
Child Maltreatment
2022
h
U.S. Department of Health & Human Services
Administration for Children and Families
Administration on Children, Youth and Families
Children’s Bureau
Y
E
A
R
O
F
R
E
P
O
R
T
I
N
G
25
t
Y
E
A
R
O
F
R
E
P
O
R
T
I
N
G
33
rd

This report was prepared by the Children’s Bureau (Administration on Children, Youth and
Families, Administration for Children and Families) of the U.S. Department of Health and
Human Services.
Public Domain Notice
Material contained in this publication is in the public domain and may be reproduced, fully or
partially, without permission of the federal government.
Electronic Access
This report is available on the Children’s Bureau website at
https://www.acf.hhs.gov/cb/data-research/child-maltreatment.
Questions and More Information
If you have questions or require additional information about this report, please contact the
Child Welfare Information Gateway at info@childwelfare.gov or 1–800–394–3366. If you have
questions about a specic state’s data or policies, contact information is provided for each state
in Appendix D, State Commentary.
Data Sets
Restricted use les of the NCANDS submissions are archived at the National Data Archive on
Child Abuse and Neglect (NDACAN) at Cornell University. Researchers who are interested in
these les for statistical analyses may contact NDACAN by phone at 607–255–7799, by email at
ndacan@cornell.edu or on the Internet at https://www.ndacan.acf.hhs.gov/. NDACAN serves as
the repository for the NCANDS data sets, but is not the author of the
Child Maltreatment report.
Recommended Citation
U.S. Department of Health & Human Services, Administration for Children and Families,
Administration on Children, Youth and Families, Children’s Bureau. (2024). Child Maltreatment
2022. Available from https://www.acf.hhs.gov/cb/data-research/child-maltreatment.
Federal Contact
Cara Kelly, Ph.D.
Child Welfare Program Specialist
330 C Street, S.W.
Mary E. Switzer Building, Room 3419B
Washington, DC
cara.kelly@acf.hhs.gov

Child Maltreatment
2022
Child Maltreatment 2022
DEPARTMENT OF HEALTH & HUMAN SERVICES
Letter from the Associate Commissioner:
Child Maltreatment 2022 (the report) is the latest edition of the annual Child Maltreatment
report series. The report is used by researchers, practitioners, and advocates throughout the
world as a source for national child welfare data. The report is available from our website
at https://www.acf.hhs.gov/cb/data-research/child-maltreatment.
Jurisdictions provide the data for this report via the National Child Abuse and Neglect Data
System (NCANDS). NCANDS was established as a voluntary, national data collection and
analysis program to make available state child abuse and neglect information. Since 1991,
child welfare agencies in the 50 states, the Commonwealth of Puerto Rico, and the District
of Columbia have collected and submitted data for NCANDS. For federal scal year (FFY)
2022, 52 states submitted both a Child File and an Agency File. Key ndings in this report
include:
■ Nationally during FFY 2022, 3,096,101 children received either an investigation response or
alternative response at a rate of 42.4 children per 1,000 in the population.
■ For FFY 2022, 52 states reported 558,899 victims of child abuse and neglect. This is a national
rate of 7.7 victims per 1,000 children in the population.
■ FFY 2022 data show 74.3 percent of victims experience neglect, 17.0 percent are physically
abused, 10.6 percent are sexually abused, and 6.8 percent are psychologically maltreated.
■ A nationally estimated 1,990 children died from abuse and neglect at a rate of 2.73 per 100,000
children in the population.
1
NCANDS would not be possible without the time, effort, and dedication of state and local
child welfare, information technology, and related agency personnel working together on
behalf of children and families. We gratefully acknowledge the efforts of all involved to
make resources like this report possible as we continue to do everything we can to promote
the safety and well-being of our nation’s children.
Data is critically important to improving child welfare outcomes. But data can only take us
so far. Good data does more than just provide us with information. These key ndings should
lead to further exploration and questions. For example, what story is the data starting to
tell? What information is missing? How is the data collected, and who made decisions about
which data is important to collect? Is there a diverse group of people determining which data
is important to collect? Is any group that is not represented in the data collection? How can
we drive innovation and better outcomes for children and families using these data?
Throughout all of our work, the Children’s Bureau continues to focus on promoting equity
and reducing disproportionality in child welfare systems. Chapter seven of the Child
Maltreatment 2022 report is entitled “Special Focus.” The analyses in this chapter review the
different dimensions of maltreatment data so that jurisdictions can have more information to
examine and prevent disproportionate outcomes, particularly for Black, Brown, and Native
American children. This data also can be used to inform specic programs or policies to
1
The national estimate of child fatalities is calculated by multiplying the national fatality rate by the child population of all
52 states and dividing by 100,000. The estimate is rounded to the nearest 10. For 2022, 51 states reported fatality data.
Letter iiii

iii
Child Maltreatment 2022
support victims of child maltreatment and to work with families to prevent maltreatment. We
hope jurisdictions will use the data and analyses in the Child Maltreatment 2022 report and
other sources of information to work to reduce disproportionate outcomes for populations of
children and their families.
Preventing maltreatment should always be the top priority. Children’s Bureau has worked
arduously to support jurisdictions to submit title IV-E prevention plans that include excit
ing evidence-based programs. Additionally, we have promulgated a regulation that will
allow
-
separate licensing standards for relative caregivers in support of caregivers who
care for children who cannot live with their parents safely. Similarly, we have published a
Notice of Proposed Rulemaking that will allow agencies to claim federal nancial participa
tion for the cost of providing an attorney to categories of individuals who are involved with
child welfare cases.
-
The Child Maltreatment 2022 report provides important, detailed insight into what is hap
pening for children who are the subject of a CPS investigation or CPS alternative response.
However, the report is only the beginning of the inquiry: use it to ask yourself and your
colleagues more questions and to challenge existing assumptions. For example, think about
ways to support families who have economic needs in order to prevent child maltreatment or
child welfare involvement. What additional questions does the disproportionality data raise
for you? My hope and expectation is that this report will encourage jurisdictions to ask as
many questions as it answers so that we can continue to work together to improve the lives
and outcomes for children, young people, and families. Thank you, as always, for using your
time, talent, and creativity in support of the families that we serve.
-
In Unity,
/s/
Aysha E. Schomburg, Associate Commissioner, Children’s Bureau
Letter

Child Maltreatment 2022
Acknowledgements iv
Acknowledgements
The Children’s Bureau in the Administration on Children, Youth and Families (ACYF), the
Administration for Children and Familes (ACF), within the U.S. Department of Health and
Human Services (HHS), strives to ensure the wellbeing of our Nation’s children through
many programs and activities. One such activity is the National Child Abuse and Neglect
Data System (NCANDS) of the Children’s Bureau. National and state statistics about child
maltreatment are derived from the data collected by child protective services agencies and
reported to NCANDS. The data is analyzed, disseminated, and released in an annual report.
Child Maltreatment 2022 marks the 33rd edition of this report. The administration hopes that
the report continues to serve as a valuable resource for policymakers, child welfare practitio
ners, researchers, and other concerned citizens.
-
The 2022 national statistics are based upon receiving case-level and aggregate data from 50
states, the Commonwealth of Puerto Rico, and the District of Columbia.
CB/ACYF/ACF/HHS wishes to thank the many people who made this publication possible.
The Children’s Bureau has been fortunate to collaborate with informed and committed state
personnel who work hard to provide comprehensive data, which reects the work of their
agencies.
CB/ACYF/ACF/HHS gratefully acknowledges the priorities that were set by state and local
agencies to submit data to the Children’s Bureau, and thanks the caseworkers and supervisors
who contribute to and use their state’s information system. The time and effort dedicated by
these and other individuals are the foundation of this successful federal-state partnership.

Contents
Letter from the AssociAte commissioner ii
A
cknowLedgements iv
s
ummAry ix
c
hApter 1: Introduction 1
Background of NCANDS 1
Annual Data Collection Process 2
2020 Census 3
NCANDS as a Resource 3
Structure of the Report 4
c
hApter 2: Reports 6
Screening 6
Report Sources 9
CPS Response Time 10
CPS Workforce and Caseload 10
Exhibit and Table Notes 11
c
hApter 3: Children 17
Alternative Response 18
Unique and Duplicate Counts 19
Children Who Received an Investigation or Alternative Response 19
Children Who Received an Investigation or Alternative Response by Disposition 19
Number of Child Victims 20
Child Victim Demographics 21
Maltreatment Types 22
Focus on Maltreatment Categories 22
Perpetrator Relationship 23
Risk Factors 24
Reporting Infants with Prenatal Substance Exposure to NCANDS 24
Number of Infants with Prenatal Substance Exposure 25
Screened-in Infants with Prenatal Substance Exposure Who Have a Plan of Safe Care 26
Screened-in Infants with Prenatal Substance Exposure Who Have a Referral to
Appropriate Services 26
Exhibit and Table Notes 26
Child Maltreatment 2022
Contents v

chApter 4: Fatalities 52
Number of Child Fatalities 52
Child Fatality Demographics 53
Maltreatment Types 55
Risk Factors 55
Perpetrator Relationship 56
Prior CPS Contact 56
Exhibit and Table Notes 56
c
hApter 5: Perpetrators 64
Number of Perpetrators 64
Perpetrator Demographics 64
Perpetrator Relationship 65
Exhibit and Table Notes 66
c
hApter 6: Services 76
Prevention Services 76
Postresponse Services 78
History of Receiving Services 80
Part C of the Individuals with Disabilities Education Act (IDEA) 80
Exhibit and Table Notes 80
chApter 7: Special Focus 93
Introduction 93
Maltreatment Type Substantiations 94
Maltreatment Type Combinations of Victims 94
Maltreatment Types and Report Sources of Victims 95
Maltreatment Types by Race and Ethnicity 96
Victims of Selected Maltreatment Types by Sex and Age 96
Maltreatment Types of Victims by Perpetrator Sex 99
Conclusion 100
Exhibit and Table Notes 100
Appendix A: CAPTA Data Items 108
A
ppendix B: Glossary 110
A
ppendix c: State Characteristics 128
A
ppendix d: State Commentary 136
Child Maltreatment 2022
Contents vi

Exhibits
Exhibit S–1 Summary of Child Maltreatment Rates per 1,000 Children, 2018–2022 xiv
Exhibit S–2 Statistics at a Glance, 2022 xv
Exhibit 2–A Screened-in Referral Rates, 2018–2022 6
Exhibit 2–B Screened-out Referral Rates, 2018–2022 7
Exhibit 2–C Total Referral Rates, 2018–2022 8
Exhibit 2–D Number of Referrals, 2018–2022 8
Exhibit 2–E Report Sources, 2022 9
Exhibit 3–A Child Disposition Rates, 2018–2022 19
Exhibit 3–B Children Who Received an Investigation or Alternative Response by
Disposition, 2022 20
Exhibit 3–C Child Victimization Rates, 2018–2022 21
Exhibit 3–D Victims by Age, 2022 22
Exhibit 4–A Child Fatality Rates per 100,000 Children, 2018–2022 53
Exhibit 4–B Child Fatalities by Age, 2022 54
Exhibit 4–C Child Fatalities by Sex, 2022 54
Exhibit 4–D Child Fatalities by Race or Ethnicity, 2022 55
Exhibit 4–E Maltreatment Types of Child Fatalities, 2022 55
Exhibit 4–F Child Fatalities with Selected Caregiver Risk Factors, 2022 56
Exhibit 5–A Perpetrators by Age, 2022 65
Exhibit 5–B Perpetrators by Race or Ethnicity, 2022 65
Exhibit 7–A Children by Number of Maltreatment Type Combinations, 2022 95
Exhibit 7–B Selected Maltreatment Types of Victims by Known Race or
Ethnicity, 2022 96
Exhibit 7–C Victims of Neglect by Sex and Age, 2022 97
Exhibit 7–D Victims of Physical Abuse and Age, 2022
98
Exhibit 7–E Victims of Psychological Maltreatment by Sex and Age, 2022 98
Exhibit 7–F Victims of Sex Abuse by Sex and Age, 2022 99
Tables
Table 2–1 Screened-in and Screened-out Referrals, 2022 13
Table 2–2 Average Response Time in Hours, 2018–2022 14
Table 2–3 Child Protective Services Workforce, 2022 15
Table 2–4 Child Protective Services Caseload, 2022 16
Table 3–1 Children Who Received an Investigation or Alternative Response, 2018–2022 30
Table 3–2 Children Who Received an Investigation or Alternative Response
by Disposition, 2022 32
Table 3–3 Child Victims, 2018–2022 34
Table 3–4 First-time Victims, 2022 36
Table 3–5 Victims by Age, 2022 37
Table 3–6 Victims by Sex, 2022 41
Table 3–7 Victims by Race or Ethnicity, 2022 42
Table 3–8 Maltreatment Types of Victims (Categories), 2022 44
Table 3–9 Victims by Relationship to Their Perpetrators, 2022 46
Table 3–10 Victims with Caregiver Risk Factors, 2022 47
Table 3–11 Infants with Prenatal Substance Exposure by Submission Type, 2022 49
Table 3–12 Screened-in Infants with Prenatal Substance Exposure Who Have
a Plan of Safe Care, 2022 50
Child Maltreatment 2022
Contents vii

Table 3–13 Screened-in Infants with Prenatal Substance Exposure Who
Have a Referral to Appropriate Services, 2022 51
Table 4–1 Child Fatalities by Submission Type, 2022 59
Table 4–2 Child Fatalities, 2018–2022 60
Table 4–3 Child Fatalities by Age, 2022 61
Table 4–4 Child Fatalities by Relationship to Their Perpetrators, 2022 61
the Previous 5 Years, 2022
Table 4–5 Child Fatalities Who Received Family Preservation Services within
62
Previous 5 Years, 2022
Table 4–6 Child Fatalities Who Were Reunited with Their Families within the
63
Table 5–1 Perpetrators, 2018–2022 68
Table 5–2 Perpetrators by Age, 2022 69
Table 5–3 Perpetrators by Sex, 2022 71
Table 5–4 Perpetrators by Race or Ethnicity, 2022 72
Table 5–5 Perpetrators by Relationship to Their Victims, 2022 74
Table 6–1 Children Who Received Prevention Services by Funding Source, 2022 83
Table 6–2 Children Who Received Postresponse Services, 2022 86
Table 6–3 Average and Median Number of Days to Initiation of Services, 2022 87
Removal Date on or After the Report Date, 2022
Table 6–4 Children Who Received Foster Care Postresponse Services and Who Had a
88
Table 6–5 Victims with Court-Appointed Representatives, 2022 89
Previous 5 Years, 2022
Table 6–6 Victims Who Received Family Preservation Services within the
90
Previous 5 Years, 2022
Table 6–7 Victims Who Were Reunited with Their Families within the
91
to Part C Agencies, 2022
Table 6–8 IDEA: Victims Who Were Eligible and Victims Who Were Referred
92
Table 7–1 Maltreatment Type Substantiations, 2022 102
Table 7–2 Maltreatment Type Combinations, 2022 102
Table 7–3 Maltreatment Types of Victims by Report Source, 2022 103
Table 7–4 Maltreatment Types of Victims by Known Race or Ethnicity, 2022 104
Table 7–5 Victims of Neglect by Sex and Age, 2022 104
Table 7–6 Victims of Physical Abuse by Sex and Age, 2022 105
Table 7–7 Victims of Psychological Maltreatment by Sex and Age, 2022 105
Table 7–8 Victims of Sexual Abuse by Sex and Age, 2022 106
Table 7–9 Maltreatment Types of Victims by Perpetrator Sex, 2022 106
Submitted, 2022
Table C–1 State Administrative Structure, Level of Evidence, and Data Files
130
Table C–2 Child Population, 2018–2022 131
Table C–3 Child Population Demographics, 2022 132
Table C–4 Adult Population by Age Group, 2022 135
Child Maltreatment 2022
Contents viii

Summary ix
Child Maltreatment 2022
Summary
Overview
All 50 states, the District of Columbia, and the U.S. Territories have child abuse and
neglect reporting laws that mandate certain professionals and institutions refer sus
pected maltreatment to a child protective services (CPS) agency. Each state has its
own denitions of child abuse and neglect that are based on standards set by federal
law. Federal legislation provides a foundation for states by identifying a set of acts
or behaviors that dene child abuse and neglect. The Child Abuse Prevention and
Treatment Act (CAPTA), (P.L. 100–294), as amended by the CAPTA Reauthorization
Act of 2010 (P.L. 111–320), retained the existing denition of child abuse and neglect
as, at a minimum:
-
Any recent act or failure to act on the part of a parent or caretaker which results in
death, serious physical or emotional harm, sexual abuse or exploitation [ ]; or an
act or failure to act, which presents an imminent risk of serious harm.
The Justice for Victims of Trafcking Act (P.L. 114–22) added the requirement to
include sex trafcking victims in the denition of child abuse and neglect. The follow
ing pages provide a summary of key information from this report. The information is
provided in a question-and-answer format as the Children’s Bureau is anticipating the
most common questions for each chapter of the report. Please refer to the individual
chapters for detailed information about each topic and the relevant data. Denitions
of terms also are provided in Appendix B, Glossary.
-
What is the National Child Abuse and Neglect Data System (NCANDS)?
NCANDS is a federally sponsored effort that collects and analyzes annual data on
child abuse and neglect. The 1988 CAPTA amendments directed the U.S. Department
of Health and Human Services to establish a national data collection and analy
sis program. The data is collected and analyzed by the Children’s Bureau in the
Administration on Children, Youth and Families (ACYF), the Administration for Children
and Families (ACF) within the U.S. Department of Health and Human Services (HHS).
The data is submitted voluntarily by the 50 states, the District of Columbia, and the
Commonwealth of Puerto Rico. The rst report from NCANDS was based on data for
1990. This report for federal scal year (FFY) 2022 is the 33rd issuance of this annual
publication.
-
How is the data used?
NCANDS data is used for the Child Maltreatment report series. In addition, the data
is a critical source of information for many publications, reports, and activities of the
federal government and other groups. For example, NCANDS data is used in the
annual publication, Child Welfare Outcomes: Report to Congress. More information
about these reports and programs are available on the Children’s Bureau website at
https://www.acf.hhs.gov/cb.
What data is collected?
Once an allegation (called a referral) of abuse or neglect is received by a CPS agency,
it is either screened-in for a response by CPS or it is screened-out. A screened-in
referral is called a report. CPS agencies respond to all reports. In most states, the
majority of reports receive investigations, which determine if a child was maltreated
or is at-risk of maltreatment, and establish whether an intervention is needed. Some
reports receive alternative responses, which focus primarily upon the needs of the
family and do not determine if a child was maltreated or is at-risk of maltreatment.
NCANDS collects case-level data on all children who received a CPS agency response
in the form of an investigation response or an alternative response. Case-level data
(meaning individual child record data) includes information about the characteristics of
screened-in referrals (reports) of abuse and neglect that are made to CPS agencies,
the children involved, the types of maltreatment, the dispositions of the CPS responses,
the risk factors of the child and their caregivers, the services that are provided, and the
perpetrators. NCANDS collects agency-level aggregate statistics in a separate data
submission called the Agency File.
Where is the data available?
The Child Maltreatment reports from this edition back to 1995 are available on the
Children’s Bureau website at https://www.acf.hhs.gov/cb/data-research/child-maltreatment.
If you have questions or require additional information about this report, please
contact the Child Welfare Information Gateway at info@childwelfare.gov or
1–800–394–3366. Restricted use les of NCANDS submissions are archived at the
National Data Archive on Child Abuse and Neglect (NDACAN) at Cornell University
https://www.ndacan.acf.hhs.gov/. Researchers who are interested in using these les
for statistical analyses may contact NDACAN by phone at 607–255–7799 or by email at
ndacan@cornell.edu. See chapter 1 for more information about NCANDS and the data
collection.
How many allegations of maltreatment are reported and screened-in
for an investigation response or alternative response?
For 2022, CPS agencies received a national estimate of 4,276,000 total referrals. The
total referrals alleging maltreatment includes approximately 7,530,000 children. The
national rate of screened-in referrals (reports) is 29.0 per 1,000 children in the national
population. Among the 47 states that report both screened-in and screened-out refer
rals, 49.5 percent of referrals are screened-in and 50.5 percent are screened-out.
-
Child Maltreatment 2022
Summary x

Summary xi
Child Maltreatment 2022
Who reports child maltreatment?
For 2022, professionals submitted 70.0 percent of reports alleging child abuse and
neglect. The term professional means that the person has contact with the alleged
child maltreatment victim as part of his or her job. This term includes teachers, police
ofcers, lawyers, and social services staff. The highest percentages of reports are
from legal and law enforcement personnel (21.2%), education personnel (20.7%), and
medical personnel (11.2%).
Nonprofessionals, including friends, neighbors, and relatives, submitted fewer than
one-fth of reports (15.2%). Unclassied sources submitted the remaining reports
(14.8%). Unclassied includes anonymous, “other,” and unknown report sources.
States use the code “other” for any report source that does not have an NCANDS
designated code. See Appendix D, State Commentary, for additional information
provided by the states as to what is included in “other.” See chapter 2 for more
information about referrals and reports.
Who are the child victims?
For FFY 2022, there are 558,899 victims of child abuse and neglect nationally. The
victim rate is 7.7 victims per 1,000 children in the population. (See chapter 3.) Victim
demographics include:
■ Children younger than 1 year old have the highest rate of victimization at 22.2 per
1,000 children of the same age in the national population.
■ The victimization rate for girls is 8.2 per 1,000 girls in the population, which is
higher than boys at 7.1 per 1,000 boys in the population.
■ American-Indian or Alaska Native children have the highest rate of victimization
at 14.3 per 1,000 children in the population of the same race or ethnicity; and
Black or African-American children have the second highest rate at 12.1 per
1,000 children of the same race or ethnicity.
What are the most common types of maltreatment?
NCANDS collects all maltreatment type allegations, however only those maltreat
ments with a disposition of substantiated or indicated are included in the Child
Maltreatment report. A child may be determined to be a victim multiple times within
the same FFY and up to four different maltreatment types in each victim report.
-
In the analysis included in chapter 3, a victim who has more than one type of
maltreatment is counted once per type. This answers the question of how many
different types of maltreatment do victims have, rather than how many occurrences
of each type. For FFY 2022, 74.3 percent of victims are neglected, 17.0 percent are
physically abused, 10.6 percent are sexually abused, and 6.8 are psychologically
maltreated.
How many infants with prenatal substance exposure are there?
The Comprehensive Addiction and Recovery Act (CARA) of 2016 includes an
amendment to CAPTA to collect and report the number of infants with prenatal
substance exposure (IPSE), IPSE with a plan of safe care, and IPSE with a referral to
appropriate services.
FFY 2022 data shows 45,756 infants in 50 states being referred to CPS agencies
as infants with prenatal substance exposure. The majority (79.2%) of IPSE were
screened-in to CPS to receive either an investigation or alternative response. For
FFY 2022, 33 states reported 23,781 screened-in IPSE (69.5%) have a plan of safe
care and 32 states reported 22,883 screened-in IPSE (68.4%) have a referral to
appropriate services.
What risk factors do caregivers have?
Risk factors are characteristics of a child or caregiver that may increase the likeli
hood of child maltreatment. Caregivers with these risk factors who are included in
each analysis may or may not be the perpetrators responsible for the maltreatment.
Refer to chapter 3 or Appendix B, Glossary for denitions of caregiver risk factors
included in this report.
-
In 39 reporting states, 95,794 victims (23.8%) have the drug abuse caregiver risk
factor and in 35 reporting states, 99,255 victims (26.5%) have the domestic violence
caregiver risk factor. See chapter 3 for more information about maltreatment victims.
How many children died from abuse or neglect?
Child fatalities are the most tragic consequence of maltreatment. For FFY 2022, a
national estimate of 1,990 children died from abuse and neglect at a rate of 2.73 per
100,000 children in the population. See chapter 4 for more information about child
fatalities. The child fatality demographics show:
■ The youngest children are the most vulnerable to maltreatment, with children
younger than 1 representing 44.7 percent of child fatalities; a fatality rate of 24.37
per 100,000 children in that age range.
■ Boys have a higher child fatality rate at 3.26 per 100,000 boys in the population
when compared with girls at 2.25 per 100,000 girls in the population.
■ The rate of Black or African-American child fatalities (6.37 per 100,000 African-
American children) is 3.3 times greater than the rate of White children (1.99 per
100,000 White children) and 3.8 times greater than the rate of Hispanic children
(1.68 per 100,000 Hispanic children).
Who abuses and neglects children?
A perpetrator is the person who is responsible for the abuse or neglect of a child.
Fifty-two states reported 434,090 perpetrators. See chapter 5 for more information
about perpetrators of maltreatment. The analyses of case-level data show:
■ The majority (68.8%) of perpetrators are between the ages of 25 and 44 years old.
■ More than one-half of perpetrators are female, 47.7 percent of perpetrators are
male, and 1.1 percent have an unknown sex.
■ The three largest percentages of perpetrators are White (47.4%), Black or African-
American (21.0%), and Hispanic (20.3%).
■ The majority (76.0%) of perpetrators are a parent to their victim.
Child Maltreatment 2022
Summary xii

Who received services?
CPS agencies provide services to children and their families, both in their homes
and in foster care. Reasons for providing services may include (1) preventing future
instances of child maltreatment and (2) remedying conditions that brought the chil
dren and their family to the attention of the agency. See chapter 6 for more informa
tion about children and their families who received services. During 2022:
-
-
■ Forty-ve states reported approximately 1.9 million (1,922,792) children received
prevention services.
■ Fifty-one states reported 897,486 children (both victims and nonvictims) received
postresponse services from a CPS agency.
■ More than one-half (55.0%) of victims and one-fth (20.3%) of nonvictims received
postresponse services.
What is the Special Focus chapter?
The purpose of chapter 7 is to highlight analyses of specic subsets of children or
data analyses focusing on a specic topic. The analyses in this chapter review the
different dimensions of maltreatment type data to determine if there are any patterns
or disproportionality within the data that will assist with targeting specic programs or
policies to aid the victims and their families. Key highlights include:
■ The FFY 2022 data shows 88.6 percent of victims have one type of substantiated
maltreatment, although, they could be reported and determined to be a victim of
one type of maltreatment multiple times.
■ For all report sources, neglect is the most common maltreatment type.
Percentages range from 51.0 percent from mental health personnel to 71.7 from
unclassied.
■ Within each race or ethnicity, most victims have the neglect maltreatment type.
Also, most races or ethnicities have physical abuse as the second highest per-
centage of maltreatment.
■ Analyzing the most common maltreatment type by age and sex shows that while
nationally the victims of neglect are split relatively evenly between the sexes,
analyzing by single year age shows some differences. From birth until age 10,
boys are more represented among neglect victim; beginning at age 11, girls are
more often determined to be neglect victims.
■ Slightly more victims are maltreated by female perpetrators, at 51.9 percent, than
male perpetrators, at 47.3 percent.
Child Maltreatment 2022
Summary xiii
Child Maltreatment 2022
National Summary
A summary of national rates per 1,000 children is provided below (S–1) and a one–
page chart of key statistics from the annual report is on the following page (S–2).
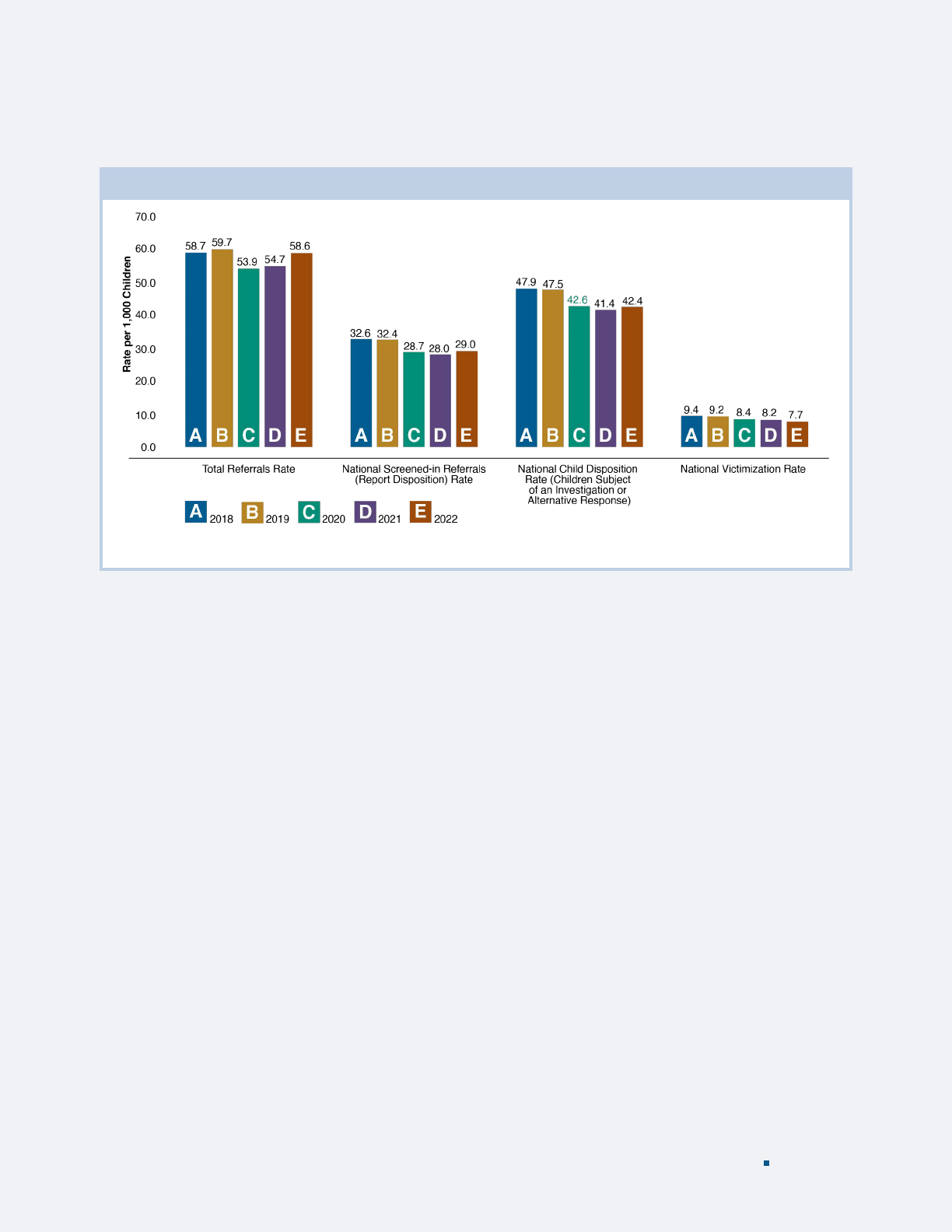
Exhibit S–1 Summary Child Maltreatment Rates per 1,000 Children, 2018–2022
Based on data from 52 states for FFY 2018-2020 and 2022, and 51 states for FFY 2021.
Summary xiv

