES.
PHASE I:
Preoperative Rehabilitation
(3-5 Weeks Before Surgery)
REHABILITATION
GOALS
• Full knee extension range of motion
• Minimize/eliminate swelling
• Maximize muscular control around
knee (no knee extension lag with
straight leg raise)
• If above goals are met, patient will have
better chance to return to prior level of
function and normal knee function
INTERVENTION
• Passive knee extension exercise
• Passive knee flexion as tolerated
• Perturbation/proprioception training to
restore neuromuscular control
• Aggressive quadriceps strengthening
(quad set, SLR without lag, squats
(tolerated ROM), lunges, step-ups

ORTHOVIRGINIA.COM
POSTOPERATIVE PHASE I:
Immediate Post-Op (0-2 Weeks)
Frequency: 2-3 days/week
1st physical therapy session should be scheduled 2 days or next available date after surgery
REHABILITATION
GOALS
• Protect the reconstructed graft
• Manage inflammation: Ice,
Compression, Elevation (20 minutes
every hour with knee in extension)
• Restore patellar mobility
• Restore full passive knee extension
to 0 degrees
• Gradually increase flexion ROM
(0-90+ degrees)
• Re-establish quadricep control and
normalized ambulation
• Restore independent, normalized
ambulation with good swing phase
• Administer initial Knee Outcome
Survey-Activities of Daily Living (KOS-
ADLS)
WEIGHT-BEARING
STATUS
• Extension brace - locked into full
extension for ambulation and sleeping,
can be unlocked for sitting
• Axillary crutches - WBAT with 2
crutches
INTERVENTION
RANGE OF MOTION
- Heel slides
- Wall slides
- Stationary bike with no resistance
- Low-load long duration (LLLD)
stretches for extension as needed
(supine heel prop or bag hangs)
PATELLAR MOBILITY
- Medial/lateral/superior/inferior
patellar mobilizations at 0-30
degrees flexion performed by PT and
patient at home
QUAD ACTIVATION
- Quad sets (50-100 reps per day)
- Prone terminal knee extensions
(TKEs)
- Standing TKEs
- Long-arc Quad (LAQ)
(90-45 degrees) no resistance
(refer to MD protocol)
- Seated submaximal multi-angle
isometrics at 90 and 60 degrees
(against resistance)
- Step-ups
HIP STRENGTH
- Straight Leg Raise (SLR) 4-way
FUNCTIONAL TRAINING
- Pre-gait standing weight shifts
- Mini squats (0-60 degrees)
MODALITIES
- (NMES) to quads with blood flow
restriction (BFR) if tolerated and
incision is fully healed
- NMES guidelines: 10-20s on, 50s
off, 15 min total, 2 sec ramp,
recommend 60 degrees isometric at
edge of table
CRITERIA TO
PROGRESS
• Range of Motion: Knee full extension,
110 degrees flexion
• SLR 2x10 without quad lag to
DC extension brace
• Good patellar mobility

ORTHOVIRGINIA.COM
POSTOPERATIVE PHASE II:
Early Phase Post-Op (2-4 Weeks)
Frequency: 2-3 days/week
REHABILITATION
GOALS
• Protect the reconstructed graft
• No anterior knee pain during or after
exercise
• Restore full range of motion at the knee
(limit hyperextension past 5 degrees)
• Restore normal gait mechanics
• Restore reciprocal stair climbing
• DC brace with good quad control
• KOS-ADLS >65%
• Quad strength >60% of uninvolved side
WEIGHT-BEARING
STATUS
• Full weight bearing
• Wean from assistive device
• If still in brace, unlock to 80% of flexion
ROM for ambulation
• Avoid plant and pivot movements with
surgical limb
INTERVENTION
Include exercises
from previous
phases as needed
RANGE OF MOTION
- Heel slides
- Stationary bike
- Prone and seated leg hangs and/or
bag hangs
- Patella mobilizations, both in
extension and into flexion
- Scar mobilization
QUAD ACTIVATION
- Quad sets
- Prone TKE
- Standing TKE
- LAQ (90-45 degrees) no resistance
(refer to MD protocol)
- Seated multi-angle isometrics
against resistance
FUNCTIONAL TRAINING
- Step-ups/Stair climber
- Gait training
- Sit to stand
- Squats
- Hip hinging
HIP STRENGTHENING
- 4-way SLR
- Bridges
- Standing calf raise
- Leg press/total gym squat
CORE STRENGTHENING
- Planks, side planks
STABILITY
- DL and SL stable surface, focused