Exhibit S–2 Statistics at a Glance, 2022
ReferralsReportsChildrenServices
2
,119,706 REPORTS received
a disposition (finding)
Submitted by
70.0% professionals
15.2% nonprofessionals
14.8% unclassied
558,899 VICTIMS
Includes 1,990* Fatalities
2,537,202* NONVICTIMS
3,4
49.5% REFERRALS SCREENED-IN
2
(become reports)
50.5% REFERRALS SCREENED-OUT
2
299,876 VICTIMS
5
received postresponse services
104,747 VICTIMS
6
received foster care services
597,610 NONVICTIMS
4,5
received postresponse services
40,702 NONVICTIMS
4,6
received foster care services
4,276,000* REFERRALS alleging maltreatment to CPS
involving 7,530,000* children
1
3
,096,101 CHILDREN received
Either an investigation or alternative response
*
Indicates a nationally estimated number. Please refer to the relevant chapter notes for information about thresholds, exclusions,
and how the estimates are calculated.
1
The average number of children included in a referral was (1.8 rounded).
2
Among the states that reported both screened-in and screened-out referrals.
3
The number of unique nonvictims is calculated by subtracting the unique count of victims from the unique count of children.
4
Includes children who received an alternative response.
5
Based on data from 51 states. These are duplicate counts.
6
Based on data from 49 states. These are duplicate counts. Only the children who are removed from their home on or after the
report date and up to 90 days after the disposition date are counted.
Child Maltreatment 2022
Summary xv

chApter 1: Introduction 1
Child Maltreatment 2022
Introduction
CHAPTER 1
Child abuse and neglect is one of the nation’s most serious concerns. This important issue is
addressed in many ways by the Children’s Bureau in the Administration on Children, Youth
and Families (ACYF), the Administration for Children and Families (ACF) within the U.S.
Department of Health and Human Services (HHS). The Children’s Bureau strives to ensure
the safety, permanency, and well-being of all children by working with state, tribal, and local
agencies to develop programs to prevent child abuse and neglect in a variety of projects,
including:
■ Providing guidance on federal law, policy, and program regulations.
■ Funding essential services, helping states and tribes operate every aspect of their child
welfare systems.
■ Supporting innovation through competitive, peer-reviewed grants for research and pro-
gram development.
■ Offering training and technical assistance to improve child welfare service delivery.
■ Monitoring child welfare services to help states and tribes achieve positive outcomes for
children and families.
■ Sharing research to help child welfare professionals improve their services.
Child Maltreatment 2022 presents national data about child abuse and neglect known to
child protective services (CPS) agencies in the United States during federal scal year (FFY)
2022. The data is collected and analyzed through the National Child Abuse and Neglect Data
System (NCANDS), which is an initiative of the Children’s Bureau.
Approximately 60 data tables and exhibits are included in the Child Maltreatment report
each year. Certain analyses are determined by federal legislation, while others are in
response to the needs of federal agencies, policy decision makers, child welfare agency staff,
and researchers.
Background of NCANDS
The Child Abuse Prevention and Treatment Act (CAPTA) was amended in 1988 (P.L. 100–
294) to direct the Secretary of HHS to establish a national data collection and analysis pro
gram, which would make available state child abuse and neglect reporting information. HHS
responded by establishing NCANDS as a voluntary national reporting system. During 1992,
HHS produced its rst NCANDS report based on data from 1990. The Child Maltreatment
report series evolved from that initial report and is now in its 33rd edition. During 1996,
CAPTA was amended to require all states that receive funds from the Basic State Grant
program to work with the Secretary of HHS to provide specic data, to the maximum extent
practicable, about children who had been maltreated. Subsequent CAPTA amendments added
-

Child Maltreatment 2022
chApter 1: Introduction 2
data elements and readers are encouraged to review Appendix A, CAPTA Data Items, most of
which are reported by states to NCANDS.
A successful federal-state partnership is the core component of NCANDS. Each state desig
nates one person to be the NCANDS state contact. The state contacts from all 52 states (unless
otherwise noted, the term “states” includes the District of Columbia and the Commonwealth
of Puerto Rico) work with the Children’s Bureau and the NCANDS Technical Team to uphold
the high-quality standards associated with NCANDS data. Webinars, technical bulletins,
virtual meetings, email, and phone conferences are used regularly to facilitate information
sharing and provision of technical assistance.
-
NCANDS has the objective to collect nationally standardized case-level and aggregate
data and to make the data useful for policy decision makers, child welfare researchers, and
practitioners. The NCANDS Technical Team developed a general data standardization (map
ping) procedure whereby all states systematically dene the rules for extracting the data
from the states’ child welfare information system into the standard NCANDS data format.
Team members provide one-on-one technical assistance to states to assist with data mapping,
construction, extraction, and data submission and validation.
-
Annual Data Collection Process
The NCANDS reporting year is based on the FFY calendar, which for Child Maltreatment
2022 is October 1, 2021, through September 30, 2022. States submit case-level data by con
structing an electronic le of child-specic records for each report of alleged child abuse and
neglect that received a CPS response. Each state’s le only includes completed reports with a
disposition (or nding) as an outcome of the CPS response during the reporting year. The data
submission containing the case-level data is called the Child File.
-
The Child File is supplemented by agency-level aggregate statistics in a separate data
submission called the Agency File. The Agency File contains data that are not reportable
at the child-specic level and are often gathered from agencies external to CPS (e.g., vital
statistics departments, child death review teams, law enforcement agencies, etc.). States
are asked to submit both the Child File and the Agency File each year. For more informa
tion about the Child File and Agency File please go to the Children’s Bureau website at
-
https://www.acf.hhs.gov/cb/data-research/ncands.
Upon receipt of data from each state, a technical validation review assesses the internal consis
tency and identies probable causes for any missing data. If the reviews conclude that correc
tions are necessary, the state may be asked to resubmit its data. States also have the opportunity
to give context to their data by providing information about policies, procedures, and legislation
in their State Commentary. (See Appendix C, State Characteristics for additional information
about submissions and Appendix D, State Commentary for information from states about their
data.)
-
-
For FFY 2022, 52 states submitted both a Child File and an Agency File. The most recent data
submissions or resubmissions from states are included in trend tables and this may account for
some differences in the counts from previous reports.

Child Maltreatment 2022
chApter 1: Introduction 3
2020 Census
With each Child Maltreatment report, the most recent population data from the U.S. Census
Bureau are used. Child Maltreatment 2022 is the second edition to use population estimates
from the 2020 Census. The population estimates for 2020–2022 are the most recently
updated estimates based on the 2020 census.
2
Information about the population estimates
may be found at https://www.census.gov/. According to the U.S. Census Bureau, the 2022
child population is for more than 72 million children. See table C–2.
NCANDS as a Resource
The NCANDS data is a critical source of information for many publications, reports, and
activities of the federal government, child welfare personnel, researchers, and others. Some
examples of programs and reports that use NCANDS data are discussed below. More infor
mation about these reports and programs are available on the Children’s Bureau website at
-
https://www.acf.hhs.gov/cb.
■ Child Welfare Outcomes: Report to Congress: This annual report presents informa
tion on state and national performance in seven outcome categories. Data for the
Child Welfare Outcomes measures and the majority of the context data in this report
come from NCANDS and the Adoption and Foster Care Analysis and Reporting
System (AFCARS). The reports are available on the Children’s Bureau’s website at
-
https://www.acf.hhs.gov/cb/data-research/child-welfare-outcomes.
■ Child and Family Services Reviews (CFSRs): The Children’s Bureau conducts periodic
reviews of state child welfare systems to ensure conformity with federal requirements,
determine what is happening with children and families who are engaged in child welfare
services, and assist states with helping children and families achieve positive outcomes.
States develop Program Improvement Plans to address areas revealed by the CFSR as in need
of improvement. For CFSR Round 4, NCANDS data is the basis for two of the CFSR national
data indicators, Recurrence of Maltreatment and Maltreatment in Foster Care. NCANDS
data is also used for data quality checks and context data.
The NCANDS data is also used for several performance measures published annually as part
of the ACF Annual Budget Request to Congress, which highlights certain key performance
measures. Specic measures on which ACF reports using NCANDS data include:
■ Decrease the rate of rst-time victims per 1,000 children in the population.
■ Decrease the percentage of children with substantiated or indicated reports of maltreat
ment who have a repeated substantiated or indicated report of maltreatment within six
months.
-
■ Improve states’ average response time between maltreatment report and investigation,
based on the median of states’ reported average response time in hours from screened-in
reports to the initiation of the investigation.
2
U.S. Census Bureau, Population division. (2023). Annual State Resident Population Estimates for 6 Race Groups (5 Race
Alone Groups and Two or More Races) by Age, Sex, and Hispanic Origin: April 1, 2020 to July 1, 2022; (SC-EST2022-
ALLDATA6) [data le]. Retrieved June 2023 from https://www.census.gov/newsroom/press-kits/2023/population-
estimates-characteristics.html and Annual Estimates of the Resident Population by Single Year of Age and Sex for the
Puerto Rico Commonwealth: April 1, 2020 to July 1, 2022 (PRC-EST2022-SYASEX) [data le]. Retrieved June 2023 from
https://www.census.gov/data/tables/time-series/demo/popest/2020s-detail-puerto-rico.html

Child Maltreatment 2022
chApter 1: Introduction 4
The National Data Archive on Child Abuse and Neglect (NDACAN) was established by
the Children’s Bureau to encourage scholars to use existing child maltreatment data in
their research. NDACAN acquires data sets from national data collection efforts and from
individual researchers, prepares the data and documentation for secondary analysis, and dis
seminates the data sets to qualied researchers who apply to use the data. NDACAN houses
the NCANDS’s Child Files and Agency Files and licenses researchers to use the data sets.
NDACAN has its own strict condentiality protection procedures. Please note that NDACAN
is not the author of the Child Maltreatment report series. More information is available at
-
https://www.ndacan.acf.hhs.gov/index.cfm.
In addition, NCANDS data is provided to other agencies as part of federal initiatives, includ
ing Healthy People
-
https://health.gov/healthypeople and America’s Children: Key National
Indicators of Well-Being https://www.childstats.gov/americaschildren.
Structure of the Report
Many tables include 5 years of data to facilitate trend analyses. To accommodate the space
needed to display the child maltreatment data, population data (when applicable) may not
appear on the table and are available in Appendix C, State Characteristics. Tables with
multiple categories or years of data have numbers presented separately from percentages or
rates to make it easier to compare numbers, percentages, or rates across columns or rows.
By making changes designed to improve the functionality and practicality of the report each
year, the Children’s Bureau endeavors to increase readers’ comprehension and knowledge
about child maltreatment. Feedback regarding changes, suggestions for potential future
changes, or other comments related to the Child Maltreatment report are encouraged.
Please provide feedback to the Children’s Bureau’s Child Welfare Information Gateway at
info@childwelfare.gov. The Child Maltreatment 2022 report contains the additional chapters
listed below. Most data tables and notes discussing methodology are at the end of each
chapter:
■ Chapter 2, Reports—referrals and reports of child maltreatment.
■ Chapter 3, Children—characteristics of victims and nonvictims.
■ Chapter 4, Fatalities—fatalities that occurred as a result of maltreatment.
■ Chapter 5, Perpetrators—characteristics of perpetrators of maltreatment.
■ Chapter 6, Services—services to prevent maltreatment and to assist children and
families.
■ Chapter 7, Special Focus—analyses of specic subsets of children or data analyses
focusing on a specic topic.
The report includes the following resources:
■ Appendix A, CAPTA Data Items—the list of data items from CAPTA, most of which
states submit to NCANDS.
■ Appendix B, Glossary—common terms and acronyms used in NCANDS and their
denitions.
■ Appendix C, State Characteristics—child and adult population data and information
about states administrative structures, levels of evidence, and data les submitted to
NCANDS.
■ Appendix D, State Commentary—information about state policies, procedures, and
legislation that may affect data.

Child Maltreatment 2022
chApter 1: Introduction 5
Readers are urged to use state commentaries as a resource for additional context to the
chapters’ text and data tables. States vary in the policies, legislation, requirements, and
procedures. While the purpose of the NCANDS project is to collect nationally standardized
aggregate and case-level child maltreatment data, readers should exercise caution in making
state-to-state comparisons. Each state denes child abuse and neglect in its own statutes
and policies and the child welfare agencies determine the appropriate response for the
alleged maltreatment based on those statutes and policies. Appendix D, State Commentary
also includes phone numbers and email addresses for each NCANDS state contact person.
Readers who would like additional information about specic policies or practices should
contact the respective states.

6
Child Maltreatment 2022
Reports
CHAPTER 2
This chapter presents statistics about referrals alleging child abuse and neglect and how child
protective services (CPS) agencies respond to those allegations. Most agencies use a two-step
process to respond to allegations of child maltreatment: (1) screening and (2) investigation and
alternative response. A CPS agency receives an initial notication, called a referral, alleging
child maltreatment. A referral may involve more than one child. Agency hotline or intake units
conduct the screening response to determine whether a referral is appropriate for further action.
Screening
A referral may be either screened-in or screened-out. Referrals that meet CPS agency cri
teria are screened-in (and called reports) to receive an investigation response or alternative
response from the agency. Referrals that do not meet agency criteria are screened-out or
diverted from CPS to other community agencies. Reasons for screening-out a referral vary
by state policy, but may include one or more of the following:
-
■ Does not concern child abuse and neglect.
■ Does not contain enough information for a CPS agency response to occur.
■ Response by another agency is deemed more appropriate.
■ Children in the referral are the responsibility of another agency or jurisdiction (e.g.,
military installation or tribe).
■ Children in the referral are older than 18 years.
3
During FFY 2022, CPS agencies in the 52 reporting states screened-in 2,119,706 referrals
which is a 12.0 percent decrease from the 2,409,970 referrals reported by 52 states for FFY
2018. See exhibit 2–A and related notes.
Exhibit 2–A Screened-in Referral Rates, 2018–2022
Year
2018
2019
2020
2021
2022
Reporting States
52
52
52
51
52
Child Population of
Reporting States
73,977,376
73,661,476
73,982,567
71,764,371
72,969,166
Screened-in Referrals
(Reports) from
Reporting States
2,409,970
2,383,411
2,123,934
2,008,904
2,119,706
Rate per
1,000 Children
32.6
32.4
28.7
28.0
29.0
Child Population of
52 States
73,977,376
73,661,476
73,982,567
73,356,806
72,969,166
National Estimate/
Actual Screened-in
Referrals
2,409,970
2,383,411
2,123,934
2,053,000
2,119,706
Screened-in referral data is from the Child File. e screened-in referral rate is calculated for each year by dividing the number of screened-in
referrals from reporting states by the child population in reporting states, multiplying the result by 1,000, and displayed as rounded to the tenth.
If fewer than 52 states report screened-in referrals (2021 only) then the national estimate/rounded number of screened-in referrals is a calculation
from the rate (displayed as rounded) of screened-in referrals multiplied by the national population of all 52 states. e result is divided by 1,000 and
rounded to the nearest 1,000. If 52 states report screened-in referrals, the the actual number of referrals reported by states is displayed.
c
hApter 2: Reports
3
Victims of sex trafcking may be included in an NCANDS submission for any victim who is younger than 24 years. See
chapter 3 for more information about victims of sex trafcking.
Child Maltreatment 2022
Screened-in referrals are called reports and may include more than one child. Every state
completes investigation responses for some reports. An investigation response includes
assessing the maltreatment allegation according to state law and policy. The main purpose of
the investigation is: (1) to determine whether the child was maltreated or is at risk of mal
treatment and (2) to determine if services are needed and which services to provide.
-
In some states, certain reports (screened-in referrals) may receive an alternative response.
This response is usually for instances where the child is at a low or moderate risk of maltreat
ment. While states vary in how they design and apply their alternative response programs,
the point is to focus on the family’s service needs to address issues which may cause future
maltreatment. See chapter 3 for more information about alternative response programs.
-
Twenty-one states report data on children in alternative response programs. See chapter 3 for
more information about alternative response. In the National Child Abuse and Neglect Data
System (NCANDS), both investigations and alternative responses result in a CPS nding
called a disposition.
For 2022, a national estimate of 2,156,000 referrals were screened-out. This is an 11.6 percent
increase from the 1,932,000 estimated screened-out referrals for 2018. See exhibit 2–B and
related notes. For 2022, 47 states reported both screened-in and screened-out referral data
and screened-in 49.5 percent and screened-out 50.5 percent of referrals. For those 47 states,
the percentages of screened-in referrals ranged from 16.9 to 98.7 and the percentages of
screened-out referrals ranged from 1.3 to 83.1. See table 2–1 and related notes.
Exhibit 2–B Screened-out Referral Rates, 2018–2022
Year
2018
2019
2020
2021
2022
Reporting States
46
45
47
46
47
Child Population of
Reporting States
59,955,457
59,518,850
62,099,246
60,080,898
61,458,398
Screened-out Referrals
1,565,553
1,625,691
1,564,101
1,602,496
1,816,161
Rate per 1,000
Children
26.1
27.3
25.2
26.7
29.6
Child Population
of 52 States
73,977,376
73,661,476
73,982,567
73,356,806
72,969,166
National Estimate of
Screened-out Referrals
1,932,000
2,012,000
1,863,000
1,957,000
2,156,000
Screened-out referral data is from the Agency File. e screened-out referral rate is calculated for each year by dividing the number of screened-out
referrals from reporting states by the child population in reporting states, multiplying the result by 1,000, and displayed as rounded to the tenth.
e national estimate of screened-out referrals is based upon the rate (rounded) of referrals multiplied by the national population of all 52 states.
e result is divided by 1,000 and rounded to the nearest 1,000.
For 2022, CPS agencies received a national estimate of 4,276,000 total referrals. This is a
1.5 percent decrease from the 4,342,000 estimated total referrals received for 2018. The 2022
estimated total referrals alleging maltreatment includes approximately 7,530,000 children.
4,5
See exhibit 2–C and related notes.
4
Dividing the number of children with dispositions (3,732,871, from table 3–2) by the number of screened-in referrals
(2,119,706, from table 2–1) results in the average number of children included in a screened-in referral (1.8, displayed as
rounded).
5
The average number of children included in a screened-in referral (1.8) multiplied by the national estimate of total
referrals (4,276,000, from exhibit 2–C) results in an estimated 7,530,000 (rounded) children included in total referrals.
c
hApter 2: Reports 7

Child Maltreatment 2022
Exhibit 2–C Total Referrals Rate, 2018–2022
Year
2018
2019
2020
2021
2022
National Estimate/ Actual
Screened-in Referrals
2,409,970
2,383,411
2,123,934
2,053,000
2,119,706
National Estimate of
Screened-out Referrals
1,932,000
2,012,000
1,863,000
1,957,000
2,156,000
National Estimate of Total
Referrals
4,342,000
4,395,000
3,987,000
4,010,000
4,276,000
Child Population of all 52
States
73,977,376
73,661,476
73,982,567
73,356,806
72,969,166
Total Referrals Rate per
1,000 Children
58.7
59.7
53.9
54.7
58.6
Screened-in referral data is from the Child File and screened-out referral data is from the Agency File.
e national estimate of total referrals is the sum of the actual reported or estimated number of screened-in referrals (from exhibit 2–A) and the
number of estimated screened-out referrals (from exhibit 2–B). e sum is rounded to the nearest 1,000. e national total referral rate is calculated
for each year by dividing the national estimate of total referrals by the child population of 52 states, multiplying the result by 1,000, and displayed as
rounded to the tenth.
As shown in exhibits 2–C and 2–D, the estimated number of total referrals received by CPS
agencies increased from FFY 2018 through 2019, decreased during FFY 2020 and began
increasing for FFYs 2021 and 2022. Also of interest is the narrowing gap between screened-
in and screened-out referrals during the previous few years. One state began reporting
screened-out referrals and according to states’ comments in Appendix D, State Commentary,
several states changed to centralized or implemented structured intakes that led to a decrease
in the percentage of referrals screened-in for a CPS response when compared to FFY 2018.
Exhibit 2–D Number of Referrals 2018–2022
The gap between the number of screened-in and screened-out referrals narrowed during the previous 5 years
Based on screened -in referral data for 52 states for FFYs 2018-2020 and 2022, and 51 states for 2021. Based on screened-out referral data for 46 states for FFYs
2018, 2019, and 2021, and 47 states for 2020 and 2022. See exhibit 2-C.
chApter 2: Reports 8

Report Sources
The report source is the role of the person who notied a CPS agency of the alleged child
abuse or neglect in a referral. Only those sources in reports (screened-in referrals) that
receive an investigation response or alternative response are submitted to NCANDS. To aid
with comparisons, report sources are grouped into three categories:
■ Professional: includes persons who encounter the child as part of their occupation, such
as child daycare providers, educators, legal and law enforcement personnel, and medical
personnel. State laws require most professionals to notify CPS agencies of suspected
maltreatment (these are known as mandated reporters).
■ Nonprofessional: includes persons who do not have a relationship with the child based
on their occupation, such as friends, relatives, and neighbors. State laws vary as to the
requirements of nonprofessionals to report suspected abuse and neglect.
■ Unclassied: includes persons who preferred to be anonymous, “other,” and unknown report
sources. States use the code of “other” for any report source that does not have an NCANDS
designated code. According to comments provided by the states, the “other” report source
category might include such sources as religious leader, Temporary Assistance for Needy
Families staff, landlord, tribal ofcial or member, camp counselor, and private agency staff.
Readers are encouraged to review Appendix D, State Commentary for additional informa
tion as to what states include in the category of “other” report source.
-
FFY 2022 data shows professionals submit 70.0 percent of reports. The highest percentages of
reports are from legal and law enforcement personnel (21.2%), education personnel (20.7%),
and medical personnel (11.2%). Nonprofessionals made 15.2 percent of reports with the largest
category of nonprofessional reporters being parents (5.8%), other relatives (5.5%), and friends and
neighbors (3.5%). Unclassied sources submit the remaining 14.8 percent. See exhibit 2–E and
Exhibit 2–E Report Sources, 2022
Professionals submitted the majority of screened-in referrals (reports) that received an investigation or alternative response
Data is from the Child File. Based on data from 48 states. States are excluded from this analysis if more than 15.0 percent had an unknown report source or if
of the known sources, more than 20.0 percent are reported as Other. Supporting data not shown.
9
Child Maltreatment 2022
chApter 2: Reports

chApter 2: Reports 10
Child Maltreatment 2022
related notes. The country has moved into a post-pandemic period, with most children going back
to in-person learning. As expected with this shift, the number and percentage of reports made by
educational personnel increased in FFY 2022 to approximately pre-pandemic levels. For example,
in FFY 2019, educational personnel made 21.0 percent of all reports for that year. The number and
percentage of reports submitted by education personnel dropped its lowest point, of 15.4 percent,
during FFY 2022.
6
For FFY 2022 education personnel made 20.7 percent of total reports.
CPS Response Time
States’ policies usually establish time guidelines or requirements for initiating a CPS
response. The denition of response time is the time from the CPS agency’s receipt of a
referral to the initial face-to-face contact with the alleged victim wherever this is appropriate,
or with another person who can provide information on the allegation(s). States have either
a single response timeframe for all reports or different timeframes for different types of
reports. High-priority responses are often stipulated to occur within 24 hours; lower priority
responses may occur within several days.
Based on data from 41 states, the FFY 2022 mean response time of state averages is 93 hours
or 3.9 days; the median response time of state averages is 56 hours or 2.3 days. See table 2–2
and related notes. Sixteen states reported a decrease and 25 states reported an increase in
average response times for FFY 2022 when compared with FFY 2021. One state began
reporting during FFY 2022. States that provided comments about the increase in response
times cited staff turnover or increased focus on training. Some states’ explanations for long
response times are related to the geography of the state, meaning the distance from the
agency to the alleged victim, difculties related to the terrain, and weather-related delays
during certain times of the year (for example, winter or hurricane season).
CPS Workforce and Caseload
Given the large number and the complexity of CPS responses that are conducted each year,
there is ongoing interest in the size of the workforce that performs CPS functions. In most
agencies, different groups of workers conduct screening, investigations, and alternative
responses. However, in some agencies, one worker may perform all or any combination of
those functions and may provide additional services. Due to limitations in states’ information
systems and the fact that workers may conduct more than one function in a CPS agency, the
data in the workforce and caseload tables vary among the states. The Children’s Bureau asks
states to submit data for workers as full-time equivalents when possible.
For FFY 2022, 45 states reported a total workforce of 30,750 and 41 states reported 5,036
specialized intake and screening workers. This is an increase from FFY 2021 when 43 states
reported 29,925 total workers and 40 states reported 4,750 intake and screening workers. The
number of investigation and alternative response workers—20,052—is computed by subtract
ing the reported number of intake and screening workers from the total workforce number in
the 41 reporting states.
-
See table 2–3 and related notes.
Using the data from the same 41 states that report on workers with specialized functions,
investigation and alternative response workers completed an average of 69 CPS responses per
worker for FFY 2022. See table 2–4 and related notes. This is an increase from the average
of 64 responses per worker for FFY 2021.
6
Child Maltreatment 2019 and Child Maltreatment 2021.