(no distractions)
AEROBIC CONDITIONING
- Cycling on stationary bike (Week 3)
- Treadmill walking with normalized
gait pattern (Week 3)
- Swimming, gentle flutter kick only
(Week 3)
- Pool walking, when incision is fully
healed
MODALITIES
- NMES: Russian stim for quad
activation with BFR for hypertrophy
- BFR: with stationary bike (unilateral
or bilateral), BFR with any exercise
with 30:15:15:15 rep scheme where
possible
CRITERIA TO
PROGRESS
• Overall the knee should be “Quiet,”
meaning the following:
• Full extension range of motion,
110 deg flexion
• Minimal effusion
(modified stroke test ≤2+)
• No joint line and anterior knee pain
• Normal gait pattern without crutches
• Normal functional activities: squat,
stairs

ORTHOVIRGINIA.COM
POSTOPERATIVE PHASE III:
Mid Phase Post-Op (4-6 Weeks)
Frequency: 2-3 days/week
REHABILITATION
GOALS
• Protect the reconstructed graft (graft is
weakest from 6-20 weeks)
• Continue with graded lower extremity
strength and neuromuscular control
programs emphasizing quads, glutes,
hamstrings, etc.
• Emphasize eccentric quad control and
force absorption in preparation for
eventual running
INTERVENTION
Include exercises
from previous
phases as needed
RANGE OF MOTION
- Tibiofemoral mobilization with
rotation if flexion is limited
- Stationary bike
QUAD
- Full LAQ as tolerated
(refer to MD protocol)
STRENGTHENING
- Hamstring curls as tolerated (unless
HS autograft, see first page of
protocol)
- Introduce hip hinge/deadlift with
kettlebell or trap bar
- Split squats
- 4-way SLR (add resistance)
- Bridges (progressions)
- Calf raises (progressions)
- Side step/monster walk
- Leg press (eccentric and/or SL)
- Core strengthening: planks, side
planks, bird dogs, modified
Copenhagens
BALANCE/PROPRIOCEPTION
- DL, SL, stable and unstable surface,
focused (no distractions)
FUNCTIONAL TRAINING
- Planks, side planks
STABILITY
- Squats (bilateral and unilateral)
- Stairs
MODALITIES
- BFR with any exercise with
30:15:15:15 rep scheme, bilateral or
unilateral cuff use encouraged
CRITERIA TO
PROGRESS
• Normal AROM or flexion within 10
degrees of contralateral side
• Quad strength ≥60% contralateral leg
with isokinetic testing, or with relative
1RM testing on leg press
• Minimal effusion (modified stroke test
≤1+)
• No patellofemoral pain or complaints
• Normal gait pattern and squat pattern,
no shifting away from surgical side

ORTHOVIRGINIA.COM
POSTOPERATIVE PHASE IV:
Mid Phase Post-Op (6-12 Weeks)
Frequency: 2 days/week and supplement 1 day of home exercise program (supplied by PT)
REHABILITATION
GOALS
• Emphasize strength in various planes of
motion for the lower extremity
• Continue with exercises noted from
previous phases, including quad
strength and motor control
• Administer initial KOS-SPORTS, TSK-
11, ACL-RSI
INTERVENTION
Include exercises
from previous
phases as needed
MOBILITY
- Restore lower extremity muscle
lengths
STRENGTHENING
- HS curls and deadlifts
- 4-way SLR with resistance
- Bridges (DL to SL progressions)
- Calf raise (DL to SL progressions)
- Side step/monster walk
- Leg press (eccentric and/or SL)
- Quad strengthening open kinetic
chain/closed kinetic chain
(OKC/CKC) (refer to MD script
for OKC guidelines)
o Leg extensions to tolerance
o Wall sits
o Squats
o Rear foot elevated split squat
(RFESS)
o Lunge progressions in multiple
planes
- Core strengthening: planks, side
planks, bird dogs, modified
Copenhagens
CARDIOVASCULAR/ENDURANCE TRAINING
- Treadmill walking (working up to
10-15 minutes at fast pace)
- Cycling with resistance
- Rowing
STABILITY
- DL and SL, stable and unstable,
some distraction (rebounder, body
blade)
FUNCTIONAL TRAINING
- DL hop, SL hop, jump landings, box
drops
MODALITIES
- BFR with any exercise with
30:15:15:15 rep scheme, bilateral or
unilateral cuff use encouraged
CRITERIA TO
PROGRESS
• Minimal to no effusion (modified stroke
test ≤trace)