Child Maltreatment 2022
Exhibit and Table Notes
The following pages contain the data tables referenced in chapter 2. Specic information
about state submissions can be found in Appendix D, State Commentary. Additional informa
tion regarding the exhibits and tables is provided below.
-
General
During data analyses, thresholds are set to ensure data quality is balanced with the need to
report data from as many states as possible. States may be excluded from an analysis for data
quality issues. Exclusion rules are in the table notes below. Not every table has exclusion
rules.
■ Rates are per 1,000 children in the population. Rates are calculated by dividing the relevant
reported count (screened-in referrals, total referrals, etc.) by the relevant child population
count and multiplying by 1,000.
■ NCANDS uses the child population estimates that are released annually by the U.S. Census
Bureau. These population estimates are provided in Appendix C, State Characteristics.
■ National totals and calculations appear in a single row labeled National instead of separate
rows labeled total, rate, or percent.
■ The row labeled Reporting States displays the count of states that provided data for that
analysis.
■ Dashes are inserted into cells without any data.
Table 2–1 Screened-in and Screened-out Referrals, 2022
■ Screened-out referral data is from the Agency File and screened-in referral data is from the
Child File.
■ This table includes screened-in referral data from all states and screened-out referral data
from 47 reporting states.
■ The state total referral rate is based on the number of total referrals divided by the child
population (see table C–2) of states reporting both screened-in and screened-out referrals and
multiplying the result by 1,000.
Table 2–2 Average Response Time in Hours, 2018–2022
■ Data is from the Agency File.
■ The national mean of states’ reported average response time is calculated by summing the
average response times from the states and dividing the total by the number of states report
ing. The result is rounded to the nearest whole number.
-
■ The national median is determined by sorting the states’ averages and nding the midpoint.
Table 2–3 Child Protective Services Workforce, 2022
■ Data is from the Agency File.
■ Some states provide the total number of CPS workers, but not the specics on worker func
tions as classied by NCANDS.
-
■ States are excluded if the worker data is not full-time equivalents.
Table 2–4 Child Protective Services Caseload, 2022
■ Data is from the Child File and the Agency File.
■ The number of completed reports per investigation and alternative response worker for each
state was based on the number of completed reports, divided by the number of investigation
and alternative response workers, and rounded to the nearest whole number.
chApter 2: Reports 11

Child Maltreatment 2022
■ The national number of reports per worker is based on the total of completed reports for
the reporting states, divided by the total number of investigation and alternative response
workers, and rounded to the nearest whole number.
■ States are excluded if the worker data is not full-time equivalents.
■ States are excluded if they do not report intake and screening workers separately from all
workers.
chApter 2: Reports 12

Child Maltreatment 2022
Table 2–1 Screened-in and Screened-out Referrals, 2022
State
Screened-in
Referrals (Reports)
Screened-out
Referrals Total Referrals
Screened-in
Referrals (Reports)
Percent
Screened-out
Referrals Percent
Total Referrals Rate
per 1,000 Children
Alabama 26,837 348 27,185 98.7 1.3 24.5
Alaska 6,627 12,674 19,301 34.3 65.7 109.3
Arizona 44,806 39,924 84,730 52.9 47.1 53.3
Arkansas 31,923 25,416 57,339 55.7 44.3 82.3
California 192,197 189,948 382,145 50.3 49.7 44.9
Colorado 31,792 77,321 109,113 29.1 70.9 89.8
Connecticut 12,709 35,971 48,680 26.1 73.9 66.6
Delaware 5,697 15,617 21,314 26.7 73.3 102.4
District of Columbia 4,039 11,029 15,068 26.8 73.2 121.1
Florida 138,711 103,799 242,510 57.2 42.8 56.4
Georgia 52,994 70,465 123,459 42.9 57.1 49.2
Hawaii 2,897 3,365 6,262 46.3 53.7 21.1
Idaho 7,465 13,741 21,206 35.2 64.8 45.8
Illinois 94,433 - 94,433 100.0 - -
Indiana 102,320 68,765 171,085 59.8 40.2 109.0
Iowa 34,900 18,372 53,272 65.5 34.5 73.5
Kansas 23,095 22,394 45,489 50.8 49.2 65.8
Kentucky 37,894
56,974 94,868 39.9 60.1 94.4
Louisiana 17,742 31,197 48,939 36.3 63.7 46.1
Maine 9,289 17,465 26,754 34.7 65.3 107.9
Maryland 19,629 41,512 61,141 32.1 67.9 45.4
Massachusetts 39,075 42,206 81,281 48.1 51.9 60.8
Michigan 68,359 105,910 174,269 39.2 60.8 82.6
Minnesota 25,662 55,983 81,645 31.4 68.6 63.1
Mississippi 28,282 8,183 36,465 77.6 22.4 53.8
Missouri 54,386 27,791 82,177 66.2 33.8 60.2
Montana 7,301 4,296 11,597 63.0 37.0 49.6
Nebraska 13,845 23,348 37,193 37.2 62.8 78.0
Nevada 16,117 25,804 41,921 38.4 61.6 60.8
New Hampshire 10,183 8,089 18,272 55.7 44.3 72.2
New Jersey 57,068 - 57,068 100.0 - -
New Mexico 20,743 17,992 38,735 53.6 46.4 84.3
New York 148,956 - 148,956 100.0 - -
North Carolina 62,304 45,232 107,536 57.9 42.1 46.9
North Dakota 2,808 - 2,808 100.0 - -
Ohio 79,081 116,517 195,598 40.4 59.6 76.3
Oklahoma 33,529 47,899
81,428 41.2 58.8 85.4
Oregon 36,174
37,104 73,278 49.4 50.6 87.5
Pennsylvania 39,775 - 39,775 100.0 - -
Puerto Rico 7,701 6,272 13,973 55.1 44.9 27.0
Rhode Island 4,597 8,529 13,126 35.0 65.0 64.4
South Carolina 36,620 30,717 67,337 54.4 45.6 60.2
South Dakota 2,496 12,317 14,813 16.9 83.1 67.6
Tennessee 71,046 71,500 142,546 49.8 50.2 92.7
Texas 207,429 38,001 245,430 84.5 15.5 32.9
Utah 21,590 22,689 44,279 48.8 51.2 47.5
Vermont 3,457 14,981 18,438 18.7 81.3 160.7
Virginia 33,801 49,869 83,670 40.4 59.6 44.8
Washington 41,645 67,974 109,619 38.0 62.0 66.6
West Virginia 22,354 13,296 35,650 62.7 37.3 101.3
Wisconsin 23,009 52,396 75,405 30.5 69.5 60.5
Wyoming 2,317 4,969 7,286 31.8 68.2 56.0
National 2,119,70 6 1,816,161 3,935,867 - - -
Reporting States 52 47 52 - - -
National for states reporting
both screened-in and
screened-out referrals 1,776,666 1,816,161 3,592,827 49.5 50.5 N/A
chApter 2: Reports 13

Child Maltreatment 2022
Table 2–2 Average Response Time in Hours, 2018–2022
State 2018 2019 2020 2021 2022
Alabama 53 51 48 51 60
Alaska 423 602 576 219 223
Arizona 31 32 31 - 35
Arkansas 98 104 98 104 114
California 148 148 141 - -
Colorado 114 116 116 114 117
Connecticut 46 42 31 32 30
Delaware 354 409 296 174 380
District of Columbia 29 23 15 15 16
Florida 11 9 9 10 11
Georgia - - - - -
Hawaii 338 315 269 322 304
Idaho 60 64 62 69 107
Illinois - - - - -
Indiana 64 63 63 60 53
Iowa 52 63 55 56 53
Kansas 123 101 125 88 81
Kentucky 96 121 200 172 221
Louisiana - - - 119 208
Maine 87 94 61 58 -
Maryland - - - - -
Massachusetts -
- - - -
Michigan 34 43 42 41 39
Minnesota 79 72 84 89 41
Mississippi 31 34 30 33 37
Missouri 48 61 - 44 49
Montana - - - - -
Nebraska 136 123 121 124 150
Nevada 68 69 64 68 56
New Hampshire 129 113 92 74 64
New Jersey 18 19 18 21 22
New Mexico 63 89 73 55 50
New York 12 12 10 11 14
North Carolina - - - - -
North Dakota - - - - -
Ohio 23 24 24 24 24
Oklahoma 50 47 50 53 55
Oregon 150 165 157 166 168
Pennsylvania - - - - -
Puerto Rico - - 141 152 157
Rhode Island 32 20 19 17 19
South Carolina 38 42 33 37 39
South Dakota 51 34 33 41 42
Tennessee - - -
- 167
Texas 50 50 50 56 64
Utah 81 76 81 93 93
Vermont 94 92 107 129 126
Virginia - - - - -
Washington 38 37 35 34 32
West Virginia 238 339 309 174 147
Wisconsin 119 113 111 109 112
Wyoming 18 23 15 11 13
National Average 93 101 97 83 93
National Median 62 64 62 59 56
Reporting States 40 40 40 40 41
chApter 2: Reports 14

Child Maltreatment 2022
Table 2–3 Child Protective Services Workforce, 2022
State Intake and Screening Workers
Investigation and Alternative
Response Workers
Intake, Screening, Investigation,
and Alternative Response Workers
Alabama
Alaska
Arizona
Arkansas
California
Colorado
Connecticut
Delaware
District of Columbia
Florida
Georgia
Hawaii
Idaho
Illinois
Indiana
Iowa
Kansas
Kentucky
Louisiana
Maine
Maryland
Massachusetts
Michigan
Minnesota
Mississippi
Missouri
Montana
Nebraska
Nevada
New Hampshire
New Jersey
New Mexico
New York
North Carolina
North Dakota
Ohio
Oklahoma
Oregon
Pennsylvania
Puerto Rico
Rhode Island
South Carolina
South Dakota
Tennessee
Texas
Utah
Vermont
Virginia
Washington
West Virginia
Wisconsin
Wyoming
National
Reporting States
87
16
98
45
-
-
50
32
37
-
-
12
16
196
122
39
83
87
45
35
-
138
161
483
22
31
23
48
58
23
113
57
-
172
-
-
80
166
-
34
19
-
16
102
519
29
29
104
110
42
1,457
-
5,036
41
451
238
377
467
-
-
409
130
130
-
-
52
174
995
711
233
251
853
181
157
-
326
1,407
517
442
467
191
179
175
113
1,184
178
-
811
-
-
565
446
-
190
81
-
44
956
4,028
124
53
656
530
323
257
-
20,052
41
538
254
475
512
2,200
-
459
162
167
-
-
64
190
1,191
833
272
334
940
226
192
616
464
1,568
1,000
464
498
214
227
233
136
1,297
235
-
983
-
-
645
612
2,686
224
100
-
60
1,058
4,547
153
82
760
640
365
1,714
160
30,750
45
chApter 2: Reports 15

Child Maltreatment 2022
Table 2–4 Child Protective Services Caseload, 2022
State
Investigation and Alternative
Response Workers
Completed Reports
(Reports with a Disposition)
Completed Reports per
Investigation and Alternative
Response Worker
Alabama 451 26,837 60
Alaska 238 6,627 28
Arizona 377 44,806 119
Arkansas 467 31,923 68
California - - -
Colorado - - -
Connecticut 409 12,709 31
Delaware 130 5,697 44
District of Columbia 130 4,039 31
Florida - - -
Georgia - - -
Hawaii 52 2,897 56
Idaho 174 7,465 43
Illinois 995 94,433 95
Indiana 711 102,320 144
Iowa 233 34,900 150
Kansas 251 23,095 92
Kentucky 853 37,894 44
Louisiana 181 17,742 98
Maine 157 9,289 59
Maryland - - -
Massachusetts 326 39,075 120
Michigan 1,407 68,359 49
Minnesota 517 25,662 50
Mississippi 442 28,282 64
Missouri 467 54,386 116
Montana 191 7,301 38
Nebraska 179 13,845 77
Nevada 175 16,117 92
New Hampshire 113 10,183 90
New Jersey 1,184 57,068 48
New Mexico
178 20,743 117
New York - - -
North Carolina 811 62,304 77
North Dakota - - -
Ohio - - -
Oklahoma 565 33,529 59
Oregon 446 36,174 81
Pennsylvania - - -
Puerto Rico 190 7,701 41
Rhode Island 81 4,597 57
South Carolina - - -
South Dakota 44 2,496 57
Tennessee 956 71,046 74
Texas 4,028 207,429 51
Utah 124 21,590 174
Vermont 53 3,457 65
Virginia 656 33,801 52
Washington 530 41,645 79
West Virginia 323 22,354 69
Wisconsin 257 23,009 90
Wyoming - - -
National 20,052 1,374,826 69
Reporting States 41 41 41
chApter 2: Reports 16

chApter 3: Children 17
Child Maltreatment 2022
Children
CHAPTER 3
This chapter discusses the children who are the subjects of reports (screened-in referrals) and
the characteristics of those who are determined to be victims of abuse and neglect. The Child
Abuse Prevention and Treatment Act (CAPTA), (P.L. 100–294) denes child abuse and neglect
as, at a minimum:
Any recent act or failure to act on the part of a parent or caretaker which results in
death, serious physical or emotional harm, sexual abuse or exploitation [ ]; or an act
or failure to act, which presents an imminent risk of serious harm.
The Justice for Victims of Trafcking Act (P.L. 114–22) added a legislation requirement to
include sex trafcking victims in the denition of child abuse and neglect. CAPTA recognizes
individual state authority by providing this minimum federal denition of child abuse and
neglect. Each state denes child abuse and neglect in its own statutes and policies and the
child welfare agencies determine the appropriate response for the alleged maltreatment based
on those statutes and policies. While the purpose of the National Child Abuse and Neglect
Data System (NCANDS) is to collect nationally standardized aggregate and case-level child
maltreatment data, readers should exercise caution in making state-to-state comparisons. States
map their own codes to the NCANDS codes.
In most states, the majority of reports receive an investigation. An investigation response
results in a determination (also known as a disposition) about the alleged child maltreatment.
The two most prevalent NCANDS dispositions are:
■ Substantiated: An investigation disposition that concludes the allegation of maltreatment
or risk of maltreatment is supported or founded by state law or policy. NCANDS includes
this disposition in the count of victims.
■ Unsubstantiated: An investigation disposition that concludes there is not sufcient
evidence under state law to conclude or suspect that the child was maltreated or is at risk
of being maltreated.
Less commonly used NCANDS dispositions for investigation responses include:
■ Indicated: A disposition that concludes maltreatment could not be substantiated under
state law or policy, but there is a reason to suspect that at least one child may have been
maltreated or is at risk of maltreatment. This disposition is applicable only to states that
distinguish between substantiated and indicated dispositions. NCANDS includes this
disposition in the count of victims.
■ Intentionally false: A disposition that concludes the person who made the allegation of
maltreatment knew that the allegation was not true.

Child Maltreatment 2022
■ Closed with no nding: A disposition that does not conclude with a specic nding
because the CPS response could not be completed. This disposition is often assigned when
CPS is unable to locate the alleged victim.
■ No alleged maltreatment: A disposition for a child who receives a CPS response, but
is not the subject of an allegation or any nding of maltreatment. Some states have laws
requiring all children in a household receive a CPS response if any child in the household
is the subject of a CPS response.
■ Other: States may use the category of “other” if none of the above is applicable. State
statutes also establish the level of evidence needed to determine a disposition of substanti
ated or indicated. See Appendix C, State Characteristics for each state’s level of evidence.
-
These statutes inuence how CPS agencies respond to the safety needs of the children who
are the subjects of child maltreatment reports.
Alternative Response
In some states, reports of maltreatment may not be investigated, but are instead assigned to
an alternative track, called alternative response, family assessment response, or differential
response. Cases receiving this response often include early determinations that the children
have a low or moderate risk of maltreatment. According to states, alternative responses usu
ally include the voluntary acceptance of CPS services and the agreement of family needs.
-
These cases do not result in a formal determination regarding the maltreatment allegation
or alleged perpetrator. The term disposition is used when referring to both investigation
response and alternative response. In NCANDS, alternative response is dened as:
■ Alternative response: The provision of a response other than an investigation that
determines if a child or family needs services. A determination of maltreatment is not
made and a perpetrator is not determined.
Variations in how states dene and implement alternative response programs continue. For
example, several states mention that they have an alternative response program that is not
reported to NCANDS. For some of these states, the alternative response programs provide
services for families regardless of whether there were any allegations of child maltreatment.
Some states restrict who can receive an alternative response by the type of abuse. For example,
several states mention that children who are alleged victims of sexual abuse must receive an
investigation response and are not eligible for an alternative response. Another variation in
reporting or reason why alternative response program data may not be reported to NCANDS is
that the program may not be implemented statewide. To test implementation feasibility, states
often rst pilot or phase in programs in select counties. Full implementation may depend on
the results of the initial implementation. Some states, or counties within states, implemented
an alternative response program and terminated the program a few years later. Readers are
encouraged to review Appendix D, State Commentary, for more information about these
programs.
chApter 3: Children 18

Child Maltreatment 2022
Unique and Duplicate Counts
All NCANDS reporting states have the ability to assign a unique identier, within the state,
to each child who receives a CPS response. These unique identiers enable two ways to
count children:
■ Duplicate count of children: Counting a child each time he or she is the subject of a
report. This count also is called a report-child pair. For example, a duplicate count of
children who received an investigation response or alternative response counts each child
for each CPS response.
■ Unique count of children: Counting a child once, regardless of the number of times he
or she is the subject of a report. For example, a unique count of victims by age counts the
child’s age in the rst report where the child has a substantiated or indicated disposition.
Children Who Received an Investigation or Alternative Response
(unique count of children)
For FFY 2022, 3,096,101 children received either an investigation or alternative response at a
rate of 42.4 children per 1,000 in the population. This is a 12.7 percent decrease in the number
of children from FFY 2018 when 3,546,154 children received an investigation or alternative
response at a rate of 47.9 per 1,000 children.
7
See exhibit 3–A and related notes.
Exhibit 3–A Child Disposition Rates, 2018–2022
Year
2018
2019
2020
2021
2022
Reporting States
52
52
52
51
52
Child Population of
Reporting States
73,977,376
73,661,476
73,982,567
71,764,371
72,969,166
Children Who Received
an Investigation or
Alternative Response
from Reporting States
3,546,154
3,500,991
3,151,631
2,969,487
3,096,101
National
Disposition
Rate per 1,000
Children
47.9
47.5
42.6
41.4
42.4
Child Population of
all 52 States
73,977,376
73,661,476
73,982,567
73,356,806
72,969,166
National Estimate/
Actual Number of
Children Who Received
an Investigation or
Alternative Response
3,546,154
3,500,991
3,151,631
3,035,000
3,096,101
e number of children is a unique count. e national disposition rate is computed by dividing the number of reported children who received an
investigation or alternative response by the child population of reporting states and multiplying by 1,000 and displayed as rounded to the tenth.
If fewer than 52 states report data in a given year, the national estimate of children who received an investigation or alternative response is
calculated by multiplying the national disposition rate (displayed as rounded) by the child population of all 52 states and dividing by 1,000. e
result is rounded to the nearest 1,000. If 52 states report data in a given year, the number of actual children who received an investigation or
alternative response reported by states is displayed.
At the state level, the percent change from FFY 2018 to FFY 2022 ranged from a 43.2 percent
decrease to a 45.1 percent increase. State explanations for changes in the number of children
who received a CPS response across the 5 years include changes to screening and assess
ment policies, and reductions due to the COVID-19 pandemic. Please see Appendix D, State
Commentary, for state-specic information about changes. Information about a change may be
in an earlier edition of Child Maltreatment.
-
See table 3–1, and related notes.
Children Who Received an Investigation or Alternative Response
by Disposition (duplicate count of children)
For FFY 2022, 3,732,871 children (duplicate count) are the subjects of reports (screened-in
referrals). A child may be a victim in one report and a nonvictim in another report, and in this
analysis, the child is counted both times. There are 16.1 percent of children who are classied
7
The national percent change was calculated using the national actual number of children who received a CPS response for
FFYs 2018 and 2022.
c
hApter 3: Children 19

Child Maltreatment 2022
as victims with dispositions of substantiated (14.8%) and indicated (1.3%).
8
The remaining
children are not determined to be victims or received an alternative response. See table 3–2,
exhibit 3–B, and related notes.
More than 16 percent of children received a disposition of substantiated or indicated and are counted as
maltreatment victims
Based on data from 52 states. See table 3–2.
Number of Child Victims (unique count of child victims)
In NCANDS, a victim is dened as:
■ Victim: A child for whom the state determined at least one maltreatment was substantiated
or indicated; and a disposition of substantiated or indicated was assigned for a child in a
report. This includes a child who died and the death was conrmed to be the result of child
abuse and neglect. A child may be a victim in one report and a nonvictim in another report.
For FFY 2022, 52 states reported 558,899 victims of child abuse and neglect. This equates
to a national rate of 7.7 victims per 1,000 children in the population. This is a 20.0 percent
decrease from the FFY 2018 actual number of victims 698,189 reported by 52 states. The
largest number of victims was for FFY 2018, the number of victims has been decreasing since
that year. (See exhibit 3–C and related notes.) States have different policies about what is
considered child maltreatment, the type of CPS responses (alternative and investigation), and
different levels of evidence required to substantiate an abuse allegation, all or some of which
may account for variations in victimization rates.
As discussed above, children with alternative response dispositions are not considered
maltreatment victims and do not have perpetrators. Children with indicated dispositions
are considered maltreatment victims. Readers are encouraged to read Appendix C, State
Characteristics and Appendix D, State Commentary, for more information. Information
about a change may be in an earlier edition of Child Maltreatment.
8
Beginning with FFY 2020, North Carolina recoded the disposition of children who would have previously received an
alternative response victim disposition to an indicated disposition. As discussed above, children with alternative response
dispositions are not considered maltreatment victims and do not have perpetrators. Children with indicated dispositions
are considered maltreatment victims.
Exhibit 3–B Children Who Received an Investigation or Alternative Response by
Disposition, 2022
chApter 3: Children 20

Exhibit 3–C Child Victimization Rates, 2018–2022
Year
2018
2019
2020
2021
2022
Reporting States
52
52
52
51
52
Child Population of
Reporting States
73,977,376
73,661,476
73,982,567
71,764,371
72,969,166
Victims from
Reporting States
698,189
677,099
619,480
588,630
558,899
National
Victimization
Rate per 1,000
Children
9.4
9.2
8.4
8.2
7.7
Child Population of
all 52 States
73,977,376
73,661,476
73,982,567
73,356,806
72,969,166
National Estimate/
Actual Number of
Victims
698,189
677,099
619,480
602,000
558,899
e number of victims is a unique count. e national victimization rate is calculated by dividing the number of victims from reporting states by the
child population of reporting states, multiplying by 1,000, and displayed as rounded to the tenth.
If fewer than 52 states report data in a given year, the national estimate/rounded number of victims is calculated by multiplying the national
victimization rate (displayed as rounded) by the child population of all 52 states and dividing by 1,000. e result is rounded to the nearest 1,000.
If 52 states report data in a given year, the number of actual victims reported by states is displayed.
At the state level, the percent change of victims of abuse and neglect ranges from a 48.0
percent decrease to a 14.5 percent increase from FFY 2018 to 2022. The FFY 2022 state
victimization rates range from a low of 1.6 to a high of 16.5 per 1,000 children. See table 3–3
and related notes. Comments about changes to legislation, child welfare policy, and practice
that may contribute to an increase or decrease in the number of victims are provided by states
in Appendix D, State Commentary. Reasons for differences across the 5 years as provided by
states include: one state changed its dispositions from alternative response victims to indicated,
several states resolved investigation or assessment backlogs, several states instituted new
screening and intake tools, two states completed and one state began their alternative response
implementation,
9
and a number of states cited the multiyear effects of the COVID-19 pandemic.
Information about a change may be in an earlier edition of Child Maltreatment.
Based on data from 52 states, the FFY 2022 rate of rst-time victims is 5.4 per 1,000 chil
dren in the population. Seventy percent of all victims are rst-time victims. States use the
disposition date of prior substantiated or indicated maltreatments to determine whether the
victim is a rst-time victim.
-
See table 3–4 and related notes.
Child Victim Demographics (unique count of child victims)
The youngest children are the most vulnerable to maltreatment. More than one-quarter
(27.3%) of victims are in the age range of birth through 2 years old. Infant victims younger
than 1 year are 14.7 percent of all victims. The victimization rate is highest for infant victims
younger than 1 year at 22.2 per 1,000 children in the population of the same age, which is
2.2 times the rate of victims who are 1 year at 9.9 per 1,000 children. Victims who are 2
or 3 years old have victimization rates of 9.3 and 8.8 victims per 1,000 children of those
respective ages in the population. Readers may notice some states have lower rates across age
groups than other states. The states with lower rates may assign low-risk cases to alternative
response or have other state policies or programs in place for maltreatment allegations. In
general, the rate of victimization decreases with the child’s age. See table 3–5, exhibit 3–D,
and related notes.
The percentages of child victims by sex are 52.5 percent for girls and 47.2 percent for boys. The
sex is unknown for 0.3 percent of victims. The FFY 2022 victimization rate for girls is 8.2 per
1,000 girls in the population, which is higher than the rate for boys at 7.1 per 1,000 boys in the
population. See table 3–6 and related notes.
9
Nebraska, Texas, and New Mexico.
Child Maltreatment 2022
chApter 3: Children 21

Exhibit 3–D Victims by Age, 2022
The youngest children are the most vulnerable to maltreatment
Based on data from 52 states. See table 3–5.
Most victims are one of three races or ethnicities—White 41.6 percent, Hispanic 23.7 percent,
and Black or African-American 21.7 percent. The racial distributions for all children in the
population are 48.8 percent White, 26.0 percent Hispanic, and 13.9 percent Black or African-
American. See table C–3 and related notes. For FFY 2022, American Indian or Alaska Native
children have the highest rate of victimization at 14.3 per 1,000 children in the population of the
same race or ethnicity and Black or African-American children have the second highest rate at
12.1 per 1,000 children in the population of the same race or ethnicity. See table 3–7 and related
notes.
Maltreatment Types
NCANDS collects all maltreatment type allegations, however only those maltreatments with
a disposition of substantiated or indicated are included in the Child Maltreatment report. The
Justice for Victims of Trafcking Act of 2015 includes an amendment to CAPTA by adding a
requirement to report the number of sex trafcking victims. States are instructed to include sex
trafcking by caregivers and noncaregivers and began reporting this data with their FFY 2018
data submissions to NCANDS.
10
Focus on Maltreatment Categories
(unique count of child victims and duplicate count of maltreatment types)
A child may be determined to be a victim multiple times within the same FFY and up to four
different maltreatment types in each victim report. A child also may be determined to be a
victim of the same maltreatment type multiple times in the same FFY, just not in the same
report. For example, a child may be the victim of neglect twice in the same year, but the neglect
maltreatment type cannot be present twice in the same victim report.
10
The Children’s Bureau Information Memoranda ACYF-CB-IM-15-05 dated July 16, 2015,
https://www.acf.hhs.gov/cb/policy-guidance/im-15-05
Child Maltreatment 2022
chApter 3: Children 22

Child Maltreatment 2022
chApter 3: Children 23
In this analysis, a victim who has more than one type of maltreatment is counted once per type.
This answers the question of how many different types of maltreatment do victims have, rather
than how many occurrences of each type, for example:
■ A victim with three reports of neglect is counted once in neglect.
■ A victim with one report with both neglect and physical abuse is counted once in neglect
and once in physical abuse.
■ A victim with two separate reports in the same FFY, one with neglect and a second report
with physical abuse, is counted once in neglect and once in physical abuse.
The FFY 2022 data shows three-quarters (74.3%) of victims experience neglect, 17.0 percent
are physically abused, 10.6 percent are sexually abused, and 0.2 percent are sex trafcked.
In addition, 3.4 percent of victims are reported with the “other” type of maltreatment. States
may code any maltreatment as “other” if it does not t in one of the NCANDS categories.
States with larger than average numbers or percentages of victims with the NCANDS “other”
maltreatment type may map state categories of threatened harm, threatened abuse, and threat
of family violence to the NCANDS “other” category.
11
See table 3–8 and related notes. A few
states have policies about conducting investigations into specic maltreatment types. Readers
are encouraged to review states’ comments (appendix D) about what is included in the
“other” maltreatment type category and for additional information on state policies related to
maltreatment types. See chapter 7 for special focus analyses on maltreatment types.
Perpetrator Relationship
(unique count of child victims and duplicate count of relationships)
In this section, data is analyzed by relationship of victims to their perpetrators. A victim
may be maltreated multiple times by the same perpetrator or by different combinations of
perpetrators (e.g., mother alone, mother and nonparent(s), two parents, etc.). This analysis
counts every combination of relationships for each victim in each report and, therefore, the
percentages total more than 100.0 percent.
The FFY 2022 data shows 89.0 percent of victims are maltreated by one or both parents.
The parent(s) could have acted together, acted alone, or acted with up to two other people to
maltreat the child. The parent categories with the largest percentages are victims maltreated
by a mother acting alone (37.4%), victims maltreated by a father acting alone (24.5%), and
victims maltreated by both parents (19.2%). See table 3–9 and related notes.
Perpetrators who are not the victim’s parent maltreated 15.8 percent of victims. The largest
categories in the nonparent group are relative(s) (5.8%), unmarried partner(s) of parent (3.7%),
and “other(s)” (3.4%). The NCANDS category of “other(s)” perpetrator relationship includes
any relationship that does not map to one of the NCANDS relationship categories. According
to states’ commentary, this category includes nonrelated adult, non-related child, foster
sibling, babysitter, household staff, clergy, and school personnel. See appendix D for more
information on what states include as “other” perpetrator relationship.
11
Florida, Hawaii, and Oregon.

Child Maltreatment 2022
chApter 3: Children 24
Risk Factors
Risk factors are characteristics of a child or caregiver that may increase the likelihood of child
maltreatment. NCANDS collects data for 9 child risk factors and 12 caregiver risk factors.
Risk factors can be difcult to accurately assess and measure, and therefore may go undetected
among many children and caregivers. Some states may not have the resources to gather infor
mation from other sources or agencies or the ability to collect or store certain information in
their child welfare system. In addition, some risk factors must be clinically diagnosed, which
may not occur during the investigation or alternative response. If the case is closed prior to
the diagnosis, the CPS agency may not be notied and the information will not be reported to
NCANDS. Caregivers with these risk factors who are included in each analysis may or may not
be the perpetrators responsible for the maltreatment. For FFY 2022, data is analyzed for care
giver risk factors with the following NCANDS denitions. Please see Appendix B, Glossary for
these and additional NCANDS denitions:
-
-
■ Alcohol abuse (caregiver): The compulsive use of alcohol that is not of a temporary nature.
■ Domestic violence (caregiver): Any abusive, violent, coercive, forceful, or threatening act
or word inicted by one member of a family or household on another. In NCANDS, the
caregiver may be the perpetrator or the victim of the domestic violence.
■ Drug abuse (caregiver): The compulsive use of drugs that is not of a temporary nature.
■ Inadequate housing: A risk factor related to substandard, overcrowded, or unsafe housing
conditions, including homelessness.
As not every state is able to report on every caregiver risk factor, the national percentages are
calculated only on the number of victims in states reporting each individual risk factor. Several
caregiver risk factors are not included in the FFY 2022 analysis that were included in previous
analyses due to data quality concerns. The largest percentages of victims with caregiver risk
factors are those reported with domestic violence and drug abuse. In 39 reporting states, 95,794
victims (23.8%) have the drug abuse caregiver risk factor and in 35 reporting states, 99,255
victims (26.5%) have the domestic violence caregiver factor. See table 3–10 and related notes.
Reporting Infants with Prenatal Substance Exposure Data to
NCANDS
12
CAPTA Section 106(d) Annual State Data Reports 18 (A) requests a count of infants with
prenatal substance exposure (IPSE). To be included in the count, a child must meet the follow
ing conditions as dened by NCANDS data elements:
-
■ Infant: the child must be in the age range of birth to 1 year old.
■ Referred to CPS by health care provider: the child must have the medical personnel report
source.
■ Born with and identied as being affected by substance abuse or withdrawal symptoms:
the child must have the alcohol abuse, drug abuse, or both alcohol and drug abuse child risk
factors.
12
The Comprehensive Addiction and Recovery Act (CARA) of 2016 amended CAPTA by adding a requirement to report the
number of infants with prenatal substance exposure (IPSE), the number of IPSE with a plan of safe care, and the number
of IPSE with a referral to appropriate services. States began reporting the new elds with their FFY 2018 NCANDS
submissions. Children’s Bureau Program Instruction ACYF-CB-PI-17-02 dated January 17, 2018,
https://www.acf.hhs.gov/cb/policy-guidance/pi-17-02.