• Normal ROM
• Strength ≥75% contralateral leg for
quad and hamstring
• Fast walking 10-15 min without pain or
increased effusion
FUNCTIONAL TESTING FOR
RETURN TO RUNNING
- Single leg squat test >85-90% LSI,
minimum of 10 repetitions each leg
- No effusion
- ROM ≥95% (must have full active
knee extension)
- 10-15 minutes fast treadmill walking
with normalized mechanics and no
patellofemoral symptoms
- Ability to single leg squat with
proper mechanics
- ≥70% quad/HS strength

ORTHOVIRGINIA.COM
POSTOPERATIVE PHASE V:
Late Phase Post-Op (3-4 Months)
Frequency: 1-2 days/week and supplement 1 day of home exercise program (supplied by PT)
REHABILITATION
GOALS
• Normalize strength, enhance muscular
power and endurance of the lower
extremity
• 1 RM on leg press >80% of uninvolved
side
• Improve neuromuscular control of the
lower extremity
• Emphasize functional strength and in
various planes of motion
• Initiate running progression
INTERVENTION
Include exercises
from previous
phases as needed
• Progress exercises from previous
phases as appropriate
• Exercises should be between 60%
(novice lifter) and 80% (experienced
lifters) of 1-RM
• Athletes should be aiming for
2-3 training sessions per week
• Training volume should be between
2-4 sets per exercises
FUNCTIONAL
- Bilateral and unilateral squats
- Lunge and hinge patterned
movements
STRENGTH
- Hamstring curls and deadlifts
- Bridges (progressions)/hip thrusts
- Calf raise (progressions)
- Side step/monster walk
- Leg press (eccentric and/or SL)
- Quad strengthening (OKC, CKC)
- Core strengthening: planks, side
planks, bird dogs
POWER
- Plyometric progressions
(double to single leg)
- Running progressions
(in clinic or at home)
CRITERIA TO
PROGRESS
• KOS-Sports ≥80%
• Normal running technique/form
• Asymptomatic knee with running
• Perform 10 consecutive single leg
squats with good form, while holding
>75% weight the athlete is able to
perform on uninvolved leg
• >85% Limb Symmetry Index (LSI) on
one-repetition maximum (1-RM) leg
press

ORTHOVIRGINIA.COM
POSTOPERATIVE PHASE VI:
Late Phase Post-Op (4-6 Months)
Frequency: 1-2 day/week and supplement 2-3 day of home exercise program (supplied by PT)
REHABILITATION
GOALS
• Development of lower extremity
muscular strength, power and
endurance preparing for eventual
return to functional and sport-specific
activities
• No compensations or side-to-side
differences with high-velocity
multiplane testing
• Continued aerobic conditioning and
core strength as needed for athletes
INTERVENTION
FUNCTIONAL
- Bilateral and unilateral squats
- Lunge and hinge patterned
movements
STRENGTH
- Hamstring curls and deadlifts
- Leg press (eccentric and/or SL)
- Quad strengthening (OKC/CKC)
- Core strengthening: planks, side
planks, bird dogs
- Hip thrusts
- Hip strengthening with focus on
preventing hip adduction with
landing
POWER
- Plyometric progressions
(double to single leg)
RUNNING PROGRESSIONS
(IN CLINIC OR AT HOME)
AGILITY
- Ladder drills (single plane)
- T-drills
- Reaction training
CRITERIA TO
PROGRESS
• Side plank abduction test >85-90% LSI,
minimum 30-second hold
• Y-Excursion limb symmetry
(90% or better)
• >80% LSI on 1-RM hamstring curl and
leg extension
• >80% LSI on peak torque testing with
isokinetic device or crane scale in clinic

ORTHOVIRGINIA.COM
POSTOPERATIVE PHASE VII:
Sport Preparation Phase Post-Op (6-9 Months)
Frequency: 1-2 days/week or every other week and supplement 2-3 days of home exercise program
(supplied by PT)
REHABILITATION
GOALS
• Prepare the athlete or individual for
functional demands of their respective
sport in a graded fashion
• Continue with lower extremity
muscular strength, power and
endurance training either in the clinic
or with a home program/with personal
trainer
• Continue with lower extremity
neuromuscular control training
• Athletes will begin progression to
return to sport during this phase.