Child Maltreatment 2022
chApter 3: Children 25
The legislation does not require the infants to be considered victims of maltreatment solely
based on the substance exposure; and drug abuse includes both legal and illegal drugs.
NCANDS uses the following denitions when discussing IPSE
13
:
■ Alcohol abuse (child risk factor): The compulsive use of alcohol that is not of a temporary
nature, includes Fetal Alcohol Syndrome, Fetal Alcohol Spectrum Disorder, and exposure
to alcohol during pregnancy.
■ Drug abuse (child risk factor): The compulsive use of drugs that is not of a temporary
nature, includes infants exposed to drugs during pregnancy.
■ Screened-in IPSE: Indicates the child is included in the state’s Child File. NCANDS
uses the existing elds of age, report source, and alcohol abuse and drug abuse child risk
factors to determine the count. These are children who were screened-in and were the
subjects of either an investigation or alternative response.
■ Screened-out IPSE: Indicates the child is included in the state’s Agency File. These
are children who were screened-out either because they did not meet the child welfare
agency’s criteria for a CPS response or because, in some states, there are special programs
outside of CPS for handling substance abuse.
■ Total IPSE: The sum of screened-in IPSE and screened-out IPSE.
Number of Infants with Prenatal Substance Exposure
(unique count of child victims)
FFY 2022 data shows 45,756 infants in 50 states being referred to CPS agencies as infants
with prenatal substance exposure. See table 3–11 and related notes. While the number of states
reporting IPSE for FFY 2022 is an increase from the 49 states that reported for FFY 2021,
the number of IPSE children decreased from 49,194 in FFY 2021 to 45,756 in FFY 2022. The
difference is mostly due to fewer IPSE children being screened-in to CPS for an investigation
or alternative response.
For FFY 2022, the majority (36,247 or 79.2%) of IPSE are screened-in to CPS to receive either
an investigation or alternative response. This is a decrease from FFY 2021 when 47 states
screened-in 40,799 IPSE. State explanations for the decrease in screened-in IPSE mostly refer
to better reporting. Of the screened-in IPSE, 82.4 percent have the drug abuse child risk factor,
0.5 percent have the alcohol abuse child risk factor and 17.0 percent have the alcohol and drug
abuse child risk factor.
14
For FFY 2022, thirty-six states reported one-fth (20.8%) of IPSE were screened-out. Some
states have policies and legislation prohibiting certain referrals from being screened-out and
some states have special programs or agencies specically for certain referrals. For example,
a state may routinely screen-out IPSE referrals to a special agency or program unless there
are additional maltreatment allegations that require an investigation. See Appendix D, State
Commentary, for more information about states’ screening policies and additional information
about states’ capabilities to collect and report data on these IPSE children.
13
CAPTA uses terms infants affected by substance abuse, prenatal drug exposure, infants affected by withdrawal symptoms,
and Fetal Alcohol Spectrum Disorder. In NCANDS, the term infants with prenatal substance exposure includes all of the
terms used by CAPTA.
14
Some states are not able to collect and report alcohol and drug abuse child risk factors separately and NCANDS guidance
is to report both risk factors for the same children. For this analysis, children with both risk factors are counted once in
the category screened-in IPSE with alcohol abuse and drug abuse child risk factor.

Child Maltreatment 2022
Screened-in Infants with Prenatal Substance Exposure Who Have a
Plan of Safe Care
(unique count of children)
CAPTA Section 106(d) Annual State Data Reports 18 (B) asks for the number of screened-
in IPSE who also have a plan of safe care as developed under subsection (b)(2)(B)(iii). For
FFY 2022, 33 states reported 23,781 screened-in IPSE (69.5%) have a plan of safe care.
See table 3–12 and related notes. This is an improvement in the number of states reporting, but
a decrease in the number of screened-in IPSE with a plan of safe care, which was 26,904 from
31 states in FFY 2021.
Screened-in Infants with Prenatal Substance Exposure Who Have a
Referral to Appropriate Services
(unique count of children)
CAPTA Section 106(d) Annual State Data Reports 18 (C) asks for the number of screened-in
IPSE who also had a referral to services as described under subsection (b)(2)(B)(iii). Thirty-
two states reported 22,883 screened-in IPSE (68.4%) have a referral to appropriate services.
See table 3–13 and related notes. What is considered an appropriate service is up to each state’s
determination and may depend on the needs of the specic case. According to comments
provided by the states, some examples of services that these children and families were referred
to include mental and behavioral health, foster care, substance abuse assessment and treat
ment, and other programs that facilitate early identication of at-risk children and caregivers
and links them with early intervention services, public health services, and community-based
resources.
-
Exhibit and Table Notes
The following pages contain the data tables referenced in chapter 3. Specic information
about state submissions can be found in Appendix D, State Commentary. Additional infor
mation regarding the exhibits and tables is provided below.
-
General
During data analyses, thresholds are set to ensure data quality is balanced with the need to
report data from as many states as possible. States may be excluded from an analysis for data
quality issues. Exclusion rules are listed in the individual table notes below. Not every table
has an exclusion rule or notes.
■ The data for all tables are from the Child File unless otherwise noted.
■ Rates are per 1,000 children in the population. Rates are calculated by dividing the relevant
reported count (child, victim, rst-time victim, etc.) by the child population count (children,
by age, etc.) and multiplying by 1,000.
■ Unless otherwise noted, the number of children and victims are unique counts.
■ The count of victims includes children with dispositions of substantiated or indicated.
■ Children with dispositions of alternative response victims are not included in the victim
count.
■ NCANDS uses the child population estimates that are released annually by the U.S. Census
Bureau. These population estimates are provided in Appendix C, State Characteristics.
■ The row labeled Reporting States displays the count of states that provided data for that
analysis.
■ National totals and calculations appear in a single row labeled National instead of separate
rows labeled total, rate, or percent.
■ Dashes are inserted into cells without any data.
chApter 3: Children 26

Child Maltreatment 2022
Table 3–1 Children Who Received an Investigation or Alternative Response,
2018–2022
■ The percent change was calculated by subtracting 2018 data from 2022 data, dividing the
result by 2018 data, and multiplying by 100.
Table 3–2 Children Who Received an Investigation or Alternative Response by
Disposition, 2022
■ The number of children is a duplicate count.
■ Many states conduct investigations for all children in a family when any child is the subject
of an allegation. In these states, a disposition of “no alleged maltreatment” is assigned to
siblings who are not the subjects of an allegation and are not found to be victims. These
children may receive an alternative response or an investigation.
Table 3–3 Child Victims, 2018–2022
■ The percent change is calculated by subtracting 2018 data from 2022 data, dividing the result
by 2018 data, and multiplying by 100.
Table 3–4 First-time Victims, 2022
■ States are instructed to check whether there was a disposition date of substantiated or
indicated associated with the same child prior to the disposition date of the current victim
report. States may have different abilities and criteria for how far back they check for rst-
time victims.
Table 3–5 Victims by Age, 2022
■ There are no population data for unknown age and, therefore, no rates.
Table 3–6 Victims by Sex, 2022
■ There are no population data for children with unknown sex and, therefore, no rates.
Table 3–7 Victims by Race or Ethnicity, 2022
■ Counts associated with each racial group are exclusive and do not include Hispanic ethnicity.
■ Only those states that have both race and ethnicity population data are included in this
analysis.
■ States are excluded from this analysis if more than 30.0 percent of victims are reported with
an unknown or missing race or ethnicity.
Table 3–8 Maltreatment Types of Victims (Duplicate Categories), 2022
■ The number of victims is a unique count and the number of maltreatment types is a
duplicate count.
■ This analysis counts victims with one or more maltreatment types but counts them only
once regardless of the number of times the child is reported as a victim of the maltreat
ment type.
-
■ A child may be a victim of more than one type of maltreatment and therefore the maltreat
ment type is a duplicate count.
-
chApter 3: Children 27

Child Maltreatment 2022
Table 3–9 Victims by Relationship to Their Perpetrators, 2022
■ The number of relationships is a duplicate count, and the number of victims is a unique
count. Percentages are calculated against the unique count of victims and total to more than
100.0 percent.
■ In NCANDS, a child victim may have up to three perpetrators. A few states’ systems do
not have the capability of collecting and reporting data for all three perpetrator elds. More
information may be found in Appendix D.
■ States are excluded from this analysis if more than 25.0 percent of perpetrators are reported
with an unknown or missing relationship.
■ States are excluded from this analysis if fewer than 85 percent of victims have one or more
perpetrators.
■ The relationship categories listed under nonparent perpetrator include any perpetrator
relationship that was not identied as an adoptive parent, a biological parent, or a stepparent.
■ The two parents of known sex category can include mother and father, two mothers, and two
fathers.
■ The two parents of known sex with nonparent category can include mother, father, and
nonparent; two mothers and nonparent; and two fathers and nonparent.
■ One or more parents of unknown sex can include up to three parents in any combination
of known and unknown sex. The parent(s) could have acted alone, together, or with a
nonparent.
■ Nonparent perpetrators counted in combination with parents (e.g., mother and nonparent(s))
are not also counted in the individual categories listed under nonparent.
■ Multiple nonparental perpetrators that are in the same category are counted within that
category. For example, two child daycare providers are counted as child daycare providers.
■ Multiple nonparental perpetrators that are in different categories are counted in more than
one nonparental perpetrator.
■ Some states are not able to collect and report on group home and residential facility staff
perpetrators due to system limitations or jurisdictional issues
Table 3–10 Victims with Caregiver Risk Factors, 2022
■ As states have varying abilities to report on caregiver risk factors, the national percentages
are calculated only on those states able to report the specic risk factor as shown in the
column labelled Victims in Reporting States.
■ A victim is counted only once if there is more than one report in which the victim is reported
with the caregiver risk factor.
■ The counts on this table are exclusive and follow a hierarchy rule. If a victim is reported both
with and without the caregiver risk factor, the victim is counted once with the caregiver risk
factor.
■ The category Any Caregiver Disability is the combination of six disability types. States
are excluded if fewer than 2.0 percent of victims are reported with the total combined
disabilities.
■ States are excluded from this analysis if fewer than 2.0 percent of victims are reported with
each specic caregiver risk factor.
■ States are included in this analysis if they are not able to differentiate between alcohol abuse
and drug abuse caregiver risk factors and reported both risk factors for the same children in
both caregiver risk factor categories.
chApter 3: Children 28

Child Maltreatment 2022
Table 3–11 Infants with Prenatal Substance Exposure by Submission Type,
2022
■ Data is from the Child File and Agency File.
■ States may be excluded from the count of screened-in referrals for incomplete reporting
Table 3–12 Screened-in Infants with Prenatal Substance Exposure Who Have a
Plan of Safe Care, 2022
■ This analysis uses a hierarchy, if a screened-in IPSE is reported with and without a plan of
safe care, the infant is counted once with the plan of safe care.
Table 3–13 Screened-in Infants with Prenatal Substance Exposure Who Have a
Referral to Appropriate Services, 2022
■ This analysis uses a hierarchy, if a screened-in IPSE is reported with and without the referral
to appropriate services, the infant is counted once with the referral to appropriate services.
chApter 3: Children 29

Child Maltreatment 2022
Table 3–1 Children Who Received an Investigation or Alternative Response,
2018–2022
(continues next page)
State 2018 2019 2020 2021 2022
Percent Change from
2018 to 2022
Alabama 38,634 39,335 36,931 36,139 36,538 -5.4
Alaska 12,749 14,429 15,460 10,816 9,799 -23.1
Arizona 87,862 82,336 77,146 - 54,687 -37.8
Arkansas 58,823 57,339 54,775 52,887 55,674 -5.4
California 360,040 343,536 306,919 271,487 292,782 -18.7
Colorado 44,698 45,849 43,483 43,197 41,159 -7.9
Connecticut 19,693 18,669 14,135 13,416 15,561 -21.0
Delaware 12,180 12,373 10,672 10,006 12,014 -1.4
District of Columbia 14,334 12,315 8,651 7,824 8,211 -42.7
Florida 292,518 285,141 251,149 256,060 251,757 -13.9
Georgia 164,147 157,705 121,595 106,948 104,979 -36.0
Hawaii 3,817 4,378 4,938 4,845 5,193 36.0
Idaho 12,825 13,385 12,769 12,850 10,666 -16.8
Illinois 146,141 151,490 140,762 142,309 158,622 8.5
Indiana 161,340 147,872 139,343 135,799 123,644 -23.4
Iowa 38,631 38,253 35,469 38,953 38,790 0.4
Kansas 27,816 32,877 29,552 26,134 24,366 -12.4
Kentucky 83,902 77,512 67,066 55,547 52,816 -37.1
Louisiana
26,064 27,366 23,553 20,623 23,633 -9.3
Maine 11,031 16,288 18,871 17,524 16,008 45.1
Maryland 32,244 32,196 29,852 21,367 23,038 -28.6
Massachusetts 76,244 72,962 62,829 65,918 65,920 -13.5
Michigan 158,673 161,058 129,271 127,759 138,996 -12.4
Minnesota 39,581 38,690 36,274 32,919 32,958 -16.7
Mississippi 40,682 38,838 33,450 34,732 36,698 -9.8
Missouri 81,059 67,322 62,059 59,129 60,422 -25.5
Montana 15,300 15,400 15,528 13,484 11,158 -27.1
Nebraska 24,476 25,312 25,964 29,093 27,634 12.9
Nevada 30,220 29,439 27,980 29,351 29,963 -0.9
New Hampshire 13,888 12,798 13,336 11,816 12,742 -8.3
New Jersey 77,661 78,741 70,179 66,321 74,766 -3.7
New Mexico 25,774 26,040 25,980 23,281 24,529 -4.8
New York 218,684 216,016 194,127 189,559 192,737 -11.9
North Carolina 124,647 124,639 115,472 109,236 113,162 -9.2
North Dakota 7,295 6,597 5,570 4,598 4,764 -34.7
Ohio 110,550 113,071 104,750 106,012 102,858 -7.0
Oklahoma 58,958 57,504 58,379 55,518 51,985 -11.8
Oregon
50,319
55,063 48,161 43,312 47,610 -5.4
Pennsylvania 42,295 41,062 35,447 34,167 39,414 -6.8
Puerto Rico 15,053 15,044 12,510 13,646 12,956 -13.9
Rhode Island 10,841 9,334 8,062 6,967 6,160 -43.2
South Carolina 82,617 84,872 63,067 63,843 65,470 -20.8
South Dakota 3,761 4,039 4,032 3,800 3,987 6.0
Tennessee 87,384 94,946 86,109 85,534 88,309 1.1
Texas 281,562 278,004 263,493 278,119 289,231 2.7
Utah 26,076 26,926 25,860 25,642 26,819 2.8
Vermont 4,485 4,429 3,178 2,902 3,790 -15.5
Virginia 49,156 49,338 44,902 44,037 44,896 -8.7
Washington 46,131 49,174 47,375 43,474 45,834 -0.6
West Virginia 52,276 53,491 49,128 46,595 46,198 -11.6
Wisconsin 36,103 35,105 32,062 30,191 30,556 -15.4
Wyoming 4,914 5,093 4,006 3,801 3,642 -25.9
National 3,546,154 3,500,991 3,151,631 2,969,487 3,096,101 N/A
Reporting States 52 52 52 51 52 -
chApter 3: Children 30

Child Maltreatment 2022
Table 3–1 Children Who Received an Investigation or Alternative Response,
2018–2022
State
2018 Rate per 1,000
Children
2019 Rate per 1,000
Children
2020 Rate per 1,000
Children
2021 Rate per 1,000
Children
2022 Rate per 1,000
Children
Alabama 35.4 36.1 33.2 32.6 32.9
Alaska 69.6 80.0 86.3 60.9 55.5
Arizona 53.6 50.2 48.4 - 34.4
Arkansas 83.6 81.8 78.6 76.0 79.9
California 40.1 38.7 34.8 31.4 34.4
Colorado 35.4 36.5 34.9 35.1 33.9
Connecticut 26.8 25.7 19.0 18.2 21.3
Delaware 59.7 60.6 51.6 48.4 57.7
District of Columbia 113.1 96.2 69.1 63.1 66.0
Florida 69.2 67.3 59.4 60.5 58.6
Georgia 65.4 62.9 48.3 42.7 41.8
Hawaii 12.6 14.6 16.1 16.1 17.5
Idaho 28.8 29.9 28.2 27.9 23.0
Illinois 51.1 53.8 49.7 51.3 58.3
Indiana 102.6 94.2 88.2 86.3 78.8
Iowa 52.9 52.5 48.4 53.5 53.5
Kansas 39.4 46.9 42.0 37.6 35.3
Kentucky 83.2 77.2 66.3 55.1 52.6
Louisiana 23.7 25.1 21.7 19.2 22.3
Maine 44.0 65.3 75.2 70.3 64.6
Maryland 24.0 24.1
21.8 15.8 17.1
Massachusetts 55.8
53.9 45.8 48.8 49.3
Michigan 73.3 75.1 60.0 60.0 65.9
Minnesota 30.4 29.7 27.6 25.3 25.5
Mississippi 57.5 55.5 48.4 50.8 54.1
Missouri 58.8 49.0 45.1 43.2 44.3
Montana 66.8 67.3 67.1 58.0 47.7
Nebraska 51.4 53.2 53.9 60.7 58.0
Nevada 43.9 42.4 40.4 42.5 43.4
New Hampshire 53.8 50.0 52.0 46.4 50.4
New Jersey 39.7 40.5 34.6 33.1 37.5
New Mexico 53.4 54.6 54.5 49.8 53.4
New York 53.7 53.6 46.6 46.6 48.3
North Carolina 54.1 54.1 50.6 47.9 49.3
North Dakota 40.9 36.5 30.2 25.1 26.1
Ohio 42.6 43.8 40.3 41.1 40.1
Oklahoma 61.7 60.3 61.5 58.4 54.5
Oregon 57.9 63.7 55.9 50.9 56.9
Pennsylvania 15.9 15.6 13.3 12.9 15.0
Puerto Rico 25.4 26.3 22.1 25.0 25.0
Rhode Island 52.6 45.8 38.5 33.7 30.2
South Carolina 74.5 76.2 57.3 57.8 58.6
South Dakota 17.4 18.5 18.6 17.5
18.2
Tennessee 57.9 62.8 56.4
56.0 57.4
Texas 38.1 37.5 35.6 37.6 38.8
Utah 28.0 29.0 27.6 27.4 28.8
Vermont 38.8 38.7 27.1 25.0 33.0
Virginia 26.3 26.4 23.8 23.5 24.0
Washington 27.8 29.6 28.3 26.2 27.8
West Virginia 143.2 148.4 137.1 131.3 131.3
Wisconsin 28.3 27.7 25.2 24.0 24.5
Wyoming 36.5 38.1 30.2 28.9 28.0
National 47.9 47.5 42.6 41.4 42.4
Reporting States - - - - -
chApter 3: Children 31

Child Maltreatment 2022
Table 3–2 Children Who Received an Investigation or Alternative Response
by Disposition, 2022
(continues next page)
State Substantiated Indicated Alternative Response Unsubstantiated Intentionally False
Alabama 11,941 - - 26,247 -
Alaska 2,794 - - 8,556 -
Arizona 5,058 8,482 - 49,607 -
Arkansas 9,363 - 6,873 27,212 -
California 53,973 - - 245,328 -
Colorado 10,572 - 16,053 22,410 -
Connecticut 5,394 - - 12,578 -
Delaware 1,104 - 2,939 5,715 -
District of Columbia 1,689 - - 4,547 -
Florida 25,697 - - 194,956 -
Georgia 10,820 - 37,000 31,402 -
Hawaii 1,342 - - 4,482 -
Idaho 2,065 - - 10,069 779
Illinois 37,077 - - 115,447 434
Indiana 20,184 - - 145,902 -
Iowa 13,150 - 11,402 31,642 -
Kansas 1,974 - - 29,044 -
Kentucky 13,492 - - 44,786 -
Louisiana 7,861 - - 16,783 -
Maine 2,575 1,519 - 10,255 -
Maryland 4,389 2,691 12,550 6,017 -
Massachusetts 24,582
- - 24,517 -
Michigan 14,195 10,721 - 80,570 3
Minnesota 5,521 - 22,741 8,256 -
Mississippi 9,797 - - 33,808 -
Missouri 4,004 - 48,411 20,112 -
Montana 2,895 18 - 10,136 -
Nebraska 2,126 - 7,556 14,032 -
Nevada 6,273 - 722 19,248 -
New Hampshire 1,053 - - 13,636 -
New Jersey 3,217 - - 86,159 -
New Mexico 6,616 - - 25,739 -
New York 57,297 - 17,172 167,144 -
North Carolina 7,730 17,073 86,414 18,368 -
North Dakota 1,154 - - 3,876 -
Ohio 17,037 7,640 50,675 42,691 -
Oklahoma 14,240 - 911 37,848 -
Oregon 11,397 - - 40,629 -
Pennsylvania 5,201 - - 34,574 -
Puerto Rico 4,957 170 - 6,141 87
Rhode Island 2,601 - - 4,325 -
South Carolina 15,680 - - 42,928 -
South Dakota 1,546 - - 2,742 -
Tennessee 6,351 673 68,276
20,332 -
Texas 55,942 - 50,458 191,942 -
Utah 9,253 - - 20,176 21
Vermont 761 - 1,619 2,172 22
Virginia 4,694 - 36,307 8,601 -
Washington 3,995 - 34,284 20,274 55
West Virginia 5,740 - - 30,506 -
Wisconsin 4,259 - 4,307 27,583 -
Wyoming 851 - 3,094 369 -
National 553,479 48,987 519,764 2,102,419 1,401
Reporting States 14.8 1.3 13.9 56.3 0.0
National States 52 9 21 52 7
chApter 3: Children 32

Child Maltreatment 2022
chApter 3: Children 33
Table 3–2 Children Who Received an Investigation or Alternative Response
by Disposition, 2022
State Closed with No Finding No Alleged Maltreatment Other Unknown Total Children
Alabama 1,297 - - 85 39,570
Alaska 988 - - - 12,338
Arizona 2,024 - - - 65,171
Arkansas 1,362 20,293 - - 65,103
California - 50,393 - - 349,694
Colorado - - - 361 49,396
Connecticut - - - - 17,972
Delaware 2,358 1,502 - - 13,618
District of Columbia 190 3,261 - 4 9,691
Florida - 80,920 - 844 302,417
Georgia - 44,860 - - 124,082
Hawaii - - - 39 5,863
Idaho - - - - 12,913
Illinois - 55,814 - - 208,772
Indiana - - - - 166,086
Iowa - - - 11 56,205
Kansas 378 - - - 31,396
Kentucky 1,495 - 3,161 - 62,934
Louisiana 1,309 - - - 25,953
Maine - 6,261 - - 20,610
Maryland - - - - 25,647
Massachusetts -
19,442 10,662 - 79,203
Michigan 693 68,885 - - 175,067
Minnesota 1,590 - - - 38,108
Mississippi 1,530 - - - 45,135
Missouri 1,351 - 355 59 74,292
Montana 459 - 108 - 13,616
Nebraska 400 10,796 - - 34,910
Nevada 700 9,425 - - 36,368
New Hampshire 811 - - 1 15,501
New Jersey - - - - 89,376
New Mexico - - - - 32,355
New York - 2,305 - - 243,918
North Carolina - 1,445 136 - 131,166
North Dakota 159 - - - 5,189
Ohio 5,530 - - - 123,573
Oklahoma 5,677 - - - 58,676
Oregon - - 5,946 1 57,973
Pennsylvania - - - - 39,775
Puerto Rico 927 2,121 - - 14,403
Rhode Island 85 - - - 7,011
South Carolina - 24,305 - - 82,913
South Dakota 191 - - - 4,479
Tennessee 7,303 - 1
78 103,014
Texas 2,813 - 19,282 3,245 323,682
Utah 2,026 - - - 31,476
Vermont - - - - 4,574
Virginia 50 488 - 5 50,145
Washington 2,332 - - - 60,940
West Virginia 3,558 10,324 - 11 50,139
Wisconsin - - - - 36,149
Wyoming - - - - 4,314
National 49,586 412,840 39,651 4,744 3,732,871
National Percent 1.3 11.1 1.1 0.1 100.0
Reporting States 29 18 8 13 52

Child Maltreatment 2022
chApter 3: Children 34
Table 3–3 Child Victims, 2018–2022 (continues next page)
Percent Change from
2018 to 2022State
2018 2019 2020
2021 2022
Alabama 12,158 11,677 11,663 11,840 11,618 -4.4
Alaska 2,615 3,059 3,212 2,733 2,581 -1.3
Arizona 15,504 12,847 9,954 - 12,324 -20.5
Arkansas 8,538 8,422 9,241 9,616 8,927 4.6
California 63,795 64,132 60,317 55,503 50,869 -20.3
Colorado 11,879 12,246 11,615 11,147 9,777 -17.7
Connecticut 7,652 8,042 6,346 5,570 5,032 -34.2
Delaware 1,251 1,248 1,200 1,131 1,077 -13.9
District of Columbia 1,699 1,857 1,568 1,647 1,574 -7.4
Florida 36,795 32,915 28,268 27,394 24,505 -33.4
Georgia 11,064 10,102 8,690 9,643 10,524 -4.9
Hawaii 1,265 1,342 1,294 1,322 1,228 -2.9
Idaho 1,919 1,869 1,958 2,268 2,005 4.5
Illinois 31,515 33,331 35,437 35,841 32,433 2.9
Indiana 25,731 23,029 22,648 21,556 19,185 -25.4
Iowa 11,764 11,648 10,600 11,271 11,150 -5.2
Kansas 3,188 2,945 2,386 2,140 1,861 -41.6
Kentucky 23,752 20,130 16,748 14,963 12,340 -48.0
Louisiana
9,380 8,441 6,859 6,422 7,572 -19.3
Maine 3,481 4,413 4,726 4,228 3,792 8.9
Maryland 7,743 7,661 7,242 6,303 6,564 -15.2
Massachusetts 25,812 25,029 22,538 22,654 22,075 -14.5
Michigan 37,703 33,043 26,932 24,515 23,500 -37.7
Minnesota 7,785 6,780 6,647 5,544 5,299 -31.9
Mississippi 10,002 9,377 8,136 8,526 9,028 -9.7
Missouri 5,662 4,762 4,449 4,262 3,932 -30.6
Montana 3,763 3,736 3,777 3,077 2,714 -27.9
Nebraska 2,596 2,822 2,376 2,471 2,026 -22.0
Nevada 5,109 4,990 5,016 5,547 5,851 14.5
New Hampshire 1,331 1,217 1,182 985 1,034 -22.3
New Jersey 6,008 5,132 3,655 3,188 3,146 -47.6
New Mexico 8,024 8,025 7,050 5,964 5,817 -27.5
New York 68,785 67,269 59,126 56,760 50,056 -27.2
North Carolina 27,280 26,449 23,480 21,643 23,134 -15.2
North Dakota 2,097 1,797 1,614 1,349 1,132 -46.0
Ohio 25,158 25,470 23,691 24,267 22,439 -10.8
Oklahoma 15,355 15,148 14,685 13,719 13,546 -11.8
Oregon
12,581
13,543 11,487 10,573 10,507 -16.5
Pennsylvania 4,695 4,817 4,582 4,683 5,005 6.6
Puerto Rico 4,381 4,738 3,572 4,753 4,320 -1.4
Rhode Island 3,644 3,183 2,743 2,588 2,444 -32.9
South Carolina 19,130 18,717 14,263 15,308 14,572 -23.8
South Dakota 1,426 1,537 1,570 1,459 1,451 1.8
Tennessee 9,186 9,859 8,687 7,739 6,924 -24.6
Texas 63,271 64,093 65,116 65,253 54,207 -14.3
Utah 10,122 10,579 9,694 9,233 8,765 -13.4
Vermont 958 851 530 392 672 -29.9
Virginia 6,132 6,159 5,658 4,944 4,563 -25.6
Washington 4,498 4,222 3,967 3,487 3,389 -24.7
West Virginia 6,946 6,727 6,116 6,094 5,510 -20.7
Wisconsin 5,017 4,576 4,177 4,229 4,082 -18.6
Wyoming 1,044 1,096 992 886 821 -21.4
National 698,189 677,099 619,480 588,630 558,899 N/A
Reporting States 52 52 52 51 52 -