Athletes will start with non-contact,
non-competitive drilling and progress
to full return to sports after 9+ months
of complete rehab
INTERVENTION
FUNCTIONAL
- Bilateral and unilateral squats
- Lunge and hinge patterned
movements
- Stepping exercises
STRENGTH
- HS curls and deadlifts
- Leg press (eccentric and/or SL)
- Quad
- Core strengthening: planks, side
planks, bird dogs
- Hip thrusts
- Hip strengthening with focus on
preventing hip adduction with
landing
POWER
- Plyometric progressions
(double to single leg)
RUNNING PROGRESSIONS
(IN CLINIC OR AT HOME)
AGILITY
- Cutting and pivoting
- Ladder drills
- T-drills
- Reaction training
CRITERIA TO
PROGRESS
STRENGTH
- Strength: 1RM testing on cybex knee
ext, flex and leg press calculate LSI.
Need a minimum of 90%
- Drop jump test
- Fatigue testing: drop jump test after
performing (1 min jumping jacks, 30
squat jumps, 1 min plank, 30 alt
lunge jumps)
- Hop testing: single, triple, crossover,
6 meter hop tests (>90% LSI)
- Using HHD or crane scale,
determine peak torque (>90% LSI)
EXPECTATIONS FOR RETURN TO SPORT SHOULD BE NO SOONER
THAN 9 MONTHS POSTOPERATIVELY. THESE EXPECTATIONS
WILL BE PROVIDED ON AN INDIVIDUAL BASIS, THOUGH IT IS EXPECTED
NO SOONER THAN 9 MONTHS FOR BEST LONG-TERM OUTCOMES.
ORTHOVIRGINIA.COM
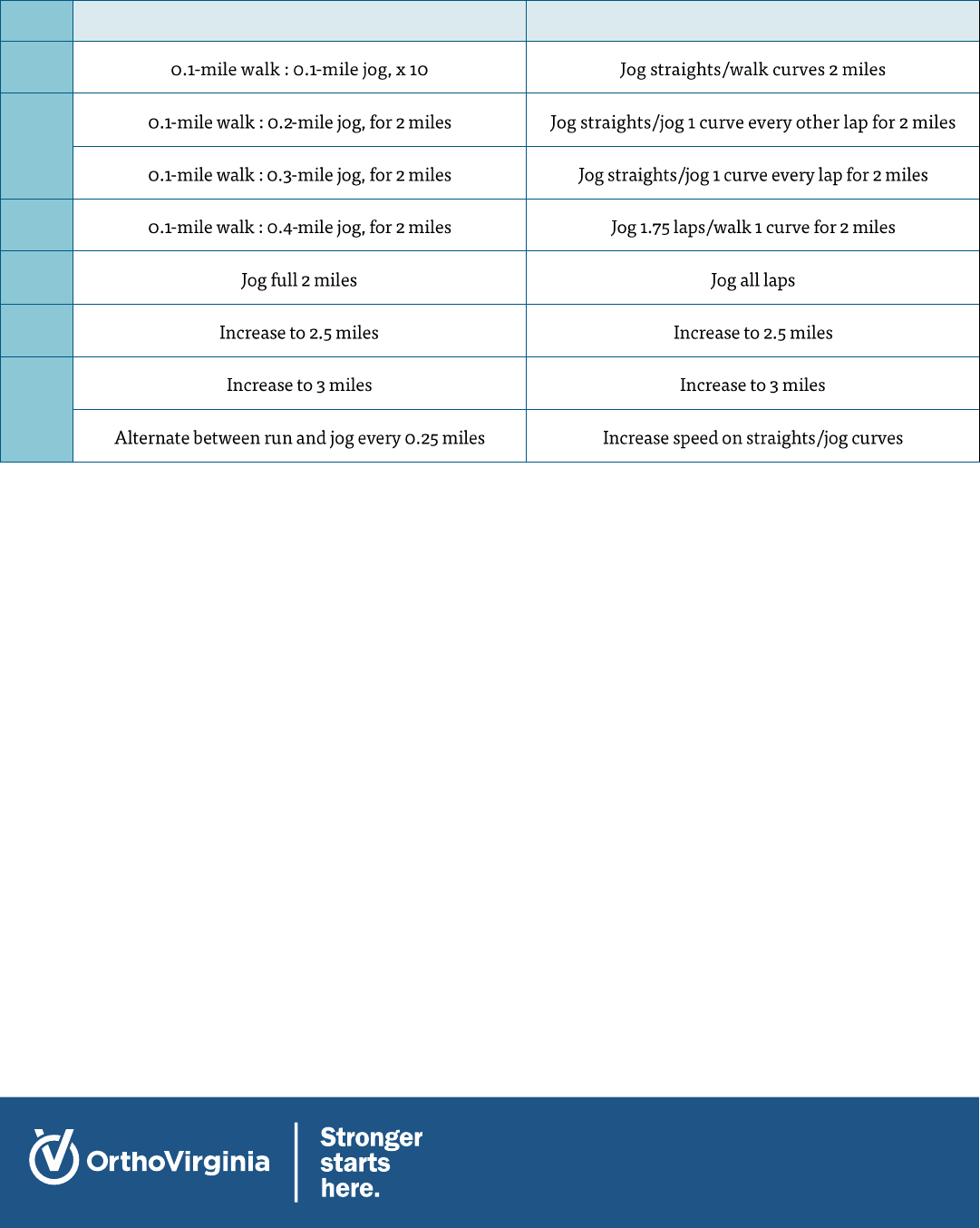
Appendices
Return to Running Progression (between 12-16 weeks if cleared)
LEVEL
TREADMILL
TRACK
1
2
3
4
5
6
7
8
RECOMMEND THE PATIENT START JUMPING IF THEY
ACHIEVE (SEE ATTACHED SCREENING TESTS):
• 10-rep max on the leg press was ≥85%
• 10 consecutive single leg squats to 60 degrees without
loss of balance or excessive motion outside of the
sagittal plane while holding ≥85% extra weight
(dumbbells, weight vest, etc.)
• No compensation patterns with deceleration during
agility drills performed at 100% effort
RECOMMEND THE PATIENT BEGIN HOPPING
AND CUTTING IF THEY ACHIEVE (SEE ATTACHED
SCREENING TESTS):
• 10-rep max on the leg press was ≥90%
• 10 consecutive single leg squats to 60 degrees without
loss of balance or excessive motion outside of the
sagittal plane while holding ≥90% extra weight
(dumbbells, weight vest, etc.)
• No display of genu valgum when loading into or
landing from jumps, and equal weight distribution
when initiating and landing the jumps

ORTHOVIRGINIA.COM
Appendices
RETURN TO SPORT TESTING INSTRUCTIONS:
1. Single Leg Forward Hop
Starting at a designated line, the patient will balance on one
leg and hop forward as far as possible, landing on the same
leg. The patient must maintain their balance. To pass, the
involved leg must measure at least 90% of the distance
compared to the uninvolved leg.
2. Single Leg Triple Hop
Starting at a designated line, the patient will balance on one
leg and hop forward three times consecutively as far as
possible, landing on the same leg. The patient must
maintain their balance on the last hop. To pass, the
involved leg must measure at least 90% of the distance
compared to the uninvolved leg.
3. Single Leg Triple Crossover Hop
Starting at a designated line, the patient will balance on one
leg and hop medially at a 45-degree angle as far as possible,
immediately hop laterally at a 45-degree angle, and then
immediately hop medially again at a 45-degree angle,
landing on the same leg. The patient must maintain their
balance on the last hop. To pass, the involved leg must
measure at least 90% of the distance forward compared to
the uninvolved leg.