chApter 3: Children 35
Child Maltreatment 2022
Table 3–3 Child Victims, 2018–2022
2018 Rate per 1,000
Children
2019 Rate per 1,000
Children
2020 Rate per 1,000
Children
2021 Rate per 1,000
Children
2022 Rate per 1,000
Children
State
Alabama 11.1 10.7 10.5 10.7 10.5
Alaska 14.3 17.0 17.9 15.4 14.6
Arizona 9.5 7.8 6.2 - 7.8
Arkansas 12.1 12.0 13.3 13.8 12.8
California 7.1 7.2 6.8 6.4 6.0
Colorado 9.4 9.7 9.3 9.0 8.0
Connecticut 10.4 11.1 8.5 7.6 6.9
Delaware 6.1 6.1 5.8 5.5 5.2
District of Columbia 13.4 14.5 12.5 13.3 12.6
Florida 8.7 7.8 6.7 6.5 5.7
Georgia 4.4 4.0 3.5 3.8 4.2
Hawaii 4.2 4.5 4.2 4.4 4.1
Idaho 4.3 4.2 4.3 4.9 4.3
Illinois 11.0 11.8 12.5 12.9 11.9
Indiana 16.4 14.7 14.3 13.7 12.2
Iowa 16.1 16.0 14.5 15.5 15.4
Kansas 4.5 4.2 3.4 3.1 2.7
Kentucky 23.6 20.0 16.6 14.9 12.3
Louisiana 8.5 7.7 6.3 6.0 7.1
Maine 13.9 17.7 18.8 17.0 15.3
Maryland 5.8 5.7
5.3 4.7 4.9
Massachusetts 18.9
18.5 16.4 16.8 16.5
Michigan 17.4 15.4 12.5 11.5 11.1
Minnesota 6.0 5.2 5.1 4.3 4.1
Mississippi 14.1 13.4 11.8 12.5 13.3
Missouri 4.1 3.5 3.2 3.1 2.9
Montana 16.4 16.3 16.3 13.2 11.6
Nebraska 5.4 5.9 4.9 5.2 4.3
Nevada 7.4 7.2 7.2 8.0 8.5
New Hampshire 5.2 4.8 4.6 3.9 4.1
New Jersey 3.1 2.6 1.8 1.6 1.6
New Mexico 16.6 16.8 14.8 12.8 12.7
New York 16.9 16.7 14.2 13.9 12.5
North Carolina 11.8 11.5 10.3 9.5 10.1
North Dakota 11.7 10.0 8.8 7.4 6.2
Ohio 9.7 9.9 9.1 9.4 8.8
Oklahoma 16.1 15.9 15.5 14.4 14.2
Oregon 14.5 15.7 13.3 12.4 12.6
Pennsylvania 1.8 1.8 1.7 1.8 1.9
Puerto Rico 7.4 8.3 6.3 8.7 8.3
Rhode Island 17.7 15.6 13.1 12.5 12.0
South Carolina 17.3 16.8 13.0 13.8 13.0
South Dakota 6.6 7.1 7.2 6.7
6.6
Tennessee 6.1 6.5 5.7 5.1 4.5
Texas 8.6 8.7 8.8 8.8 7.3
Utah 10.9 11.4 10.3 9.9 9.4
Vermont 8.3 7.4 4.5 3.4 5.9
Virginia 3.3 3.3 3.0 2.6 2.4
Washington 2.7 2.5 2.4 2.1 2.1
West Virginia 19.0 18.7 17.1 17.2 15.7
Wisconsin 3.9 3.6 3.3 3.4 3.3
Wyoming 7.8 8.2 7.5 6.7 6.3
National 9.4 9.2 8.4 8.2 7.7
Reporting States - - - - -

chApter 3: Children 36
Child Maltreatment 2022
Table 3–4 First-time Victims, 2022
State
First-time Victims First-time Victims Rate per 1,000 Children
Alabama 9,423 8.5
Alaska 1,676 9.5
Arizona 7,060 4.4
Arkansas 7,462 10.7
California 40,083 4.7
Colorado 6,683 5.5
Connecticut 3,553 4.9
Delaware 895 4.3
District of Columbia 1,088 8.7
Florida 11,046 2.6
Georgia 8,747 3.5
Hawaii 945 3.2
Idaho 1,695 3.7
Illinois 20,623 7.6
Indiana 13,632 8.7
Iowa 7,704 10.6
Kansas 1,669 2.4
Kentucky 7,903 7.9
Louisiana 6,063 5.7
Maine 2,044 8.2
Maryland 4,402 3.3
Massachusetts 12,206 9.1
Michigan 14,840 7.0
Minnesota 5,008 3.9
Mississippi 7,921 11.7
Missouri 3,420 2.5
Montana 2,173 9.3
Nebraska 1,557 3.3
Nevada 3,852 5.6
New Hampshire 847 3.3
New Jersey 2,574 1.3
New Mexico 3,955 8.6
New York 28,845 7.2
North Carolina 15,590 6.8
North Dakota 814 4.5
Ohio 16,217 6.3
Oklahoma 10,525 11.0
Oregon 6,730 8.0
Pennsylvania 4,724 1.8
Puerto Rico 3,941 7.6
Rhode Island 1,647 8.1
South Carolina 10,293 9.2
South Dakota 1,101 5.0
Tennessee 3,523
2.3
Texas 43,563 5.8
Utah 6,001 6.4
Vermont 561 4.9
Virginia 4,285 2.3
Washington 1,552 0.9
West Virginia 4,480 12.7
Wisconsin 3,415 2.7
Wyoming 629 4.8
National 391,185 5.4
Reporting States 52 -

chApter 3: Children 37
Child Maltreatment 2022
Table 3–5 Victims by Age, 2022 (continues next page)
State
<1 1 2
3 4 5 6 7 8 9
Alabama
2,009 731 669 689 604 600 593 534 500
475
Alaska
358 168 162 158 164 147 138 146 144
133
Arizona
2,995 749 742 703 621 623 572 539 496
479
Arkansas
1,985 474 477 461 481 395 490 381 365
349
California
8,425 3,156 2,908 2,775 2,649 2,723 2,737 2,575 2,511
2,405
Colorado
1,261 670 555 532 502 523 542 545 529
491
Connecticut
625 327 314 262 287 261 284 233 245
243
Delaware
119 61 57 60 58 64 62 62 63
47
District of Columbia
200 101 103 91 91 78 105 102 93
79
Florida
3,813 1,765 1,753 1,657 1,524 1,421 1,337 1,288 1,128
1,014
Georgia
1,711 572 552 568 568 593 618 627 540
516
Hawaii
170
73 48 79 65 62 65 56 64
59
Idaho
473 98 103 99 101 82 98 105 81
87
Illinois
3,992 2,463 2,212 2,273 2,146 2,010 1,953 1,836 1,693
1,671
Indiana
4,595 1,125 1,032 986 957 955 940 901 845
821
Iowa
1,777 744 773 687 680 640 639 554 590
516
Kansas
146 120 105 103 100 115 94 95 116
92
Kentucky
1,766 826 798 793 712 676 730 675 587
586
Louisiana
2,590 395 420 371 352 316 310 339 271
284
Maine
439 222 231 237 203 231 228 219 243
209
Maryland
476 336 336 355 343 316 366 325 277
324
Massachusetts
2,336 1,292 1,243 1,202 1,143 1,138 1,272 1,256 1,104
1,140
Michigan
2,703 1,641 1,599 1,448 1,383 1,445 1,345 1,261 1,255
1,110
Minnesota
744 329 327
304 328 342 283 243 274
260
Mississippi
1,172 469 476 416 448 459 497 462 451
432
Missouri
288 228 217 212 201 205 155 165 183
176
Montana
342 173 185 157 178 180 161 152 137
129
Nebraska
253 126 130 116 124 133 107 124 83
82
Nevada
903 422 392 388 349 344 353 302 328
275
New Hampshire
138 77 75 65 55 53 52 56 44
41
New Jersey
394 177 180 162 166 162 174 154 147
153
New Mexico
643 292 324 268 287 345 369 385 362
342
New York
4,642 2,967 2,955 2,839 2,628 2,833 2,904 2,822 2,822
2,663
North Carolina
2,939 1,506 1,429 1,386 1,277 1,316 1,295 1,252 1,199
1,142
North Dakota
223 76 75 79 69 67 71 65 58
41
Ohio
3,320 1,300 1,247 1,234 1,193
1,113 1,201 1,155 1,061
1,123
Oklahoma
2,063 959 957 862 816 803 791 700 714
644
Oregon
1,152 591 628 652 622 622 595 552 539
509
Pennsylvania
427 260 218 241 206 215 188 197 194
209
Puerto Rico
274 207 210 223 238 245 283 242 251
275
Rhode Island
327 180 166 154 125 131 157 115 133
113
South Carolina
2,107 965 961 857 798 793 815 770 703
731
South Dakota
278 117 110 97 98 86 85 67 65
54
Tennessee
1,568 362 285 299 278 274 291 276 265
257
Texas
10,075 4,330 3,991 3,928 3,554 3,446 2,763 2,579 2,327
2,159
Utah
719 424 440 426 428 435 425 456 463
419
Vermont
46 42 36 30 32 31 33 28 39
28
Virginia
565 312 299 288 255 252 223
227 199
203
Washington
353 252 244 246 198 202 199 182 144
163
West Virginia
847 311 293 301 306 289 315 301 293
272
Wisconsin
453 264 251 234 257 249 243 222 203
184
Wyoming
110 48 58 57 51 47 41 35 56
46
National
82,329 35,875 34,351 33,110 31,299 31,086 30,587 28,940 27,477
26,255
Reporting States
52 52 52 52 52 52 52 52 52
52
Child Maltreatment 2022
chApter 3: Children 38
Table 3–5 Victims by Age, 2022 (continues next page)
Unborn,
Unknown,
and 18–21
State
10 11 12
13 14 15 16 17
Total Victims
Alabama 473 488 552 592 632 627 433 315 102
11,618
Alaska 118 129 117 123 116 114 76 55 15
2,581
Arizona 463 466 438 518 479 554 511 364 12
12,324
Arkansas 352 311 387 448 494 398 381 245 53
8,927
California 2,272 2,388 2,449 2,416 2,363 2,358 2,123 1,600 36
50,869
Colorado 508 496 524 567 486 447 341 237 21
9,777
Connecticut 226 237 278 265 277 239 228 165 36
5,032
Delaware 51 61 54 57 55 49 50 44 3
1,077
District of Columbia 78 82 68 79 71 71 44 36 2
1,574
Florida 1,037 1,056 1,087 1,055 1,077 988 849 586 70
24,505
Georgia 504 442 531 547 530 522 377 197 9
10,524
Hawaii 56 66 63 66 67 59 51 50 9
1,228
Idaho 71 100 92 90 99 86 87 50 3
2,005
Illinois 1,524 1,418 1,479 1,418 1,303 1,241 1,026 707 68
32,433
Indiana 816 770 848 852 880 795 632 413 22
19,185
Iowa 542 464 490 504 474 451 355 253 17
11,150
Kansas 96 108 110 110 106 104 79 61 1
1,861
Kentucky 608 526 589 593 568 530 457 295 25
12,340
Louisiana 292 262 250 297 262 243 197 110 11
7,572
Maine 217 220 182 168 188 147 121 81 6
3,792
Maryland 336 350 431 488 421 411 380 281 12
6,564
Massachusetts 1,073 1,126 1,215 1,294 1,273 1,208 1,024 713 23
22,075
Michigan 1,069 1,055 1,149 1,218 1,154 1,125 910 619 11
23,500
Minnesota 271 257 255 250 270 242 175 128 17
5,299
Mississippi 438 455 489 512 570 572 427 272 11
9,028
Missouri 194 182 217 287 316 301 245 158 2
3,932
Montana 139 128 125 126 121 117 93 64 7
2,714
Nebraska 115 87 101 98 85 94 72 68 28
2,026
Nevada 274 230 241 254 259 230 166 134 7
5,851
New Hampshire 44 60 48 57 57 48 42 20 2
1,034
New Jersey 172 158 168 192 170 160 127 121 9
3,146
New Mexico 331 347 300 305 275 245 216 126 55
5,817
New York 2,626 2,629 2,764 2,796 2,754 2,700 2,195 1,410 107
50,056
North Carolina 1,129 1,118 1,164 1,228 1,177 1,039 894 527 117
23,134
North Dakota 43 42 48 41 50 27 27 15 15
1,132
Ohio 1,058 1,070 1,209 1,241 1,251 1,042 917 621 83
22,439
Oklahoma 613 572 613 592 588 508 414 267 70
13,546
Oregon 481 474 499 588 559 550 474 371 49
10,507
Pennsylvania 211 281 307 379 441 384 322 260 65
5,005
Puerto Rico 261 243 266 246 238 245 240 112 21
4,320
Rhode Island 112 130 110 117 98 106 89 61 20
2,444
South Carolina 690 694 678 707 725 694 551 283 50
14,572
South Dakota 61 69 49 45 54 49 36 25 6
1,451
Tennessee 303 342 427 376 355 360 329 221 56
6,924
Texas 2,099 2,063 2,163 2,183 2,049 1,789 1,541 900 268
54,207
Utah 405 448 452 564 588 575 579 507 12
8,765
Vermont 36 44 35 49 57 41 37 27 1
672
Virginia 187 207 215 239 255 211 180 133 113
4,563
Washington 143 174 195 187 155 146 112 92 2
3,389
West Virginia 279 301 261 272 243 249 238 123 16
5,510
Wisconsin 203 212 209 237 208 181 159 104 9
4,082
Wyoming 48 35 40 32 33 29 22 29 4
821
National 25,748 25,673 27,031 27,965 27,376 25,701 21,651 14,656 1,789
558,899
Reporting States
52 52 52 52 52 52 52 52 52 52

Child Maltreatment 2022
chApter 3: Children 39
Table 3–5 Victims by Age, 2022 (continues next page)
<1
Rate per
1,000 children
1
Rate per
1,000 child
ren
2
Rate per
1,00
0 child
ren
3
Rate per
1,00
0 child
ren
4
Rate per
1,00
0 child
ren
5
Rate per
1,00
0 child
ren
6
Rate per
1,00
0 child
ren
7
Rate per
1,00
0 child
ren
8
Rate per
1,00
0 child
ren
State
Alabama 34.7 12.8 11.7 11.9 10.1 9.9 9.6 8.6 8.2
Alaska 37.7 18.1 17.3 17.2 17.2 14.8 13.7 14.5 14.1
Arizona 38.1 9.9 9.5 8.8 7.6 7.4 6.6 6.0 5.6
Arkansas 55.2 13.4 13.4 12.7 12.9 10.5 12.7 9.8 9.5
California 19.8 7.8 6.9 6.4 6.0 5.9 5.8 5.4 5.3
Colorado 20.1 10.9 9.1 8.7 8.0 8.1 8.1 8.1 7.9
Connecticut 17.4 9.4 8.6 7.1 7.6 6.8 7.3 5.9 6.2
Delaware 11.0 5.9 5.3 5.6 5.3 5.7 5.4 5.4 5.5
District of Columbia 24.2 12.4 13.7 12.2 11.8 10.1 13.9 13.6 13.1
Florida 17.3 8.3 8.0 7.4 6.6 6.1 5.6 5.4 4.7
Georgia 13.7 4.7 4.4 4.5 4.3
4.4 4.5 4.5 3.9
Hawaii 10.8 4.8 3.0 4.9 3.9 3.7 3.8 3.2 3.7
Idaho 21.1 4.4 4.6
4.4 4.3 3.3 3.8 4.0 3.1
Illinois 30.5 18.9 16.2 16.3 15.0 13.7 13.0 12.1 11.3
Indiana 57.6 14.4 12.7 12.0 11.4 11.3 10.8 10.3 9.7
Iowa 48.3 20.6 20.7 18.4 17.6 16.3 15.9 13.7 14.6
Kansas 4.2 3.5 3.0 2.9 2.8 3.1 2.5 2.5 3.0
Kentucky 33.9 16.1 15.3 15.0 13.2 12.4 13.1 12.1 10.5
Louisiana 45.7 7.1 7.7 6.7 6.2 5.4 5.2 5.7 4.6
Maine 36.6 19.1 18.3 18.6 15.9 17.7 16.9 16.1 17.8
Maryland 6.9 5.0 4.8 5.0 4.7 4.3 4.9 4.3 3.7
Massachusetts 33.1 19.4 18.3 17.6 16.3 16.0 17.6 17.2 15.1
Michigan 25.8 15.9 14.8 13.3 12.4 12.7 11.6 10.7 10.7
Minnesota 11.5 5.2 4.9 4.5 4.8 4.8 3.9 3.3 3.8
Mississippi 33.7 13.6 13.8 11.9 12.6 12.9 13.7 12.6 12.3
Missouri 4.2 3.3 3.1 3.0 2.8 2.8 2.1
2.2 2.4
Montana 30.5 15.7 16.0 13.4 14.7 14.2 12.1 11.3 10.3
Nebraska 10.4 5.2 5.3 4.6 4.8 5.1 4.0 4.6 3.1
Nevada 26.9 12.5 11.2 10.8 9.6 9.3 9.2 7.8 8.5
New Hampshire 10.9 6.3 6.0 5.1 4.3 4.0 3.9 4.1 3.2
New Jersey 3.8 1.8 1.7 1.5 1.6 1.5 1.6 1.4 1.3
New Mexico 30.9 13.8 14.8 11.8 12.3 14.4 14.8 15.1 14.1
New York 21.6 14.7 14.0 13.3 12.1 12.9 13.1 12.7 12.8
North Carolina 24.2 12.8 12.1 11.7 10.6 10.7 10.4 9.9 9.6
North Dakota 22.1 7.7 7.6 8.0 6.8 6.4 6.6 6.1 5.6
Ohio 25.8 10.1 9.4 9.2 8.7 8.0 8.5 8.1 7.4
Oklahoma 43.2 20.2 19.7 17.5 16.2 15.5 14.8 13.0 13.2
Oregon 28.1 15.0 15.3
15.7 14.5 14.0 12.8 11.7 11.4
Pennsylvania 3.2 2.0 1.6 1.8 1.5 1.5 1.3 1.4 1.3
Puerto Rico 14.2
11.3 10.7 10.6 11.2 10.6 11.1 8.8 8.6
Rhode Island 31.0 18.1 15.7 14.3 11.4 11.8 13.8 10.2 11.9
South Carolina 37.1 17.1 16.9 15.0 13.6 13.4 13.4 12.5 11.4
South Dakota 24.3 10.5 9.4 8.2 8.2 7.1 6.9 5.5 5.3
Tennessee 19.2 4.5 3.5 3.7 3.4 3.3 3.4 3.2 3.1
T
exas 26.6 11.7 10.6 10.2 9.0 8.5 6.6 6.1 5.5
Utah 15.4 9.4 9.4 9.1 9.0 8.8 8.3 8.8 8.9
Vermont 8.6 8.1 6.5 5.3 5.5 5.1 5.3 4.4 6.0
Virginia 5.8 3.3 3.1 2.9 2.5 2.5 2.1 2.2 1.9
Washington 4.2 3.0 2.8 2.9 2.3 2.2 2.1 2.0 1.6
West Virginia 48.7 17.9 16.7 17.1 16.9 15.8 16.6 15.5 14.8
Wisconsin 7.4 4.4 4.0 3.7 4.0 3.8 3.6
3.2 3.0
Wyoming 17.9 7.9 9.3 9.0 7.8 6.8 5.7 4.8 7.7
National 22.2 9.9 9.3 8.8 8.1 7.9 7.6 7.1 6.8
Reporting S
tates
- - - - - - - - -

Child Maltreatment 2022
chApter 3: Children 40
Table 3–5 Victims by Age, 2022
State
9
Rate per
1,000 Children
10
Rate per
1,000 Children
11
Rate per
1,000 Children
12
Rate per
1,000 Children
13
Rate per
1,000 Children
14
Rate per
1,000 Children
15
Rate per
1,000 Children
16
Rate per
1,000 Children
17
Rate per
1,000 Children
Alabama 7.8 7.8 7.9 8.7 9.1 9.3 9.3 6.6 4.9
Alaska 13.0 11.7 12.7 11.7 12.3 11.6 11.6 8.0 5.8
Arizona 5.4 5.2 5.2 4.8 5.5 4.8 5.6 5.3 3.8
Arkansas 9.1 9.2 8.0 9.8 11.0 11.6 9.4 9.2 6.0
California 5.0 4.8 4.9 5.0 4.8 4.5 4.5 4.1 3.1
Colorado 7.4 7.6 7.2 7.4 7.9 6.5 6.0 4.6 3.2
Connecticut 6.1 5.6 5.7 6.6 6.1 6.0 5.1 4.9 3.5
Delaware 4.1 4.4 5.2 4.5 4.7 4.4 3.9 4.0 3.6
District of Columbia 11.0 11.1 12.2 11.0 13.2 12.1 12.4 8.1 6.8
Florida 4.3 4.4 4.4 4.5 4.2 4.1 3.8 3.3 2.3
Georgia 3.7 3.6 3.1 3.7 3.7
3.4 3.3 2.5 1.3
Hawaii 3.4 3.2 3.9 3.8 4.1 4.0 3.7 3.2 3.2
Idaho 3.4 2.7 3.8
3.4 3.2 3.4 3.0 3.1 1.8
Illinois 11.2 10.1 9.2 9.4 8.8 7.8 7.4 6.2 4.2
Indiana 9.4 9.4 8.8 9.5 9.3 9.3 8.4 6.8 4.4
Iowa 12.9 13.7 11.7 11.8 11.8 10.7 10.2 8.2 5.9
Kansas 2.4 2.5 2.8 2.7 2.7 2.5 2.5 1.9 1.5
Kentucky 10.5 11.0 9.5 10.4 10.2 9.4 8.8 7.7 5.0
Louisiana 4.9 5.0 4.5 4.2 4.8 4.1 3.8 3.2 1.8
Maine 15.3 15.9 16.0 12.6 11.4 12.2 9.4 7.8 5.2
Maryland 4.4 4.5 4.6 5.6 6.2 5.2 5.1 4.8 3.6
Massachusetts 15.5 14.5 15.0 15.9 16.6 15.7 14.8 12.5 8.6
Michigan 9.5 9.2 9.0 9.5 9.9 9.0 8.7 7.1 4.8
Minnesota 3.6 3.8 3.6 3.4 3.3 3.5 3.1 2.3 1.7
Mississippi 11.9 11.8 12.2 12.7 12.6 13.3 13.2 10.3 6.7
Missouri 2.3 2.6 2.4 2.8 3.6 3.8 3.6
3.0 2.0
Montana 9.8 10.4 9.7 9.3 9.1 8.4 8.2 6.6 4.7
Nebraska 3.1 4.4 3.3 3.7 3.5 3.0 3.3 2.6 2.5
Nevada 7.2 7.1 5.8 6.1 6.2 6.1 5.4 4.0 3.3
New Hampshire 2.9 3.1 4.2 3.3 3.8 3.6 3.0 2.6 1.2
New Jersey 1.4 1.6 1.4 1.5 1.7 1.4 1.3 1.1 1.0
New Mexico 13.2 12.7 13.1 10.9 10.8 9.4 8.4 7.6 4.4
New York 12.0 11.8 11.7 12.3 12.4 11.9 11.6 9.5 6.1
North Carolina 9.1 9.0 8.8 8.9 9.1 8.4 7.4 6.5 3.9
North Dakota 4.0 4.2 4.2 4.8 4.1 4.9 2.7 2.7 1.6
Ohio 7.9 7.5 7.6 8.3 8.3 8.1 6.7 6.0 4.1
Oklahoma 11.9 11.4 10.6 1
1.2 10.6 10.2 8.9 7.5 4.9
Oregon 10.8 10.2 9.9
10.2 11.7 10.7 10.6 9.4 7.4
Pennsylvania 1.4 1.4 1.9 2.0 2.5 2.8 2.4 2.0 1.7
Puerto Rico 9.0
8.2 7.4 7.7 7.0 6.7 6.7 6.3 2.9
Rhode Island 10.2 10.1 11.6 9.7 10.0 8.0 8.6 7.1 4.8
South Carolina 11.9 11.2 11.1 10.5 10.5 10.4 10.0 8.2 4.3
South Dakota 4.4 5.0 5.7 3.9 3.6 4.2 3.8 2.9 2.1
Tennessee 3.1 3.6 4.1 4.9 4.2 3.8 3.9 3.6 2.5
Texas 5.2 5.1 4.9 5.0 5.0 4.5 4.0 3.5 2.1
Utah 8.0 7.8 8.5 8.3 10.1 10.2 10.0 10.3 9.2
Vermont 4.4 5.5 6.7 5.2 7.2 7.9 5.6 5.1 3.7
Virginia 2.0 1.8 2.0 2.0 2.2 2.3 1.9 1.6 1.2
W
ashington 1.8 1.6 1.9 2.1 2.0 1.6 1.5 1.2 1.0
West Virginia 13.6 14.0 15.1 12.8 13.0 11.2 11.4 11.1 5.8
Wisconsin 2.7 2.9 3.0 2.9 3.2 2.7 2.3
2.1 1.4
Wyoming 6.3 6.6 4.7 5.2 4.0 4.0 3.5 2.7 3.7
National 6.5 6.3 6.3 6.5 6.5
6.2 5.8 5.0 3.4
Reporting S
tates
- - - - - - - - -

Child Maltreatment 2022
chApter 3: Children 41
Table 3–6 Victims by Sex, 2022
Boy Rate per
1,000 Children
Girl Rate per
1,000 ChildrenState
Boy Girl Unknown
Total Victims
Alabama 5,273 6,332 13 11,618 9.3 11.6
Alaska 1,236 1,332 13 2,581 13.7 15.5
Arizona 5,991 6,107 226 12,324 7.4 7.9
Arkansas 3,969 4,954 4 8,927 11.1 14.6
California 24,123 26,689 57 50,869 5.5 6.4
Colorado 4,599 5,178 - 9,777 7.4 8.7
Connecticut 2,387 2,606 39 5,032 6.4 7.3
Delaware 490 587 - 1,077 4.6 5.7
District of Columbia 783 789 2 1,574 12.4 12.9
Florida 11,587 12,745 173 24,505 5.3 6.1
Georgia 5,031 5,484 9 10,524 3.9 4.5
Hawaii 555 662 11 1,228 3.6 4.6
Idaho 923 1,082 - 2,005 3.9 4.8
Illinois 16,041 16,273 119 32,433 11.5 12.2
Indiana 9,102 10,072 11 19,185 11.3 13.2
Iowa 5,435 5,704 11 11,150 14.7 16.1
Kansas 812 1,049 - 1,861 2.3 3.1
Kentucky 6,012 6,257 71
12,340 11.7 12.8
Louisiana 3,733 3,812 27 7,572 6.9 7.3
Maine 1,829 1,956 7 3,792 14.4 16.2
Maryland 2,726 3,809 29 6,564 4.0 5.8
Massachusetts 10,579 11,104 392 22,075 15.5 17.0
Michigan 11,534 11,947 19 23,500 10.7 11.6
Minnesota 2,474 2,825 - 5,299 3.7 4.5
Mississippi 4,048 4,959 21 9,028 11.7 14.9
Missouri 1,579 2,352 1 3,932 2.3 3.5
Montana 1,351 1,360 3 2,714 11.2 12.0
Nebraska 937 1,089 - 2,026 3.8 4.7
Nevada 2,831 3,020 - 5,851 8.0 9.0
New Hampshire 509 525 - 1,034 3.9 4.3
New Jersey 1,334 1,807 5 3,146 1.3 1.9
New Mexico 2,772 3,007 38 5,817 11.8 13.4
New York 24,490 25,544 22 50,056 12.0 13.1
North Carolina 11,160 11,959 15 23,134 9.5 10.6
North Dakota 551 579 2 1,132 5.9 6.5
Ohio 10,130 12,256 53 22,439 7.7 9.8
Oklahoma 6,581 6,951 14 13,546
13.5 14.9
Oregon 4,813
5,669 25 10,507 11.2 13.9
Pennsylvania 1,829 3,176 - 5,005 1.4 2.5
Puerto Rico 2,080 2,239 1 4,320 7.9 8.8
Rhode Island 1,206 1,228 10 2,444 11.6 12.3
South Carolina 7,176 7,338 58 14,572 12.6 13.4
South Dakota 670 780 1 1,451 6.0 7.3
Tennessee 2,657 4,230 37 6,924 3.4 5.6
Texas 24,966 28,939 302 54,207 6.6 7.9
Utah 3,887 4,842 36 8,765 8.1 10.7
Vermont 273 399 - 672 4.6 7.2
Virginia 2,177 2,385 1 4,563 2.3 2.6
Washington 1,531 1,850 8 3,389 1.8 2.3
West Virginia 2,660 2,822 28 5,510 14.7 16.5
Wisconsin 1,768 2,286 28 4,082 2.8 3.8
Wyoming 409 412 - 821 6.1 6.5
National 263,599 293,358 1,942 558,899 7.1 8.2
Reporting States 52 52 41 52 - -
Child Maltreatment 2022
chApter 3: Children 42
Table 3–7 Victims by Race or Ethnicity, 2022 (continues next page)
State
American
Indian or
Alaska Native Asian
Black or
African-
American Hispanic
Native
Hawaiian or
Other Pacic
Islander
Two or More
Races White
Unknown
Number Total Victims
Alabama 6 27 3,479 611 9 323 7,038 125 11,618
Alaska 1,354 16 39 81 66 370 509 146 2,581
Arizona 521 31 1,064 3,580 25 463 3,033 3,607 12,324
Arkansas 8 17 1,698 744 41 784 5,506 129 8,927
California 462 1,257 6,633 29,198 122 1,135 9,584 2,478 50,869
Colorado 112 86 1,118 4,099 29 449 3,592 292 9,777
Connecticut 8 42 1,045 1,817 3 324 1,652 141 5,032
Delaware 0 3 507 178 0 28 361 - 1,077
District of Columbia 0 1 1,080 136 1 11 10 335 1,574
Florida 11 91 7,112 4,272 15 1,321 10,415 1,268 24,505
Georgia 5 23 4,302 862 5 549 4,565 213 10,524
Hawaii 1 88 19
32 336 494 195 63 1,228
Idaho 23 2 9 255 5 65 1,085 561 2,005
Illinois 10 374 10,362 6,366 10 1,030 14,034 247 32,433
Indiana 4 95 3,374 1,813 11 1,545 12,284 59 19,185
Iowa 151 72 1,682 1,235 63 357 7,537 53 11,150
Kansas 6 10 204 299 2 150 1,154 36 1,861
Kentucky 8 24 1,195 603 9 629 9,338 534 12,340
Louisiana 17 18 3,626 180 7 262 3,169 293 7,572
Maine 31 8 87 142 6 174 2,650 694 3,792
Maryland 1 72 2,279 703 4 250 1,607 1,648 6,564
Massachusetts 43 318 2,804 7,105 17 1,328 8,108 2,352 22,075
Michigan 88 93 7,287 1,910 10 2,369 11,705 38 23,500
Minnesota 469 169 695 816 4 1,065 1,889 192 5,299
Mississippi 15 9 3,653 279 5 258 4,499
310 9,028
Missouri 7 9 435 325 5 73 2,745
333 3,932
Montana 418 2 31 136 0 193 1,908 26 2,714
Nebraska 133 20 263 366 5 171 941 127 2,026
Nevada 25 45 1,596 1,774 68 471 1,471 401 5,851
New Hampshire 2 10 28 79 1 41 787 86 1,034
New Jersey 1 35 873 1,103 2 80 987 65 3,146
New Mexico 547 6 145 3,316 1 102 999 701 5,817
New York 172 1,300 13,612 15,319 24 2,448 16,829 352 50,056
North Carolina 601 93 7,789 2,853 48 1,331 9,761 658 23,134
North Dakota 268 3 92 64 4 91 527 83 1,132
Ohio 13 44 5,669 1,433 19 2,435 12,467 359 22,439
Oklahoma 980 44 1,388 2,392 42 3,429 5,227 44 13,546
Oregon 247 56 340 1,335 55 417 5,616 2,441 10,507
Pennsylvania 4
38 1,020 783 2 303 2,639 216 5,005
Puerto Rico -
- - - - - - - -
Rhode Island 5 20 294 759 1 209 1,106 50 2,444
South Carolina 27 16 5,688 1,000 13 468 6,197 1,163 14,572
South Dakota 640 5 36 95 3 184 449 39 1,451
Tennessee - - - - - - - - -
Texas 81 363 11,468 25,441 82 2,041 13,837 894 54,207
Utah 156 72 312 2,201 202 232 5,494 96 8,765
Vermont 1 4 15 5 0 10 594 43 672
Virginia 2 29 1,118 561 6 285 2,353 209 4,563
Washington 130 43 209 702 66 500 1,562 177 3,389
West Virginia 1 3 138 74 0 380 4,862 52 5,510
Wisconsin 191 74 907 500 4 204 2,122 80 4,082
Wyoming 37 3 31 116 1
6 594 33 821
National 8,043 5,
283 118,850 130,048 1,459 31,837 227,59 3 24,542 547,655
Reporting States 50 50 50 50 50 50 50 49 50