4. Timed 6-meter Single Leg Hop
Starting at a designated line, the patient will balance on one
leg and hop as fast as they can consecutively a distance of 6
meters. To pass, the involved leg must hop 6 meters in at
least 90% of the time compared to the uninvolved leg. (6
meters = 19.7 feet)
5. Single Leg Medial Hop
Starting at a designated line, the patient will balance on one
leg and hop medially as far as possible, landing on the same
leg. The patient must maintain their balance. To pass, the
involved leg must measure at least 90% of the distance
compared to the uninvolved leg.
6. Single Leg Lateral Hop
Starting at a designated line, the patient will balance on one
leg and hop laterally as far as possible, landing on the same
leg. The patient must maintain their balance. To pass, the
involved leg must measure at least 90% of the distance
compared to the uninvolved leg.
7. Peak Torque at 60 Degrees
The patient will sit at the end of the plinth or in the leg
extension machine. With a crane scale anchored to the
testing limb at 90 degrees to the tibia, measure the distance
from the inferior pole of the patella to the anchor on the
lower portion of the lower limb. The patient is instructed to
slowly kick out to a max effort. The isometric quadriceps
contraction should be at 60 degrees of knee flexion. The
testing therapist will record the max number recorded on
the crane scale. That number is then converted to newtons.
Then multiply the length of the limb (in meters) by the
force (in newtons) and divide by the patient’s weight (in
kg). This will give you the peak force in N*m/kg. Normative
data should be above 3 N*m/kg and LSI should be >90%.
8. SL Squat Test
Have the patient sit on a chair or plinth with the test leg
bent to 90 degrees, and 10cm from the edge of the chair.
With hands folded across the chest, the patient aims to
stand up from the sitting position, and sit down as many
times as possible. (>22 repetitions per side and >90% LSI
for passing grade)
9. Drop Jump Test
The patient starts on a 12” box, hands placed on the hips.
The patient then drops down off the box to the floor,
bending both knees on landing, then immediately performs
a max vertical jump. The patient should land on both feet in
the same spot they took off from. This can be performed
using a video capture app and timer or with timing mats if
available. We are looking to calculate time in air as well as
overall landing mechanics.
10. Fatigued Drop Jump Test
Prior to performing a second drop jump test as above, the
patient will perform the following: 1 minute of jumping
jacks, 30 bodyweight squats, 1 min plank and 30
alternating lunge jumps. The patient will not be given a rest
break during those four exercises and will immediately
perform another drop jump test. We are comparing time in
air for both trials as well as overall movement quality of the
two trials.
11. 10-Yard Pro-Agility Run
The patient will start straddling line A and will turn and
sprint five yards to line B. Then the patient will sprint ten
yards to line C. Finally, the patient will sprint five yards
through line A. The patient must make sure to touch each
line with his/her hand. The administrator will measure the
time it takes for patient to complete the test. This test will
be completed in reverse order (A to C to B to A) to make
sure the patient is planting with both the involved and
uninvolved foot. (Males ≤4.5-5.5 seconds; Females ≤5.5-6.5
seconds) See diagram.
CRITERIA TO PASS RETURN TO
SPORT TESTING: ALL TESTING ITEMS
ON THE INVOLVED SIDE MUST BE
WITHIN 90% OF THE UNINVOLVED TO
PASS THE TEST. BALANCE MUST BE
HELD FOR AT LEAST 2 SECONDS
WITHOUT ANY EXTRA HOPS.

ORTHOVIRGINIA.COM
ACL Scorecard
PATIENT REPORTED OUTCOMES
PASSING SCORE
PATIENT SCORE
KOOS
>90%
11-18
>90%
1RM STRENGTH TESTING
LEFT (LBS.)
RIGHT (LBS.)
LSI (%)
Leg Press
SL HOP TESTING
LEFT (CM)
RIGHT (CM)
LSI (%)
Single
SINGLE LEG TESTS
LEFT
RIGHT
LSI (%)
Peak Torque at 60
degrees
OTHER TEST
SCORE
Drop Jump Test