Child Maltreatment 2022
chApter 3: Children 43
Table 3–7 Victims by Race or Ethnicity, 2022
State
American
Indian or
Alaska Native
Rate per 1,000
Children
Asian Rate per
1,000 Children
Black or
African-
American
Rate per 1,000
Children
Hispanic Rate
per 1,000
Children
Native
Hawaiian or
Other Pacic
Islander Rate
per 1,000
Children
Two or More
Races Rate per
1,000 Children
White Rate per
1,000 Children
Alabama 1.5 1.6 10.8 6.3 14.3 7.7 11.2
Alaska 42.0 1.6 7.6 4.3 15.5 15.2 6.2
Arizona 7.3 0.6 12.4 5.0 8.2 6.6 5.1
Arkansas 1.6 1.3 13.8 8.0 8.2 26.7 12.8
California 15.2 1.1 15.6 6.6 4.0 2.5 4.7
Colorado 17.2 2.0 20.3 10.3 12.2 7.6 5.5
Connecticut 3.9 1.1 12.0 9.1 8.4 10.8 4.4
Delaware 0.0 0.3 9.3 4.8 0.0 2.3 3.8
District of Columbia 0.0 0.3 16.8 6.2 19.6 1.9 0.3
Florida 1.3 0.7 8.4 3.1 4.9 7.6 5.9
Georgia 1.1 0.2 5.0 2.2 2.1 5.2 4.4
Hawaii 2.4 1.4 3.8 0.5 10.1 5.2 4.8
Idaho 5.4 0.3 2.2 2.8 5.8 3.7 3.2
Illinois 2.7 2.4
24.7 9.4 12.8 10.0 10.3
Indiana 1.6 2.1 18.3 9.5 14.2 21.8 11.4
Iowa 61.0 3.6 39.2 15.3 26.6
11.5 13.8
Kansas 1.4 0.5 4.8 2.2 2.0 3.9 2.6
Kentucky 6.3 1.2 12.7 8.4 8.4 13.5 12.1
Louisiana 2.8 1.0 9.5 2.0 19.4 7.2 6.0
Maine 16.6 2.3 10.1 16.7 58.8 17.4 12.3
Maryland 0.4 0.8 5.5 2.9 7.4 3.4 3.0
Massachusetts 18.0 3.0 22.5 26.1 22.7 22.7 10.5
Michigan 7.7 1.2 21.2 10.2 15.5 21.8 8.5
Minnesota 26.5 2.0 4.8 6.7 3.5 15.3 2.2
Mississippi 3.8 1.3 13.1 7.6 22.4 13.3 13.6
Missouri 1.5 0.3 2.4 3.2 1.6 1.1 2.8
Montana 19.9 1.0 21.6 8.0 0.0 16.9 10.6
Nebraska 27.3 1.4 9.0 4.0 13.2 8.3 3.0
Nevada 5.1 1.0 20.3 6.2 12.3 9.2 6.8
New Hampshire 5.0 1.1 5.2 4.0 10.9 4.6 3.8
New Jersey
0.3 0.2 3.2 1.9 2.1 1.2 1.1
New Mexico 12.2 1.0 16.8 11.7 4.5 7.9 9.6
New York 14.0 3.6 23.1
15.2 11.6 15.5 9.0
North Carolina 24.6 1.1 15.2 7.0 25.2 12.1 8.5
North Dakota 21.1 0.9 10.5 4.6 16.4 10.4 3.9
Ohio 3.6 0.6 14.3 7.9 12.7 17.9 7.0
Oklahoma 11.0 2.0 18.5 13.1 14.5 34.4 10.9
Oregon 29.4 1.5 17.0 6.8 12.4 7.4 11.0
Pennsylvania 1.2 0.3 3.0 2.1 2.0 2.6 1.6
Puerto Rico - - - - - - -
Rhode Island 5.3 2.6 19.4 12.8 6.4 20.8 10.0
South Carolina 8.5 0.7 17.8 8.3 15.6 9.3 10.3
South Dakota 25.5 1.3 4.8 5.2 11.0 16.8 2.9
Tennessee - - - - - - -
Texas 4.6 1.0 12.2 7.0 11.7 9.3 6.1
Utah 21.0 3.9 26.9 12.2 18.0 6.2 8.3
Vermont 3.6 1.5 6.8 1.4 0.0 2.1
5.9
Virginia 0.5 0.2 3.0 2.0 4.9 2.5 2.5
Washington 6.6 0.3 2.8 1.8 4.4 3.4 1.8
West Virginia 2.1 1.1 10.6 6.7 0.0 23.0 15.8
Wisconsin 15.0 1.5 8.2 3.1 6.6 3.7 2.5
Wyoming 10.9 3.0 24.8 5.5 12.0 1.3 6.0
National 14.3 1.3 12.1 7.0 9.3 9.4 6.6
Reporting States - - - - - - -

Child Maltreatment 2022
chApter 3: Children 44
Table 3–8 Maltreatment Types of Victims (Duplicate Categories), 2022 (continues next page)
State Victims
Me
dical
Neglect Neglect Other Physical Abuse
Psychological
Maltreatment Sexual Abuse Sex Trafcking Unknown
Total
Maltreatment
Typ es
Alabama 11,618 75 4,823 - 6,221 14 2,028 5 - 13,166
Alaska 2,581 79 1,899 - 610 891 252 3 - 3,734
Arizona 12,324 14 11,001 - 1,298 862 581 - - 13,756
Arkansas 8,927 - 6,089 262 1,592 185 1,860 12 - 10,000
California 50,869 64 45,022 249 3,496 3,963 3,451 74 - 56,319
Colorado 9,777 141 8,007 - 953 211 1,064 - 37 10,413
Connecticut 5,032 130 4,330 - 310 1,355 426 1 - 6,552
Delaware 1,077 15 327 161 237 301 195 - - 1,236
District of Columbia 1,574 - 1,416 - 214 - 38 15 - 1,683
Florida 24,505 888 14,463 9,350 2,201 313 2,390 - - 29,605
Georgia 10,524 293 7,137 - 1,484 2,052 652 43
- 11,661
Hawaii 1,228 17 229 1,108 101 12 83 9 - 1,559
Idaho 2,005 10 1,536 13 368 - 187 1 - 2,115
Illinois 32,433 656 25,470 27 5,273 81 3,823 - - 35,330
Indiana 19,185 - 16,517 - 1,324 - 2,284 49 - 20,174
Iowa 11,150 101 9,730 - 1,172 115 648 18 - 11,784
Kansas 1,861 42 880 - 408 287 402 6 - 2,025
Kentucky 12,340 269 11,002 - 1,146 89 756 - - 13,262
Louisiana 7,572 - 6,757 15 768 19 406 6 - 7,971
Maine 3,792 - 2,452 - 930 1,252 239 - - 4,873
Maryland 6,564 - 3,765 - 1,346 12 1,974 - - 7,097
Massachusetts 22,075 - 20,608 4 1,796 - 794 310 - 23,512
Michigan 23,500 570 19,936 - 3,794 156 1,282 17 - 25,755
Minnesota 5,299 - 3,621
- 708 125 1,408 10 - 5,872
Mississippi 9,028 464 6,275 31 1,441 1,644 1,296 25 - 11,176
Missouri 3,932 118 2,090 1 1,236 500 1,246 14 - 5,205
Montana 2,714 14 2,613 1 166 12 107 2 - 2,915
Nebraska 2,026 1 1,706 - 253 15 171 20 - 2,166
Nevada 5,851 84 4,985 - 943 6 458 - - 6,476
New Hampshire 1,034 39 911 - 102 64 68 4 - 1,188
New Jersey 3,146 60 2,114 - 449 18 652 3 - 3,296
New Mexico 5,817 205 4,801 - 738 1,403 207 - - 7,354
New York 50,056 2,677 48,806 1,329 4,715 433 2,161 13 - 60,134
North Carolina 23,134 712 15,349 205 2,436 3,741 1,971 3 314 24,731
North Dakota 1,132 10 995 - 97 78 26 - - 1,206
Ohio 22,439
373 10,101 - 10,467 1,439 4,111 7 - 26,498
Oklahoma 13,546 271 9,950 - 1,774 4,609 704 8 - 17,316
Oregon 10,507 - 4,350 5,953 1,228 181 1,196 - - 12,908
Pennsylvania 5,005 168 560 5 2,323 45 2,145 44 - 5,290
Puerto Rico 4,320 573 2,897 24 861 2,248 218 2 - 6,823
Rhode Island 2,444 28 1,423 64 341 902 111 - - 2,869
South Carolina 14,572 257 8,287 - 6,926 777 777 123 - 17,147
South Dakota 1,451 - 1,304 - 154 28 80 - - 1,566
Tennessee 6,924 87 1,688 - 3,587 170 2,449 141 - 8,122
Texas 54,207 861 43,788 2 6,403 309 7,150 26 - 58,539
Utah 8,765 36 2,170 102 3,498 3,233 1,684 18 - 10,741
Vermont 672 24 22 - 394 2 263 2 - 707
Virginia 4,563 84 3,016
3 1,148 75 703
2 - 5,031
Washington 3,389 - 2,514 - 767 - 477 20 - 3,778
West Virginia 5,510 301 2,459 - 4,197 3,508 273 - - 10,738
Wisconsin 4,082 49 2,593 7 617 17 1,053 28 - 4,364
Wyoming 821 3 661 9 15 278 64 - - 1,030
National 558,899 10,863 415,445 18,925 95,026 38,030 59,044 1,084 351 638,768
Reporting States 52 41 52 23 52 47 52 36 2 52

chApter 3: Children 45
Child Maltreatment 2022
Table 3–8 Maltreatment Types of Victims (Duplicate Categories), 2022
State
Medical
Neglect
Percent
Neglect
Percent Other Percent
Physical Abuse
Percent
Psychological
Maltreatment
Percent
Sexual Abuse
Percent
Sex Trafcking
Percent
Unknown
Percent
Total
Maltreatment
Types Percent
Alabama 0.6 41.5 - 53.5 0.1 17.5 0.0 - 113.3
Alaska 3.1 73.6 - 23.6 34.5 9.8 0.1 - 144.7
Arizona 0.1 89.3 - 10.5 7.0 4.7 - - 111.6
Arkansas - 68.2 2.9 17.8 2.1 20.8 0.1 - 112.0
California 0.1 88.5 0.5 6.9 7.8 6.8 0.1 - 110.7
Colorado 1.4 81.9 - 9.7 2.2 10.9 - 0.4 106.5
Connecticut 2.6 86.0 - 6.2 26.9 8.5 0.0 - 130.2
Delaware 1.4 30.4 14.9 22.0 27.9 18.1 - - 114.8
District of Columbia - 90.0 - 13.6 - 2.4 1.0 - 106.9
Florida 3.6 59.0 38.2 9.0 1.3 9.8 - - 120.8
Georgia 2.8 67.8 - 14.1 19.5 6.2 0.4 - 110.8
Hawaii 1.4 18.6
90.2 8.2 1.0 6.8 0.7 - 127.0
Idaho 0.5 76.6 0.6 18.4 - 9.3 0.0 - 105.5
Illinois 2.0 78.5 0.1 16.3 0.2 11.8 - - 108.9
Indiana - 86.1 - 6.9 - 11.9 0.3 - 105.2
Iowa 0.9 87.3 - 10.5 1.0 5.8 0.2 - 105.7
Kansas 2.3 47.3 - 21.9 15.4 21.6 0.3 - 108.8
Kentucky 2.2 89.2 - 9.3 0.7 6.1 - - 107.5
Louisiana - 89.2 0.2 10.1 0.3 5.4 0.1 - 105.3
Maine - 64.7 - 24.5 33.0 6.3 - - 128.5
Maryland - 57.4 - 20.5 0.2 30.1 - - 108.1
Massachusetts - 93.4 0.0 8.1 - 3.6 1.4 - 106.5
Michigan 2.4 84.8 - 16.1 0.7 5.5 0.1 - 109.6
Minnesota - 68.3 - 13.4 2.4 26.6 0.2 - 110.8
Mississippi 5.1 69.5 0.3 16.0 18.2 14.4
0.3 - 123.8
Missouri 3.0 53.2 0.0 31.4 12.7 31.7 0.4
- 132.4
Montana 0.5 96.3 0.0 6.1 0.4 3.9 0.1 - 107.4
Nebraska 0.0 84.2 - 12.5 0.7 8.4 1.0 - 106.9
Nevada 1.4 85.2 - 16.1 0.1 7.8 - - 110.7
New Hampshire 3.8 88.1 - 9.9 6.2 6.6 0.4 - 114.9
New Jersey 1.9 67.2 - 14.3 0.6 20.7 0.1 - 104.8
New Mexico 3.5 82.5 - 12.7 24.1 3.6 - - 126.4
New York 5.3 97.5 2.7 9.4 0.9 4.3 0.0 - 120.1
North Carolina 3.1 66.3 0.9 10.5 16.2 8.5 0.0 1.4 106.9
North Dakota 0.9 87.9 - 8.6 6.9 2.3 - - 106.5
Ohio 1.7 45.0 - 46.6 6.4 18.3 0.0 - 118.1
Oklahoma 2.0 73.5 - 13.1 34.0 5.2 0.1 - 127.8
Oregon - 41.4 56.7 11.7 1.7 11.4 - - 122.9
Pennsylvania
3.4 11.2 0.1 46.4 0.9 42.9 0.9 - 105.7
Puerto Rico 13.3
67.1 0.6 19.9 52.0 5.0 0.0 - 157.9
Rhode Island 1.1 58.2 2.6 14.0 36.9 4.5 - - 117.4
South Carolina 1.8 56.9 - 47.5 5.3 5.3 0.8 - 117.7
South Dakota - 89.9 - 10.6 1.9 5.5 - - 107.9
Tennessee 1.3 24.4 - 51.8 2.5 35.4 2.0 - 117.3
Texas 1.6 80.8 0.0 11.8 0.6 13.2 0.0 - 108.0
Utah 0.4 24.8 1.2 39.9 36.9 19.2 0.2 - 122.5
Vermont 3.6 3.3 - 58.6 0.3 39.1 0.3 - 105.2
Virginia 1.8 66.1 0.1 25.2 1.6 15.4 0.0 - 110.3
Washington - 74.2 - 22.6 - 14.1 0.6 - 111.5
West Virginia 5.5 44.6 - 76.2 63.7 5.0 - - 194.9
Wisconsin 1.2 63.5 0.2 15.1 0.4 25.8 0.7 - 106.9
Wyoming 0.4 80.5 1.1 1.8
33.9 7.8 - - 125.5
National 1.9 74.3 3
.4 17.0 6.8 10.6 0.2 0.1 114.3
Reporting States - - - - - - - - -

chApter 3: Children 46
Child Maltreatment 2022
Table 3–9 Victims by Relationship to Their Perpetrators, 2022
Perpetrator Vi
ctims
Reported
Relationships
Reported
Relationships Percent
PARENT
- - -
Father Only
-
125,489 24.5
Father and Nonparent
-
5,397 1.1
Mother Only
-
191,450 37.4
Mother and Nonparent
-
29,204 5.7
Two Parents of known sex
-
98,538 19.2
Three Parents of known sex
-
619 0.1
Two Parents of known sex and Nonparent
-
4,019 0.8
One or more Parents of Unknown Sex
-
1,162 0.2
Total Parents
-
455,878 89.0
NONPARENT
-
-
-
Child Daycare Provider(s) - 2,091 0.4
Foster Parent(s) - 1,754 0.3
Friend(s) and Neighbor(s) - 3,958 0.8
Group Home and Residential Facility Staff - 924 0.2
Legal Guardian(s) - 1,731 0.3
Other Professional(s) -
1,277 0.2
Relative(s) -
29,919 5.8
Unmarried Partner(s) of Parent -
19,196 3.7
Other(s) -
17,489 3.4
More Than One Nonparental Perpetrator - 2,318 0.5
Total Nonparents - 80,657 15.8
TOTAL UNKNOWN - 15,633 3.1
National 512,077 552 ,168 107.8
Based on data from 48 states.

chApter 3: Children 47
Child Maltreatment 2022
Table 3–10 Victims with Caregiver Risk Factors, 2022 (continues next page)
State
Victims
in Reporting
States Alcohol Abuse
Alcohol Abuse
Percent
Victims
in Reporting
States
Domestic
Violence
Domestic
Violence
Percent
Alabama 11,618 720 6.2 - - -
Alaska 2,581 1,398 54.2 2,581 1,192 46.2
Arizona - - - - - -
Arkansas - - - 8,927 800 9.0
California - - - - - -
Colorado - - - - - -
Connecticut - - - - - -
Delaware 1,077 176 16.3 1,077 428 39.7
District of Columbia 1,574 485 30.8 1,574 349 22.2
Florida - - - 24,505 9,072 37.0
Georgia - - - 10,524 333 3.2
Hawaii 1,228 230 18.7 1,228 431 35.1
Idaho 2,005 256 12.8 - - -
Illinois - - - - - -
Indiana 19,185 731 3.8 19,185 2,180 11.4
Iowa - - - - - -
Kansas - - - - - -
Kentucky 12,340 1,761 14.3 12,340 6,184 50.1
Louisiana - - - - - -
Maine 3,792 579 15.3 3,792 817 21.5
Maryland 6,564 174 2.7 6,564 294 4.5
Massachusetts 22,075 10,286 46.6 22,075 10,097 45.7
Michigan - - - 23,500 1,686 7.2
Minnesota 5,299 529 10.0 5,299 1,362 25.7
Mississippi 9,028 509 5.6 9,028 963 10.7
Missouri 3,932 318 8.1 3,932 267 6.8
Montana 2,714 163 6.0 2,714 120 4.4
Nebraska 2,026 336 16.6 2,026 86 4.2
Nevada 5,851 1,757 30.0 5,851 1,104 18.9
New Hampshire 1,034 106 10.3 1,034 464 44.9
New Jersey 3,146 373 11.9 3,146 724 23.0
New Mexico 5,817 1,117 19.2 - - -
New York 50,056 8,758 17.5 50,056 13,639 27.2
North Carolina 23,134 1,435 6.2 23,134 3,867 16.7
North Dakota - - - - - -
Ohio - - - 22,439 5,883 26.2
Oklahoma
13,546 2,535 18.7 13,546 5,241 38.7
Oregon 10,507
4,846 46.1 10,507 4,278 40.7
Pennsylvania - - - - - -
Puerto Rico 4,320 610 14.1 4,320 1,309 30.3
Rhode Island 2,444 245 10.0 2,444 1,180 48.3
South Carolina - - - - - -
South Dakota 1,451 536 36.9 1,451 385 26.5
Tennessee - - - - - -
Texas 54,207 2,524 4.7 54,207 19,658 36.3
Utah 8,765 1,081 12.3 8,765 2,636 30.1
Vermont - - - - - -
Virginia - - - 4,563 880 19.3
Washington 3,389 899 26.5 3,389 672 19.8
West Virginia 5,510 502 9.1 - - -
Wisconsin 4,082 108 2.6 4,082 485 11.9
Wyoming 821 171 20.8 821 189 23.0
National
305,118 46,254 15.2
374,626 99,255 26.5
Reporting States
33 33 -
35 35 -

chApter 3: Children 48
Child Maltreatment 2022
Table 3–10 Victims with Caregiver Risk Factors, 2022
State
Victims
in Reporting
States Drug Abuse
Drug Abuse
Percent
Victims
in Reporting
States
Inadequate
Housing
Inadequate
Housing Percent
Alabama 11,618 5,940 51.1 11,618 630 5.4
Alaska 2,581 819 31.7 2,581 210 8.1
Arizona - - - - - -
Arkansas 8,927 218 2.4 8,927 430 4.8
California - - - - - -
Colorado - - - - - -
Connecticut - - - 5,032 131 2.6
Delaware 1,077 345 32.0 1,077 211 19.6
District of Columbia 1,574 485 30.8 1,574 141 9.0
Florida 24,505 570 2.3 24,505 1,860 7.6
Georgia 10,524 623 5.9 - - -
Hawaii 1,228 524 42.7 1,228 93 7.6
Idaho 2,005 812 40.5 2,005 329 16.4
Illinois - - - - - -
Indiana 19,185 3,442 17.9 19,185 1,405 7.3
Iowa - - - 11,150 353 3.2
Kansas - - - - - -
Kentucky
12,340 6,117 49.6 12,340 2,727 22.1
Louisiana
- - - - - -
Maine 3,792 794 20.9 3,792 195 5.1
Maryland 6,564 467 7.1 - - -
Massachusetts 22,075 10,286 46.6 22,075 1,066 4.8
Michigan 23,500 600 2.6 - - -
Minnesota 5,299 951 17.9 5,299 551 10.4
Mississippi 9,028 3,134 34.7 9,028 1,523 16.9
Missouri 3,932 916 23.3 3,932 728 18.5
Montana 2,714 432 15.9 - - -
Nebraska 2,026 573 28.3 - - -
Nevada 5,851 1,766 30.2 5,851 462 7.9
New Hampshire 1,034 330 31.9 1,034 85 8.2
New Jersey 3,146 656 20.9 3,146 221 7.0
New Mexico 5,817 1,490 25.6 5,817 150 2.6
New York 50,056 8,800 17.6 - - -
North Carolina 23,134 4,518 19.5 23,134 1,220 5.3
North Dakota - - - - - -
Ohio 22,439 11,386 50.7 22,439 2,998 13.4
Oklahoma 13,546
5,107 37.7 13,546 652 4.8
Oregon 10,507
4,874 46.4 10,507 777 7.4
Pennsylvania - - - - - -
Puerto Rico 4,320 645 14.9 4,320 370 8.6
Rhode Island 2,444 299 12.2 2,444 74 3.0
South Carolina - - - 14,572 2,215 15.2
South Dakota 1,451 676 46.6 1,451 313 21.6
Tennessee 6,924 837 12.1 6,924 187 2.7
Texas 54,207 9,500 17.5 54,207 2,248 4.1
Utah 8,765 2,027 23.1 8,765 566 6.5
Vermont - - - - - -
Virginia - - - - - -
Washington 3,389 1,565 46.2 3,389 578 17.1
West Virginia 5,510 2,664 48.3 - - -
Wisconsin 4,082 226 5.5 4,082 216 5.3
Wyoming 821 380 46.3 821 146 17.8
National
401,937 95,794 23.8
331,797 26,061 7.9
Reporting States
39 39 -
35 35 -

chApter 3: Children 49
Child Maltreatment 2022
Table 3–11 Infants with Prenatal Substance Exposure by Submission Type, 2022
State
Screened-in IPSE
with Alcohol Abuse
Child Risk Factor
Screened-in IPSE
with Drug Abuse
Child Risk Factor
Screened-in IPSE
with Alcohol Abuse
and Drug Abuse Child
Risk Factor
Total Screened-in
IPSE Screened-out IPSE Total IPSE
Alabama 2 542 - 544 1 545
Alaska - - 82 82 104 186
Arizona - - - - 169 169
Arkansas 20 1,622 2 1,644 3 1,647
California - 36 2,934 2,970 579 3,549
Colorado - 23 - 23 826 849
Connecticut - - - - 92 92
Delaware - 332 1 333 19 352
District of Columbia - 109 - 109 - 109
Florida - - - - 40 40
Georgia 46 2,370 82 2,498 1,138 3,636
Hawaii - 20 8 28 - 28
Idaho 6 169 - 175 2 177
Illinois - - 680 680 - 680
Indiana 2 570 3 575 59 634
Iowa - 30 - 30 7 37
Kansas - - 29
29 18 47
Kentucky 8 757 5 770 381 1,151
Louisiana
12 2,092 - 2,104 40 2,144
Maine - - - - 327 327
Maryland - 11 - 11 0 11
Massachusetts - 36 1,345 1,381 177 1,558
Michigan 3 6,633 19 6,655 1,598 8,253
Minnesota 5 1,497 7 1,509 250 1,759
Mississippi 1 67 - 68 213 281
Missouri - 19 - 19 273 292
Montana 1 19 1 21 - 21
Nebraska 2 155 2 159 19 178
Nevada - 2 745 747 - 747
New Hampshire - 86 - 86 - 86
New Jersey 3 394 6 403 - 403
New Mexico 1 131 3 135 274 409
New York 1 561 5 567 - 567
North Carolina 3 1,210 - 1,213 693 1,906
North Dakota - - - - - -
Ohio 6 5,309 44 5,359
1,683 7,042
Oklahoma 17 2,248 66 2,331 25 2,356
Oregon -
23 - 23 - 23
Pennsylvania - - - - - -
Puerto Rico - 9 1 10 - 10
Rhode Island - - 70 70 4 74
South Carolina - 533 1 534 109 643
South Dakota - 36 1 37 47 84
Tennessee - 134 - 134 - 134
Texas 59 1,131 - 1,190 4 1,194
Utah - 179 - 179 - 179
Vermont - - - - 102 102
Virginia - - 18 18 90 108
Washington - 253 - 253 40 293
West Virginia - 528 3 531 - 531
Wisconsin - - - - 56 56
Wyoming - 8 2 10 47 57
National 198 29,884 6,165 36,247 9,509 45,756
National Percent
N/A N/A N/A 79.2 20.8 100.0
Percent of
Screened-in IPSE
0.5 82.4 17.0 100.0 N/A N/A
Reporting States
19 39 28 44 36 50

chApter 3: Children 50
Child Maltreatment 2022
Table 3–12 Screened-in Infants with Prenatal Substance Exposure Who
Have a Plan of Safe Care, 2022
State
Screened-in IPSE
Screened-in IPSE Who Have a Plan
of Safe Care
Screened-in IPSE Who Have a Plan
of Safe Care Percent
Alabama 544 231 42.5
Alaska - - -
Arizona - - -
Arkansas 1,644 1,419 86.3
California 2,970 1,313 44.2
Colorado 23 2 8.7
Connecticut - - -
Delaware 333 322 96.7
District of Columbia 109 95 87.2
Florida - - -
Georgia 2,498 1,775 71.1
Hawaii - - -
Idaho 175 142 81.1
Illinois - - -
Indiana 575 309 53.7
Iowa 30 30 100.0
Kansas 29 1 3.4
Kentucky 770 142 18.4
Louisiana 2,104 1,240 58.9
Maine - - -
Maryland - - -
Massachusetts 1,381 869 62.9
Michigan 6,655 6,445 96.8
Minnesota 1,509 1,299 86.1
Mississippi - - -
Missouri - - -
Montana - - -
Nebraska 159 30 18.9
Nevada 747 48 6.4
New Hampshire 86 55 64.0
New Jersey 403 121 30.0
New Mexico 135 45 33.3
New York 567
480 84.7
North Carolina 1,213 1,131 93.2
North Dakota - - -
Ohio 5,359 4,701 87.7
Oklahoma 2,331 48 2.1
Oregon 23 3 13.0
Pennsylvania - - -
Puerto Rico 10 10 100.0
Rhode Island - - -
South Carolina - - -
South Dakota 37 12 32.4
Tennessee 134 132 98.5
Texas 1,190 1,190 100.0
Utah 179 36 20.1
Vermont - - -
Virginia 18 13 72.2
Washington 253 92 36.4
West Virginia - - -
Wisconsin - - -
Wyoming - - -
National 34,193 23,781 69.5
Reporting States 33 33 -

chApter 3: Children 51
Child Maltreatment 2022
Table 3–13 Screened-in Infants with Prenatal Substance Exposure Who
Have a Referral to Appropriate Services, 2022
State
Screened-in IPSE
Screened-in IPSE Who Have a
Referral to Appropriate Services
Screened-in IPSE Who Have a
Referral to Appropriate Services
Percent
Alabama 544 248 45.6
Alaska - - -
Arizona - - -
Arkansas 1,644 1,418 86.3
California 2,970 1,020 34.3
Colorado 23 3 13.0
Connecticut - - -
Delaware 333 136 40.8
District of Columbia 109 93 85.3
Florida - - -
Georgia 2,498 1,775 71.1
Hawaii - - -
Idaho 175 149 85.1
Illinois - - -
Indiana 575 159 27.7
Iowa 30 28 93.3
Kansas 29 1 3.4
Kentucky 770 178 23.1
Louisiana 2,104 1,428 67.9
Maine - - -
Maryland - - -
Massachusetts 1,381 1,333 96.5
Michigan 6,655 5,815 87.4
Minnesota 1,509 390 25.8
Mississippi - - -
Missouri - - -
Montana - - -
Nebraska 159 111 69.8
Nevada - - -
New Hampshire 86 52 60.5
New Jersey 403 121 30.0
New Mexico 135 44
32.6
New York 567
436 76.9
North Carolina 1,213 1,127 92.9
North Dakota - - -
Ohio 5,359 4,217 78.7
Oklahoma 2,331 1,188 51.0
Oregon 23 4 17.4
Pennsylvania - - -
Puerto Rico 10 7 70.0
Rhode Island - - -
South Carolina - - -
South Dakota 37 5 13.5
Tennessee 134 132 98.5
Texas 1,190 1,123 94.4
Utah 179 36 20.1
Vermont - - -
Virginia 18 14 77.8
Washington 253 92 36.4
West Virginia - - -
Wisconsin - - -
Wyoming - - -
National 33,446 22,883 68.4
Reporting States 32 32 -

chApter 4: Fatalities 52
Child Maltreatment 2022
Fatalities
The effects of child abuse and neglect are serious, and a child fatality is the most tragic
consequence. The National Child Abuse and Neglect Data System (NCANDS) collects case-
level data in the Child File on child deaths from maltreatment. Additional counts of child
fatalities, for which case-level data is not known, are reported in the Agency File.
Some child maltreatment deaths may not come to the attention of child protective services
(CPS) agencies. Reasons for this include if there were no surviving siblings in the family,
or if the child had not (prior to his or her death) received child welfare services. To improve
the counts of child fatalities in NCANDS, states consult data sources outside of CPS for
deaths attributed to child maltreatment. The Child and Family Services Improvement and
Innovation Act (P.L. 112–34) lists the following additional data sources, which states must
include a description of in their state plan or explain why they are not used to report child
deaths due to maltreatment: state vital statistics departments, child death review teams,
law enforcement agencies, and ofces of medical examiners or coroners. In addition to the
sources mentioned in the law, some states also collect child fatality data from hospitals,
health departments, juvenile justice departments, and prosecutor and attorney general ofces.
States that can provide these additional data do so as aggregate data in the Agency File.
After the passage of the Child and Family Services Improvement and Innovation Act, several
states mentioned that they implemented new child death reviews or expanded the scope of
existing reviews. Some states began investigating all unexplained infant deaths regardless of
whether there was an allegation of maltreatment.
The child fatality count in this report reects the federal scal year (FFY) in which the
deaths are determined as due to maltreatment. The year in which a determination is made
may be different from the year in which the child died. CPS agencies may need more time
to determine a child died due to maltreatment. The time needed to conclude if a child was a
victim of maltreatment often does not coincide with the timeframe for concluding that the
death was a result of maltreatment, due to multiple-agency involvement and multiple levels
of review for child deaths. The “date of death” eld in the NCANDS Child File indicates the
day, month, and year in which the child died.
Number of Child Fatalities
For FFY 2022, a national estimate of 1,990 children died from abuse and neglect at a rate
of 2.73 per 100,000 children in the population. The 2022 national estimate is a 12.7 percent
increase from the 2018 actual number of child fatalities of 1,765.
15
See exhibit 4–A and
CHAPTER 4
15
The percent change is calculated using the actual reported number for FFY 2018 and FFY 2022.
chApter 4: Fatalities 53
Child Maltreatment 2022
related notes on how the national estimate is calculated. Due to the relatively low frequency
of child fatalities, the national rate and national estimate are sensitive to which states report
data and changes in the child population estimates produced by the U.S. Census Bureau.
Detailed explanations for data uctuations may be found in Appendix D, State Commentary.
An explanation for a change may be in an earlier edition of the Child Maltreatment
report. Previous editions of the report are located on the Children’s Bureau website at
https://www.acf.hhs.gov/cb/data-research/child-maltreatment.
At the state level for FFY 2022, 51 states reported 1,955 fatalities. Of those states, 46 reported
case-level data on 1,609 fatalities and 37 reported aggregate data on 346 fatalities. Fatality
rates by state range from 0.00 to 10.62 per 100,000 children in the population. See table 4–1
and related notes. All states are required to conrm fatality counts during data submission and
validation.
The total child fatalities reported by states in the Child File and Agency File uctuated during
the past 5 years, which is partly due to the number of states reporting. See table 4–2 and
related notes. The number of reported fatalities increased from 1,852 for FFY 2021 to 1,955
for FFY 2022. While not every state had an explanation for the increases, one state noted
improved reporting and resubmitted multiple prior years to include additional fatalities, one
state cited increased violence, and one cited increased fentanyl and opioid related deaths.
16
The state with the largest decrease conrmed a decrease in deaths due to unsafe sleep condi-
tions, drownings, vehicle-related deaths, and physical abuse. This state also cited a change in
the neglect denition.
17
Readers are encouraged to review the fatality comments provided by
states in Appendix D.
Child Fatality Demographics
Younger children are the most vulnerable to death as the result of child abuse and neglect.
See table 4–3, exhibit 4–B, and related notes. FFY 2022 data shows that 66.1 percent of child
fatalities are younger than 3 years. Close to one-half (44.7%) of child fatalities are younger
than 1 year, a fatality rate of 24.37 per 100,000 children in that age range. This is 3.4 (rounded)
times the fatality rate for 1-year-old children (7.14 per 100,000 children in the population of the
same age). The child fatality rates mostly decrease with age.
Exhibit 4–A Child Fatality Rates per 100,000 Children, 2018–2022
Year Reporting States
Child Population of
Reporting States
Child Fatalities
from Reporting
States
National Fatality
Rate Per 100,000
Children
Child Population of
all 52 States
National Estimate/
Actual Number of
Child Fatalities
2018 52
73,977,376
1,765 2.39 73,977,376 1,765
2019 52 73,661,476 1,825 2.48 73,661,476 1,825
2020 51 72,609,649 1,818 2.50 73,982,567 1,850
2021 50 70,413,403 1,852 2.63 73,356,806 1,930
2022
51
71,631,732 1,955 2.73 72,969,166 1,990
Data is from the Child File and Agency File. National fatality rates per 100,000 children are calculated for each year by dividing the number of
child fatalities by the population of reporting states, multiplying the result by 100,000, and displayed as rounded to the hundredth.
If fewer than 52 states reported data, the national estimate of child fatalities is calculated by multiplying the national fatality rate (displayed as
rounded) by the child population of all 52 states and dividing by 100,000. e estimate is rounded to the nearest 10. If 52 states reported data, the
actual number of child fatalities reported by states is displayed.
16
North Carolina, Ohio, and Washington.
17
Texas

chApter 4: Fatalities 54
Child Maltreatment 2022
Boys have a higher child fatality rate than girls at 3.26 per 100,000 boys in the population,
compared with 2.25 per 100,000 girls in the population. Boys are 60.3 percent of child fatali-
ties and girls are 39.7 percent. There are not any child fatalities with an unknown sex for FFY
2022. See exhibit 4–C and related notes.
More than 85.0 percent (85.6%) of child fatalities are one of three races: White (36.7%),
Black or African-American (34.9%), or Hispanic (13.9%). Using the number of victims and
the population data to create rates highlights some racial disparity. The rate of Black or
African-American child fatalities (6.37 per 100,000 Black or African-American children) is
3.2 (rounded) times greater than the rate of White child fatalities (1.99 per 100,000 White
children) and 3.8 (rounded) times greater than the rate of Hispanic child fatalities (1.68 per
100,000 Hispanic children). Children of two or more races had the second highest rate at
4.03 and American Indian or Alaska Native children had a rate of 3.37 per 100,000 children.
See exhibit 4–D and related notes.
Exhibit 4–C Child Fatalities by Sex, 2022
Sex Child Population Child Fatalities Child Fatalities Percent
Child Fatalities Rate per
100,000 Children
Boys 29,761,383 971 60.3 3.26
Girls 28,409,359 638 39.7 2.25
Unknown - - - -
National 58,170,742 1,609 100.0 N/A
Based on data from 46 states. Data is from the Child File. No fatalities are reported with an unknown sex. Dashes are inserted into cells without any
data included in this analysis.
Exhibit 4–B Child Fatalities by Age, 2022
Children <1 year old died from abuse and neglect at more than three times the rate of children
who were 1 year old.
Based on data from 46 states. See table 4–3.

chApter 4: Fatalities 55
Child Maltreatment 2022
Exhibit 4–E Maltreatment Types
of Child Fatalities, 2022
Maltreatment Type Child Fatalities Maltreatment Types
Maltreatment Types
Percent
Medical Neglect - 133 8.3
Neglect - 1,229 76.4
Other - 8 0.5
Physical Abuse - 677 42.1
Psychological
Maltreatment - 39 2.4
Sexual Abuse - 9 0.6
Sex Trafcking
- - -
Unknown - - -
National 1,609 2,095 N/A
Based on data from 46 states. Data is from the Child File. A child may have suered from more
than one type of maltreatment and therefore, the total number of reported maltreatments exceeds
the number of fatalities, and the total percentage of reported maltreatments exceeds 100.0
percent. e percentages are calculated against the number of child fatalities in the reporting
states. Dashes are inserted into cells without any data included in this analysis.
As discussed in chapter 3, the Child
Maltreatment report includes only
those maltreatment types that have a
disposition of substantiated or
indicated. It is important to note that
while these maltreatment types likely
contributed to the cause of death,
NCANDS does not have a field for
collecting the official cause of death.
Of the children who died, 76.4 percent
suffered neglect and 42.1 percent
suffered physical abuse either exclu-
sively or in combination with another
maltreatment type. See exhibit 4–E
and related notes.
Risk Factors
Risk factors are characteristics of a child or caregiver that may increase the likelihood of
child maltreatment. Risk factors can be difcult to accurately assess and measure, and there-
fore may go undetected among many children and caregivers. Some states are able to report
data on caregiver risk factors for children who died as a result of maltreatment. Caregivers
with these risk factors may not be the perpetrator responsible for the child’s death. Please see
the Risk Factors section in chapter 3 or Appendix B, Glossary, for more information and the
NCANDS denitions of these risk factors.
Twenty-eight states report that 40 (5.1%) child fatalities had a caregiver with a risk factor of
alcohol abuse. Thirty-four states report that 253 (20.8%) child fatalities had a caregiver with a
risk factor of drug abuse. See exhibit 4–F and related notes.
Exhibit 4–D Child Fatalities by Race or Ethnicity, 2022
Race and Ethnicity Child Population Child Fatalities Child Fatalities Percent
Child Fatalities Rate per
100,000 Children
American Indian or Alaska Native 445,159 15 1.0 3.37
Asian 2,505,982 7 0.4 0.28
Black or African-American 8,624,432 549 34.9 6.37
Hispanic 12,947,772 218 13.9 1.68
Native Hawaiian or Other Pacic
Islander
99,878 3 0.2 3.00
Unknown - 100 6.4 N/A
White 28,958,953 577 36.7 1.99
Two or More Races 2,532,090 102 6.5 4.03
National 56,114,266 1,571 100.0 N/A
Based on data from 44 states. Data is from the Child File. Counts associated with specic racial groups (e.g., White) are exclusive and do not include
Hispanic.
States with 30.0 percent or more of victim race or ethnicity reported as unknown or missing are excluded from this analysis. is analysis includes
only those states that have both race and ethnicity population data. Dashes are inserted into cells without any data included in this analysis.
Maltreatment Types

chApter 4: Fatalities 56
Child Maltreatment 2022
Perpetrator Relationship
The FFY 2022 data shows that most perpetrators are caregivers of their victims. More than 80
percent (81.8%) of child fatalities involved one or more parents acting alone, together, or with
other individuals. More than 10 percent (13.2%) of fatalities did not have a known parental
relationship to their perpetrator. Similarly to all victims, the largest categories in the nonparent
group are relative(s) (4.7%) and “other(s)” (3.4%). The NCANDS category of “other(s)” perpetra-
tor relationship includes any relationship that does not map to one of the NCANDS relationship
categories. According to states’ commentary, “other” includes nonrelated adult, nonrelated child,
foster sibling, babysitter, household staff, clergy, and school personnel. Please see Appendix
D for additional information on what states include in this category. Based on data from 43
states, child fatalities with unknown perpetrator relationship data accounted for 4.9 percent.
See table 4–4 and related notes.
Prior CPS Contact
Some children who die from abuse and neglect are already known to CPS agencies. Not
all states that report child fatalities are able to report family preservation or reunication
services. The national percentages are sensitive to which states report data.
In the states reporting both child fatalities and family preservation services, 97 (9.5%) of
the 1,020 Child File fatalities and 52 (15.4%) of the 338 Agency File fatalities had family
preservation services. In the states reporting both fatalities and family reunication services,
52 (4.1%) of the 1,256 Child File fatalities and 15 (4.4%) of the 342 Agency File fatalities
were removed from home and subsequently reunited with their families prior to their death.
See tables 4–5, 4–6, and related notes.
Exhibit and Table Notes
The following pages contain the data tables referenced in chapter 4. Specic information
about state submissions can be found in Appendix D, State Commentary. Additional infor-
mation regarding the exhibits and tables is provided below.
General
During data analyses, thresholds are set to ensure data quality is balanced with the need to
report data from as many states as possible. States may be excluded from an analysis for data
quality issues. Exclusion rules are listed with the relevant table notes below. Not every table
has an exclusion rule or notes.
■ The data for all tables are from the Child File unless otherwise noted.
■ All analyses use a unique count of fatalities (child fatality is counted once).
■ Rates are per 100,000 children in the population.
Exhibit 4–F Child Fatalities with Selected Caregiver Risk Factors, 2022
Caregiver Risk Factor Reporting States
Child Fatalities from
Reporting States
Child Fatalities with a
Caregiver Risk Factor
Child Fatalities with a
Caregiver Risk Factor
Percent
Alcohol Abuse 28 781 40 5.1
Drug Abuse 34 1,217 253 20.8
Data is from the Child File. For each caregiver risk factor, the analysis includes only those states that report at least 2.0 percent of child victims’
caregiver with the risk factor.
If a child is reported both with and without the caregiver risk factor, the child is counted once with the caregiver risk factor.

chApter 4: Fatalities 57
Child Maltreatment 2022
■ Rates are calculated by dividing the relevant reported count (fatalities, by age, by race,
etc.) by the relevant child population count (by age, by race, etc.) and multiplying by
100,000.
■ NCANDS uses the child population estimates that are released annually by the U.S.
Census Bureau. These estimates are in Appendix C, State Characteristics.
■ The row labeled Reporting States displays the count of states that provide data for that
analysis. States that do not have a child maltreatment related death and report a zero are
included in the count of reporting states and the state’s child population is included in
tables with rate calculations.
■ Child fatalities are reported during the FFY in which the death was determined as due to
maltreatment. This may not be the same year in which the child died.
■ National totals and calculations appear in a single row labeled National instead of separate
rows labeled total, rate, or percent.
■ Dashes are inserted into cells without any data.
Table 4–1 Child Fatalities by Submission Type, 2022
■ Data is from the Child File and Agency File.
■ The rates were computed by dividing the number of total child fatalities by the child
population of reporting states and multiplying by 100,000.
Table 4–2 Child Fatalities, 2018–2022
■ Data is from the Child File and Agency File.
Table 4–3 Child Fatalities by Age, 2022
■ There is no population data for unknown age and therefore, no rates.
Table 4–4 Child Fatalities by Relationship to Their Perpetrators, 2022
■ States are excluded from this analysis if more than 20.0 percent of perpetrators are
reported with an unknown or missing relationship.
■ States are excluded from this analysis if more than 15.0 percent of victims are not associ-
ated with at least one perpetrator.
■ In NCANDS, a child victim may have up to three perpetrators. A few states’ systems do
not have the capability of collecting and reporting data for all three perpetrator elds.
More information may be found in Appendix D.
■ The relationship categories listed under nonparent perpetrator include any perpetrator
relationship that was not identied as a parent.
■ The two parents of known sex category includes mother and father, two mothers, and two
fathers.
■ The two parents of known sex with nonparent category includes mother, father, and
nonparent; two mothers and nonparent; and two fathers and nonparent.
■ One or more parents of unknown sex includes up to three parents in any combination
of known and unknown sex. The parent(s) could have acted alone, together, or with a
nonparent.
■ Nonparent perpetrators counted in combination with parents (e.g., mother and
nonparent(s)) are not also counted in the individual categories listed under nonparent.
■ Multiple nonparental perpetrators that are in the same category are counted within that
category. For example, two child daycare providers are counted as child daycare providers.
■ Multiple nonparental perpetrators that are in different categories are counted in more than
one nonparental perpetrator.

chApter 4: Fatalities 58
Child Maltreatment 2022
■ Some states were not able to collect and report on group home and residential facility staff
perpetrators due to system limitations or jurisdictional issues. See also table 5–5.
Table 4–5 Child Fatalities Who Received Family Preservation Services within
the Previous 5 Years, 2022
■ Data is from the Child File and Agency File.
Table 4–6 Child Fatalities Who Were Reunited with Their Families within the
Previous 5 Years, 2022
■ Data is from the Child File and Agency File.

chApter 4: Fatalities 59
Child Maltreatment 2022
Table 4–1 Child Fatalities by Submission Type, 2022
State
Child Fatalities Reported in
the Child File
Child Fatalities Reported in
the Agency File Total Child Fatalities
Child Fatality Rates per
100,000 Children
Alabama
38 0 38 3.42
Alaska
- 8 8 4.53
Arizona
14 - 14 0.88
Arkansas
39 - 39 5.59
California
- 164 164 1.93
Colorado
40 0 40 3.29
Connecticut
15 0 15 2.05
Delaware
6 0 6 2.88
District of Columbia
3 0 3 2.41
Florida
86 - 86 2.00
Georgia
109 5 114 4.54
Hawaii
5 0 5 1.68
Idaho
7 1 8 1.73
Illinois
110 0 110 4.04
Indiana
62 - 62 3.95
Iowa
18 - 18 2.48
Kansas
8 0 8 1.16
Kentucky
12 0 12 1.19
Louisiana
28 1 29 2.73
Maine
3 - 3 1.21
Maryland
68 0 68 5.05
Massachusetts
- - - -
Michigan
57 4 61 2.89
Minnesota
25 0 25 1.93
Mississippi
69 3 72 10.62
Missouri
56 1 57
4.18
Montana
1 0 1 0.43
Nebraska
3 0 3 0.63
Nevada
14 1 15 2.17
New Hampshire
0 2 2 0.79
New Jersey
19 0 19 0.95
New Mexico
16 3 19 4.13
New York
105 - 105 2.63
North Carolina
- 93 93 4.05
North Dakota
6 0 6 3.28
Ohio
111 4 115 4.49
Oklahoma
29 0 29 3.04
Oregon
- 19 19 2.27
Pennsylvania
80 - 80 3.05
Puerto Rico
4 0 4 0.77
Rhode Island
2 - 2 0.98
South Carolina
34 4 38 3.40
South Dakota
13 - 13 5.93
Tennessee
34 0 34 2.21
Texas
175 1 176 2.36
Utah
15 - 15 1.61
Vermont
0 - 0 0.00
Virginia
39 - 39 2.09
Washington
- 31 31 1.88
West Virginia
8 0 8 2.27
Wisconsin
21 - 21 1.69
Wyoming
2 1 3 2.31
National
1,609 346
1,955 2.73
Reporting States
46 37 51 -

chApter 4: Fatalities 60
Child Maltreatment 2022
Table 4–2 Child Fatalities, 2018–2022
State 2018 2019 2020 2021 2022
Alabama 43 34 47 36 38
Alaska 2 1 2 6 8
Arizona 48 33 18 - 14
Arkansas 44 35 30 36 39
California 145 153 150 159 164
Colorado 40 25 24 31 40
Connecticut 8 4 9 14 15
Delaware 4 13 5 7 6
District of Columbia 5 3 4 2 3
Florida 111 114 101 84 86
Georgia 86 68 85 92 114
Hawaii 1 4 0 2 5
Idaho 3 3 10 3 8
Illinois 70 106 102 89 110
Indiana 80 116 56 57 62
Iowa 16 25 9 12 18
Kansas 9 16 10 10 8
Kentucky 6 12 9 11 12
Louisiana 25 24 18 23 29
Maine 3 3 1 8 3
Maryland 40 55 50 84 68
Massachusetts 14
13 - - -
Michigan 49 63 43 35 61
Minnesota 30 17 21 22 25
Mississippi 30 35 38 49 72
Missouri 36 46 44 75 57
Montana 2 2 5 2 1
Nebraska 0 5 2 1 3
Nevada 19 20 14 27 15
New Hampshire 0 2 2 3 2
New Jersey 18 19 17 10 19
New Mexico 12 11 13 10 19
New York 118 69 105 126 105
North Carolina 14 5 99 121 93
North Dakota 8 6 5 4 6
Ohio 106 79 94 98 115
Oklahoma 47 23 42 15 29
Oregon 26 23 17 18 19
Pennsylvania 45 54 67 65 80
Puerto Rico 3 5 5 7 4
Rhode Island 1 3 2 2 2
South Carolina 39 60 36 41 38
South Dakota 3 9 12 9 13
Tennessee 47 43 34
32 34
Texas 200 229 255 206 176
Utah 10 11 6 4 15
Vermont 1 1 0 1 0
Virginia 37 49 39 51 39
Washington 28 25 14 19 31
West Virginia 8 17 12 9 8
Wisconsin 24 34 32 22 21
Wyoming 1 0 3 2 3
National 1,765 1,825 1,818 1,852 1,955
Reporting States 52 52 51 50 51

chApter 4: Fatalities 61
Child Maltreatment 2022
Table 4–4 Child Fatalities by Relationship to Their Perpetrators, 2022
Table 4–3 Child Fatalities by Age, 2022
Age Child Population Child Fatalities Child Fatalities Percent
Child Fatalities Rate per
100,000 Children
<1 2,950,151 719 44.7 24.37
1 2,884,134 206 12.8 7.14
2 2,968,151 138 8.6 4.65
3 3,010,181 98 6.1 3.26
4 3,078,737 89 5.5 2.89
5 3,133,549 51 3.2 1.63
6 3,218,278 34 2.1 1.06
7 3,244,883 23 1.4 0.71
8 3,235,278 30 1.9 0.93
9 3,223,002 20 1.2 0.62
10 3,229,046 30 1.9 0.93
11 3,262,705 19 1.2 0.58
12 3,334,666 33 2.1 0.99
13 3,407,838 29 1.8 0.85
14 3,535,093 30 1.9 0.85
15 3,531,250 18 1.1 0.51
16 3,476,081 15 0.9 0.43
17 3,447,719 23 1.4 0.67
Unborn, Unknown,
and 18–21 - 4 0.2 N/A
National 58,170,742 1,609 100.0 N/A
Based on data from 46 states.
Perpetrator
Child Fatalities
by Reported Relationships Reported Relationships Percent
PARENT - -
Father Only 226 14.5
Father and Nonparent 21 1.3
Mother Only 473 30.2
Mother and Nonparent 161 10.3
Two Parents of Known Sex 363 23.2
Three Parents of Known Sex 2 0.1
Two Parents of Known Sex and
Nonparent 26 1.7
One or More Parents of Unknown Sex 8 0.5
Total Parents 1,280 81.8
NONPARENT
- -
Child Daycare Provider(s) 21 1.3
Foster Parent(s) 6 0.4
Friend(s) or Neighbor(s) 4 0.3
Group Home and Residential Facility Staff 4 0.3
Legal Guardian(s) 7 0.4
Other Professional(s) 2 0.1
Relative(s) 73 4.7
Unmarried Partner(s) of Parent 17 1.1
Other(s) 53 3.4
More Than One Nonparental Perpetrator
20
1.3
Total Nonparents 207 13.2
UNKNOWN 77 4.9
National 1,564 100.0
Based on data from 43 states.
chApter 4: Fatalities 62
Child Maltreatment 2022
Table 4–5 Child Fatalities Who Received Family Preservation
Services within the Previous 5 Years, 2022
State Child File Fatalities
Child File Fatalities Whose Families
Received Preservation Services in
the Previous 5 Years Agency File Fatalities
Agency File Fatalities Whose
Families Received Preservation
Services in the Previous 5 Years
Alabama 38 5 0 0
Alaska - - 8 2
Arizona - - - -
Arkansas 39 6 - -
California - - 164 23
Colorado - - - -
Connecticut 15 0 0 0
Delaware - - - -
District of Columbia 3 0 0 0
Florida 86 8 - -
Georgia 109 10 5 2
Hawaii - - - -
Idaho 7 0 1 1
Illinois 110 9 0 0
Indiana - - - -
Iowa - - - -
Kansas 8 2 0 0
Kentucky 12 2 0 0
Louisiana 28 4 1 0
Maine - - - -
Maryland - - - -
Massachusetts - - - -
Michigan - - - -
Minnesota 25 9 0 0
Mississippi 69 2 3 0
Missouri 56 4 1
0
Montana - - - -
Nebraska 3 0 0 0
Nevada 14 1 1 0
New Hampshire 0 0 2 0
New Jersey 19 1 0 0
New Mexico 16 0 3 0
New York - - - -
North Carolina - - 93 10
North Dakota 6 2 0 0
Ohio 111 0 4 0
Oklahoma 29 1 0 0
Oregon - - 19 9
Pennsylvania - - - -
Puerto Rico 4 0 0 0
Rhode Island 2 2 - -
South Carolina - - - -
South Dakota - - - -
Tennessee 34 7 0 0
Texas 175 21 1 0
Utah - - - -
Vermont 0 0 - -
Virginia - - - -
Washington - - 31 5
West Virginia - - - -
Wisconsin - - - -
Wyoming 2 1 1
0
National 1,020 97
338 52
National Percent - 9.5 - 15.4
Reporting States 28 28 29 29

chApter 4: Fatalities 63
Child Maltreatment 2022
Table 4–6 Child Fatalities Who Were Reunited with Their Families
within the Previous 5 Years, 2022
State Child File Fatalities
Child File Fatalities Who Were
Reunited with Their Families in the
Previous 5 Years Agency File Fatalities
Agency File Fatalities Who Were
Reunited with Their Families in the
Previous 5 Years
Alabama 38 0 0 0
Alaska - - 8 2
Arizona - - - -
Arkansas 39 0 - -
California - - 164 10
Colorado 40 3 - -
Connecticut 15 0 0 0
Delaware 6 1 0 0
District of Columbia 3 0 0 0
Florida 86 3 - -
Georgia 109 4 5 0
Hawaii 5 0 0 0
Idaho 7 0 1 0
Illinois 110 4 0 0
Indiana 62 7 - -
Iowa - - - -
Kansas 8 1 0 0
Kentucky 12 1 0 0
Louisiana 28 0 1 0
Maine - - - -
Maryland 68 9 - -
Massachusetts - - - -
Michigan - - - -
Minnesota 25 1 0 0
Mississippi 69 0 3 0
Missouri 56 1 1
0
Montana - - - -
Nebraska 3 0 0 0
Nevada 14 1 1 0
New Hampshire 0 0 2 0
New Jersey 19 0 0 0
New Mexico 16 0 3 0
New York - - - -
North Carolina - - 93 1
North Dakota 6 0 0 0
Ohio 111 4 4 0
Oklahoma 29 1 0 0
Oregon - - 19 0
Pennsylvania - - - -
Puerto Rico 4 0 0 0
Rhode Island 2 0 - -
South Carolina 34 0 4 0
South Dakota - - - -
Tennessee 34 2 0 0
Texas 175 8 1 0
Utah - - - -
Vermont 0 0 - -
Virginia - - - -
Washington - - 31 2
West Virginia - - - -
Wisconsin 21 0 - -
Wyoming 2 1 1
0
National 1,256 52
342 15
National Percent - 4.1 - 4.4
Reporting States 35 35 32 32

chApter 5: Perpetrators 64
Child Maltreatment 2022
Perpetrators
NCANDS denes a perpetrator as a person who is determined to have caused or knowingly
allowed the maltreatment of a child. NCANDS does not collect information about persons who
are alleged to be perpetrators and not found to have perpetrated abuse and neglect. This chapter
includes perpetrators of children with substantiated and indicated dispositions (see chapter 3 for
denitions). The majority of perpetrators are caregivers of their victims.
One state recoded the disposition of children who would have previously received an alternative
response victim disposition to an indicated disposition and submitted or resubmitted les for
FFYs 2018–2022. Children with alternative response dispositions are not considered maltreat-
ment victims and do not have perpetrators. Children with indicated dispositions are considered
maltreatment victims. The state was not able to include perpetrators for indicated dispositions
in its FFY 2018–2022 data submissions and is excluded from the majority of this chapter.
18
Number of Perpetrators (unique count of perpetrators)
The analyses in this chapter use a unique count of perpetrators, which means identifying and
counting a perpetrator once, regardless of the number of times the perpetrator is the subject
of a report. For FFY 2022, 52 states reported a unique count of 434,090 perpetrators. This is
a 20.6 percent decrease from FFY 2018 when 52 states reported 546,836 unique perpetrators.
See table 5–1 and related notes.
Perpetrator Demographics (unique count of perpetrators)
The majority (68.8%) of perpetrators are in the age range of 25–44 years old. Perpetrators in
the age group 25–34 are 39.9 percent of all perpetrators. Perpetrators younger than 18 years
old accounted for 1.9 percent of all perpetrators. Some states have laws that limit the youngest
age that a person can be considered a perpetrator. (See Appendix D, State Commentary.) The
perpetrator age group of 25–34 have the highest rate at 3.9 per 1,000 adults in the population of
the same age. Older adults in the age group of 35–44 have the second highest rate at 2.9, while
young adults in the age group of 18–24 have a rate of 1.9 per 1,000 adults in the population of
the same age.
19
See table 5–2, exhibit 5–A, and related notes.
Based on data from 50 reporting states, slightly more than one-half (51.1%) of perpetrators are
female and 47.7 percent of perpetrators are male; 1.1 percent of perpetrators are of unknown
sex. See table 5–3 and related notes. The three largest percentages of perpetrators are White
(47.4%), Black or African-American (21.0%), and Hispanic (20.3%). Race or ethnicity is
CHAPTER 5
18
North Carolina
19
Rates are not calculated for perpetrators younger than 18 years due to the variations in state policy as to how young a
perpetrator can be.

Child Maltreatment 2022
chApter 5: Perpetrators 65
unknown or not reported for 6.1
percent of perpetrators. See table 5–4,
exhibit 5–B, and related notes.
Perpetrator Relationship
(unique count of perpetrators and unique
count of relationships)
In this analysis, single relationships
are counted only once per category.
Perpetrators with two or more rela-
tionships are counted in the multiple
relationships category. In the scenarios
below, the perpetrator is counted once in
the parent category:
■ The perpetrator is a parent to one
victim and in two or more reports
(one victim is reported at
least twice).
■ The perpetrator is a parent
to two victims and in one
report.
In the following scenarios, the
perpetrator is counted once
in the multiple relationships
category:
■ The perpetrator is a
parent to one victim and
is an unmarried partner of
parent to a second victim
in the same report.
■ The perpetrator is a parent
to one victim in one report
and an unmarried partner of parent to a second victim in a second report.
The majority (76.0%) of perpetrators are a parent of their victim, 7.0 percent of perpetrators
are a relative other than a parent, 4.2 percent are an unmarried partner of the parent, and 4.1
percent have multiple relationships to their victims. Nearly 4.0 percent (3.9%) of perpetrators
have an “other” relationship to their victims. See table 5–5 and related notes. According to
Appendix D, State Commentary, the NCANDS category of “other” perpetrator relationship
includes foster sibling, nonrelative, babysitter, etc.
Exhibit 5–B Perpetrators by Race or Ethnicity, 2022
The largest percentages of perpetrators are White,
Black or African-American, and Hispanic
Based on data from 48 states. See table 5–4.
Exhibit 5–A Perpetrators by Age, 2022
Perpetrators ages 25 through 44 have the highest rates per 1,000
Based on data from 50 states. See table 5–2.

chApter 5: Perpetrators 66
Child Maltreatment 2022
Exhibit and Table Notes
The following pages contain the data tables referenced in chapter 5. Specic information
about state submissions can be found in Appendix D, State Commentary. Additional informa-
tion regarding the exhibits and tables is provided below.
General
During data analyses, thresholds are set to ensure data quality is balanced with the need to
report data from as many states as possible. States may be excluded from an analysis for
data quality issues. Exclusion rules are listed in the table notes below. Not every table has an
exclusion rule or notes.
■ The data for all tables are from the Child File.
■ Rates are per 1,000 adults in the population.
■ Rates are calculated by dividing the perpetrator count by the adult population count and
multiplying by 1,000.
■ NCANDS uses the population estimates that are released annually by the U.S. Census
Bureau. These estimates are available in Appendix C, State Characteristics.
■ National totals and calculations appear in a single row labeled National instead of separate
rows labeled total, rate, or percent.
■ The row labeled Reporting States displays the count of states that provided data for that
analysis.
■ Unless otherwise noted, all tables use a unique count of perpetrators.
■ Dashes are inserted into cells without any data.
Table 5–2 Perpetrators by Age, 2022
■ In NCANDS, valid perpetrator ages are 6–75 years old. If a perpetrator is reported with an
age of 76 years or older, the age is recoded to 75.
■ Some states have laws restricting how young a perpetrator can be. More information may be
found in appendix D.
■ Rates are not calculated for perpetrators younger than 18 years.
■ If a perpetrator appears in two or more reports, the age at the time of the earliest report is
used.
■ States are excluded from this analysis if fewer than 85.0 percent of victims are associated
with one or more perpetrators.
■ States are excluded from this analysis if there are known data quality issues with reporting
age.
Table 5–3 Perpetrators by Sex, 2022
■ The category of unknown sex includes not reported.
■ States are excluded from this analysis if fewer than 85.0 percent of victims are associated
with one or more perpetrators.
■ States are excluded if more than 15.0 percent of perpetrators are reported with an unknown or
missing sex.
Table 5–4 Perpetrators by Race or Ethnicity, 2022
■ Counts associated with each racial group are exclusive and do not include Hispanic ethnicity.
■ Perpetrators reported with Hispanic ethnicity are counted as Hispanic, regardless of any
reported race.
■ States are excluded from this analysis if more than 30.0 percent of perpetrators have an
unknown or missing race or ethnicity.

Child Maltreatment 2022
chApter 5: Perpetrators 67
■ Only those states that reported both race and ethnicity separately are included in this
analysis.
■ States are excluded from this analysis if fewer than 85.0 percent of victims are associated
with one or more perpetrators.
Table 5–5 Perpetrators by Relationship to Their Victims, 2022
■ Some states are not able to collect and report on group home and residential facility staff
perpetrators due to system limitations or jurisdictional issues. More information may be
found in appendix D.
■ States are excluded from this analysis if more than 25.0 percent of perpetrators are reported
with an unknown or missing relationship.
■ States are excluded from this analysis if fewer than 85.0 percent of victims are associated
with one or more perpetrators.

Child Maltreatment 2022
chApter 5: Perpetrators 68
Table 5–1 Perpetrators, 2018–2022
State 2018 2019 2020 2021 2022
Alabama 8,791 8,376 8,432 8,387 8,162
Alaska 2,032 2,294 2,425 2,023 1,964
Arizona 15,395 12,909 9,684 - 12,151
Arkansas 7,424 7,118 7,809 8,138 7,635
California 58,362 55,845 53,124 49,073 45,289
Colorado 10,253 10,478 9,820 9,416 8,080
Connecticut 6,292 6,497 5,171 4,541 4,090
Delaware 976 977 919 896 829
District of Columbia 1,136 1,257 1,054 1,059 1,016
Florida 27,844 24,927 21,599 20,933 18,647
Georgia 8,612 8,107 6,730 7,344 7,897
Hawaii 1,098 1,158 1,150 1,220 1,144
Idaho 1,774 1,774 1,764 2,016 1,702
Illinois 22,275 23,858 25,303 25,475 23,359
Indiana 20,159 18,477 18,036 17,185 15,302
Iowa 8,529 8,327 7,625 8,158 8,003
Kansas 2,594 2,473 1,998 1,786 1,551
Kentucky 17,400 14,731 12,443 11,303 9,399
Louisiana 7,983 7,574 6,091 5,659 6,565
Maine 3,021 3,874 4,030 3,693 3,258
Maryland 6,507 6,559 6,424 5,715 5,967
Massachusetts 20,750
20,075 17,947 18,261 17,811
Michigan 30,705 26,210 21,484 19,348 18,417
Minnesota 5,617 4,951 4,709 4,000 3,768
Mississippi 8,252 7,793 6,812 7,107 7,611
Missouri 5,108 4,252 4,015 3,945 3,625
Montana 2,704 2,686 2,630 2,142 1,870
Nebraska 1,859 2,022 1,648 1,684 1,338
Nevada 4,120 4,000 4,094 4,465 4,643
New Hampshire 1,154 1,112 1,008 875 913
New Jersey 4,589 4,026 2,826 2,517 2,434
New Mexico 6,832 6,702 5,852 4,848 4,668
New York 54,550 52,669 45,922 43,478 38,597
North Carolina 3,995 3,718 3,891 3,635 3,752
North Dakota 1,558 1,344 1,200 1,037 852
Ohio 20,567 21,190 19,599 19,772 18,424
Oklahoma 12,929 12,901 12,487 11,595 11,332
Oregon 9,486 10,056 8,541 7,964 7,969
Pennsylvania 4,865 4,941 4,615 4,765 5,040
Puerto Rico 3,347 3,666 2,734 3,786 3,472
Rhode Island 2,846 2,508 2,141 2,023 1,948
South Carolina 14,350 13,630 10,727 11,503 10,930
South Dakota 933 1,099 1,097 992 1,028
Tennessee 9,116 9,428 8,493
7,608 6,828
Texas 49,563 49,969 50,567 50,820 42,240
Utah 7,784 7,851 7,197 6,676 6,387
Vermont 782 709 419 308 556
Virginia 5,074 5,005 4,728 4,180 3,882
Washington 3,881 3,693 3,315 3,036 2,986
West Virginia 6,252 5,959 5,359 5,475 4,821
Wisconsin 4,031 3,668 3,345 3,431 3,325
Wyoming 780 849 729 652 613
National 546,836 526,272 481,762 455,948 434,090
Reporting States 52 52 52 51 52

Child Maltreatment 2022
chApter 5: Perpetrators 69
Table 5–2 Perpetrators by Age, 2022 (continues next page)
State 6 –11 12–17 18–24 25–34 35–44 45–54 55–64 65 –74 75 and Older Unknown
Total Unique
Perpetrators
Alabama - 269 1,467 3,196 1,861 535 234 79 18 503 8,162
Alaska - 5 232 784 587 196 91 26 3 40 1,964
Arizona - 60 1,756 5,119 3,465 966 310 99 24 352 12,151
Arkansas 116 368 1,545 2,839 1,632 468 236 73 24 334 7,635
California 43 445 5,229 18,421 13,887 4,445 1,518 461 166 674 45,289
Colorado 23 200 1,017 3,248 2,424 712 221 69 56 110 8,080
Connecticut 2 10 437 1,561 1,338 458 158 41 13 72 4,090
Delaware 2 22 87 343 245 66 36 24 4 - 829
District of Columbia - 4 117 476 284 72 23 6 0 34 1,016
Florida - 57 1,980 7,587 5,869 1,716 645 250 79 464 18,647
Georgia
1
72 976 3,434 2,352 677 267 95 19 4 7,897
Hawaii - 3 99 389 398 153 55 18 5 24 1,144
Idaho - 14 294 683 497 151 50 11 2 - 1,702
Illinois 24 410 3,424 9,924 6,422 1,945 666 207 45 292 23,359
Indiana 12 379 3,026 6,507 3,651 1,061 379 116 40 131 15,302
Iowa - 138 1,237 3,285 2,389 620 233 74 18 9 8,003
Kansas 4 105 197 547 461 134 58 18 8 19 1,551
Kentucky 1 51 1,240 3,903 2,750 876 390 134 53 1 9,399
Louisiana 2 52 1,217 2,903 1,744 400 174 54 14 5 6,565
Maine - 5 315 1,311 1,165 304 106 27 5 20 3,258
Maryland - - - - - - - - - - -
Massachusetts - 64
1,638
6,443 6,025 2,208 687 202 48 496 17,811
Michigan 2 54 2,256 8,005 5,727 1,659 532 129 35 18 18,417
Minnesota 18 149 452 1,433 1,226 324 121 38 7 - 3,768
Mississippi 68 274 1,099 2,800 2,195 670 316 136 28 25 7,611
Missouri - 31 470 1,285 1,032 375 186 67 20 159 3,625
Montana - 8 217 743 635 175 53 18 2 19 1,870
Nebraska - 28 196 541 397 129 35 9 2 1 1,338
Nevada - 17 557 2,082 1,418 390 138 31 10 - 4,643
New Hampshire - 9 84 360 318 84 38 9 2 9 913
New Jersey - 3 180 903 867 271 122 36 13 39 2,434
New Mexico 2 18 433 1,820 1,391 379 126 45 9 445 4,668
New York 4 108 3,952 14,605
12,847
4,874 1,673 440 86 8 38,597
North Carolina - - - - - - - - - - -
North Dakota - 3 108 382 255 47 10 4 0 43 852
Ohio 46 853 2,713 6,762 4,580 1,444 600 212 48 1,166 18,424
Oklahoma 1 58 1,652 4,656 3,255 992 374 114 26 204 11,332
Oregon 1 176 939 3,049 2,465 739 245 83 41 231 7,969
Pennsylvania - 197 760 1,660 1,340 555 261 121 27 119 5,040
Puerto Rico 4 23 462 1,372 1,032 350 156 49 18 6 3,472
Rhode Island - 30 264 840 566 173 46 12 2 15 1,948
South Carolina 19 39 1,249 4,528 3,462 1,057 359 147 34 36 10,930
South Dakota - 10 142 465 292 74 28 2 2 13 1,028
Tennessee 12 384 997 2,254 1,303 488
253
88 34 1,015 6,828
Texas 168 1,714 8,312 17,848 9,824 2,688 1,135 406 112 33 42,240
Utah 18 565 819 2,078 2,007 624 193 61 19 3 6,387
Vermont - 39 82 167 154 45 28 10 1 30 556
Virginia - 36 455 1,485 1,081 370 156 70 24 205 3,882
Washington - 2 294 1,182 1,051 311 89 21 8 28 2,986
West Virginia 4 14 501 1,863 1,353 415 175 77 9 410 4,821
Wisconsin 3 24 405 1,137 808 241 94 24 9 580 3,325
Wyoming 1 7 64 263 206 42 11 6 1 12 613
National 601 7,606 57,644 169,471 122,533 38,148 14,090 4,549 1,273 8,456 424,371
Reporting States 27 50 50 50 50 50 50 50 50 46 50
Child Maltreatment 2022
chApter 5: Perpetrators 70
Table 5–2 Perpetrators by Age, 2022
State
18–24 Rate
per 1,000
Adults
25–34 Rate
per 1,000
Adults
35–44 Rate
per 1,000
Adults
45–54 Rate
per 1,000
Adults
55–64 Rate
per 1,000
Adults
65–74 Rate
per 1,000
Adults
75 and Older
Rate per
1,000 Adults
Alabama 3.0 4.9 3.0 0.9 0.4 0.1 0.0
Alaska 3.4 6.9 5.7 2.4 1.0 0.4 0.1
Arizona 2.4 5.0 3.7 1.1 0.4 0.1 0.0
Arkansas 5.3 7.1 4.3 1.3 0.6 0.2 0.1
California 1.4 3.2 2.6 0.9 0.3 0.1 0.1
Colorado 1.8 3.5 2.9 1.0 0.3 0.1 0.2
Connecticut 1.2 3.4 2.9 1.0 0.3 0.1 0.0
Delaware 1.0 2.7 2.0 0.6 0.3 0.2 0.0
District of Columbia 1.7 3.3 2.6 1.0 0.4 0.1 0.0
Florida 1.1 2.7 2.1 0.6 0.2 0.1 0.0
Georgia 0.9 2.3 1.6 0.5 0.2 0.1 0.0
Hawaii 0.8 2.0 2.1 0.9 0.3 0.1 0.0
Idaho 1.5 2.7 2.0 0.7 0.2 0.1 0.0
Illinois 2.9 5.8 3.9 1.2 0.4 0.2 0.0
Indiana 4.5 7.3 4.2 1.3 0.4 0.2 0.1
Iowa 3.8 8.2 5.9 1.7 0.6
0.2 0.1
Kansas 0.6 1.5 1.2 0.4 0.2 0.1 0.0
Kentucky 3.0 6.6 4.9 1.6 0.7 0.3 0.2
Louisiana 2.8 4.8 2.9 0.8 0.3 0.1 0.0
Maine 2.9 7.8 6.9 1.8 0.5 0.1 0.0
Maryland - - - - - - -
Massachusetts 2.3 6.6 6.7 2.6 0.7 0.3 0.1
Michigan 2.4 6.1 4.7 1.4 0.4 0.1 0.0
Minnesota 0.9 1.9 1.6 0.5 0.2 0.1 0.0
Mississippi 3.8 7.4 6.0 1.9 0.9 0.4 0.1
Missouri 0.8 1.6 1.3 0.5 0.2 0.1 0.0
Montana 2.1 5.1 4.4 1.4 0.4 0.1 0.0
Nebraska 1.0 2.1 1.5 0.6 0.1 0.0 0.0
Nevada 2.1 4.5 3.2 1.0 0.4 0.1 0.0
New Hampshire 0.7 2.0 1.8 0.5 0.2 0.1 0.0
New Jersey 0.2 0.8 0.7 0.2 0.1
0.0 0.0
New Mexico 2.1 6.5 5.2 1.6 0.5 0.2 0.1
New York 2.2 5.3 5.1
2.0 0.6 0.2 0.1
North Carolina - - - - - - -
North Dakota 1.2 3.5 2.5 0.6 0.1 0.1 0.0
Ohio 2.5 4.4 3.1 1.0 0.4 0.2 0.1
Oklahoma 4.1 8.6 6.2 2.2 0.8 0.3 0.1
Oregon 2.5 5.1 4.2 1.4 0.5 0.2 0.1
Pennsylvania 0.6 1.0 0.8 0.4 0.1 0.1 0.0
Puerto Rico 1.6 3.2 2.7 0.9 0.4 0.1 0.0
Rhode Island 2.4 5.5 4.1 1.3 0.3 0.1 0.0
South Carolina 2.5 6.7 5.3 1.7 0.5 0.2 0.1
South Dakota 1.6 4.1 2.6 0.8 0.2 0.0 0.0
Tennessee 1.5 2.3 1.5 0.6 0.3 0.1 0.1
Texas 2.7 4.1 2.3 0.7 0.3 0.2 0.1
Utah 2.0 4.2 4.3 1.7 0.6 0.2 0.1
Vermont 1.2 2.2 1.9 0.6 0.3 0.1 0.0
Virginia 0.6 1.3 0.9
0.3 0.1 0.1 0.0
Washington 0.4 1.0 0.9 0.3 0.1 0.0 0.0
West Virginia 3.1
8.7 6.4 1.9 0.7 0.3 0.1
Wisconsin 0.7 1.6 1.1 0.3 0.1 0.0 0.0
Wyoming 1.2 3.6 2.7 0.6 0.2 0.1 0.0
National 1.9 3.9 2.9 1.0 0.3 0.1 0.1
Reporting States - - - - - - -

chApter 5: Perpetrators 71
Child Maltreatment 2022
Table 5–3 Perpetrators by Sex, 2022
State Men Women Unknown Total Perpetrators Men Percent Women Percent Unknown Percent
Alabama 3,499 4,639 24 8,162 42.9 56.8 0.3
Alaska 893 1,048 23 1,964 45.5 53.4 1.2
Arizona - - - - - - -
Arkansas 3,418 4,058 159 7,635 44.8 53.1 2.1
California 20,619 24,307 363 45,289 45.5 53.7 0.8
Colorado 4,340 3,697 43 8,080 53.7 45.8 0.5
Connecticut 2,054 1,997 39 4,090 50.2 48.8 1.0
Delaware 518 311 - 829 62.5 37.5 -
District of Columbia 326 674 16 1,016 32.1 66.3 1.6
Florida 8,866 9,445 336 18,647 47.5 50.7 1.8
Georgia 2,795 5,085 17 7,897 35.4 64.4 0.2
Hawaii 520 609 15 1,144 45.5 53.2 1.3
Idaho 704 997 1 1,702 41.4 58.6 0.1
Illinois 10,998 12,177 184 23,359 47.1 52.1 0.8
Indiana 6,583 8,679 40 15,302 43.0 56.7 0.3
Iowa 3,725 4,262 16 8,003 46.5
53.3 0.2
Kansas 883 660 8 1,551 56.9 42.6 0.5
Kentucky 4,396 4,970 33 9,399 46.8 52.9 0.4
Louisiana 2,051 4,484 30 6,565 31.2 68.3 0.5
Maine 1,654 1,602 2 3,258 50.8 49.2 0.1
Maryland 3,227 2,514 226 5,967 54.1 42.1 3.8
Massachusetts 8,023 9,051 737 17,811 45.0 50.8 4.1
Michigan 9,150 9,234 33 18,417 49.7 50.1 0.2
Minnesota 2,037 1,731 - 3,768 54.1 45.9 -
Mississippi 3,225 4,307 79 7,611 42.4 56.6 1.0
Missouri 2,163 1,329 133 3,625 59.7 36.7 3.7
Montana 860 980 30 1,870 46.0 52.4 1.6
Nebraska 696 642 - 1,338 52.0 48.0 -
Nevada 2,203 2,439 1 4,643 47.4 52.5 0.0
New Hampshire 449 458 6 913 49.2 50.2 0.7
New Jersey 1,221 1,209 4 2,434 50.2 49.7 0.2
New Mexico 1,984 2,573 111 4,668 42.5 55.1 2.4
New York 19,115 19,478 4
38,597 49.5 50.5 0.0
North Carolina - - - - - - -
North Dakota 272 557 23 852 31.9 65.4 2.7
Ohio 9,048 8,993 383 18,424 49.1 48.8 2.1
Oklahoma 5,618 5,669 45 11,332 49.6 50.0 0.4
Oregon 4,667 3,164 138 7,969 58.6 39.7 1.7
Pennsylvania 3,354 1,605 81 5,040 66.5 31.8 1.6
Puerto Rico 1,336 2,136 - 3,472 38.5 61.5 -
Rhode Island 998 945 5 1,948 51.2 48.5 0.3
South Carolina 4,300 6,624 6 10,930 39.3 60.6 0.1
South Dakota 373 646 9 1,028 36.3 62.8 0.9
Tennessee 3,524 2,844 460 6,828 51.6 41.7 6.7
Texas 21,545 20,440 255 42,240 51.0 48.4 0.6
Utah 3,752 2,597 38 6,387 58.7 40.7 0.6
Vermont 383 173 - 556 68.9 31.1 -
Virginia 1,836 1,970 76 3,882 47.3 50.7 2.0
Washington 1,504 1,473 9 2,986 50.4 49.3 0.3
West Virginia 2,057
2,761 3 4,821 42.7 57.3 0.1
Wisconsin 1,586 1,289 450 3,325 47.7 38.8 13.5
Wyoming 269 344 - 613 43.9 56.1 -
National 199,617 213,876 4,694 418,187 47.7 51.1 1.1
Reporting States 50 50 44 50 - - -

chApter 5: Perpetrators 72
Child Maltreatment 2022
Table 5–4 Perpetrators by Race or Ethnicity, 2022 (continues next page)
State
American
Indian or
Alaska Native Asian
Black or
African-
American Hispanic
Two or More
Races
Native
Hawaiian or
Other Pacic
Islander White Unknown
Total
Perpetrators
Alabama 6 16 2,248 307 48 6 5,303 228 8,162
Alaska 1,025 14 60 6 88 42 526 203 1,964
Arizona 568 48 1,195 39 297 34 6,639 3,331 12,151
Arkansas 7 17 1,522 516 391 38 4,856 288 7,635
California 447 1,302 6,215 21,564 0 146 11,653 3,962 45,289
Colorado - - - - - - - - -
Connecticut 5 34 978 1,234 71 3 1,604 161 4,090
Delaware 0 3 375 127 2 0 322 - 829
District of Columbia 0 1 728 90 2 0 11 184 1,016
Florida 24 100 5,216 2,738 205 17 9,108 1,239 18,647
Georgia 7 24 3,112 516 74 6 3,849 309 7,897
Hawaii 6 122 22 49
294 310 252 89 1,144
Idaho 35 3 19
175 21 2 1,061 386 1,702
Illinois 11 269 7,164 3,812 215 7 11,447 434 23,359
Indiana 6 64 2,882 1,018 352 17 10,793 170 15,302
Iowa 112 54 1,132 632 87 42 5,855 89 8,003
Kansas 14 13 186 189 28 3 1,013 105 1,551
Kentucky 5 19 881 268 242 5 7,795 184 9,399
Louisiana 20 12 2,984 162 29 3 3,053 302 6,565
Maine 41 12 85 84 76 5 2,484 471 3,258
Maryland - - - - - - - - -
Massachusetts 26 298 2,450 4,760 396 19 7,613 2,249 17,811
Michigan 92 83 5,735 1,184 893 9 10,350 71 18,417
Minnesota 289 112 591 456 398 3 1,824 95 3,768
Mississippi 16 11 2,722 159 31 3 3,813 856
7,611
Missouri 11 7 442 230 12 7 2,605
311 3,625
Montana 311 2 17 66 42 3 1,042 387 1,870
Nebraska 81 11 175 200 50 1 689 131 1,338
Nevada 23 75 1,275 1,152 103 65 1,576 374 4,643
New Hampshire 2 5 17 39 14 1 743 92 913
New Jersey 6 30 654 731 18 2 899 94 2,434
New Mexico 434 10 125 2,382 54 3 1,020 640 4,668
New York 153 1,128 11,127 10,176 677 21 14,935 380 38,597
North Carolina - - - - - - - - -
North Dakota 189 2 61 29 21 4 459 87 852
Ohio 15 50 4,638 759 539 14 11,174 1,235 18,424
Oklahoma 590 43 1,206 1,623 2,486 26 5,237 121 11,332
Oregon 172 52 331 852 145 35 4,826 1,556 7,969
Pennsylvania 7 42
1,102 655 65 1 2,747 421 5,040
Puerto Rico 5
0 33 3,173 3 0 88 170 3,472
Rhode Island 14 25 299 512 52 1 983 62 1,948
South Carolina 17 20 4,105 580 97 8 5,302 801 10,930
South Dakota 440 1 25 65 90 2 372 33 1,028
Tennessee - - - - - - - - -
Texas 80 321 9,571 17,326 398 64 13,042 1,438 42,240
Utah 135 55 217 1,359 81 137 4,346 57 6,387
Vermont 0 6 23 6 0 0 465 56 556
Virginia 2 25 893 443 30 7 2,148 334 3,882
Washington 126 44 223 497 154 65 1,628 249 2,986
West Virginia 0 2 174 37 97 2 4,457 52 4,821
Wisconsin 127 44 578 273 51 1 1,673 578 3,325
Wyoming 21 2 13 64 0 2
484 27 613
National 5,723 4,633 85,826 83,314 9,519
1,192 194,164 25,092 409,463
Reporting States 48 48 48 48 48 48 48 47 48
Child Maltreatment 2022
chApter 5: Perpetrators 73
Table 5–4 Perpetrators by Race or Ethnicity, 2022
State
American
Indian or
Alaska Native
Percent Asian Percent
Black or
African-
American
Percent
Hispanic
Percent
Two or More
Races Percent
Native
Hawaiian or
Other Pacic
Islander
Percent
White
Percent
Unknown
Percent
Alabama 0.1 0.2 27.5 3.8 0.6 0.1 65.0 2.8
Alaska 52.2 0.7 3.1 0.3 4.5 2.1 26.8 10.3
Arizona 4.7 0.4 9.8 0.3 2.4 0.3 54.6 27.4
Arkansas 0.1 0.2 19.9 6.8 5.1 0.5 63.6 3.8
California 1.0 2.9 13.7 47.6 0.0 0.3 25.7 8.7
Colorado - - - - - - - -
Connecticut 0.1 0.8 23.9 30.2 1.7 0.1 39.2 3.9
Delaware 0.0 0.4 45.2 15.3 0.2 0.0 38.8 -
District of Columbia 0.0 0.1 71.7 8.9 0.2 0.0 1.1 18.1
Florida 0.1 0.5 28.0 14.7 1.1 0.1 48.8 6.6
Georgia 0.1 0.3 39.4 6.5 0.9 0.1 48.7 3.9
Hawaii 0.5 10.7 1.9 4.3 25.7 27.1 22.0 7.8
Idaho 2.1 0.2
1.1 10.3 1.2 0.1 62.3 22.7
Illinois 0.0 1.2 30.7 16.3 0.9 0.0 49.0
1.9
Indiana 0.0 0.4 18.8 6.7 2.3 0.1 70.5 1.1
Iowa 1.4 0.7 14.1 7.9 1.1 0.5 73.2 1.1
Kansas 0.9 0.8 12.0 12.2 1.8 0.2 65.3 6.8
Kentucky 0.1 0.2 9.4 2.9 2.6 0.1 82.9 2.0
Louisiana 0.3 0.2 45.5 2.5 0.4 0.0 46.5 4.6
Maine 1.3 0.4 2.6 2.6 2.3 0.2 76.2 14.5
Maryland - - - - - - - -
Massachusetts 0.1 1.7 13.8 26.7 2.2 0.1 42.7 12.6
Michigan 0.5 0.5 31.1 6.4 4.8 0.0 56.2 0.4
Minnesota 7.7 3.0 15.7 12.1 10.6 0.1 48.4 2.5
Mississippi 0.2 0.1 35.8 2.1 0.4 0.0 50.1 11.2
Missouri 0.3 0.2 12.2 6.3 0.3 0.2 71.9 8.6
Montana 16.6 0.1 0.9 3.5 2.2 0.2 55.7 20.7
Nebraska 6.1
0.8 13.1 14.9 3.7 0.1 51.5 9.8
Nevada 0.5 1.6 27.5 24.8 2.2 1.4
33.9 8.1
New Hampshire 0.2 0.5 1.9 4.3 1.5 0.1 81.4 10.1
New Jersey 0.2 1.2 26.9 30.0 0.7 0.1 36.9 3.9
New Mexico 9.3 0.2 2.7 51.0 1.2 0.1 21.9 13.7
New York 0.4 2.9 28.8 26.4 1.8 0.1 38.7 1.0
North Carolina - - - - - - - -
North Dakota 22.2 0.2 7.2 3.4 2.5 0.5 53.9 10.2
Ohio 0.1 0.3 25.2 4.1 2.9 0.1 60.6 6.7
Oklahoma 5.2 0.4 10.6 14.3 21.9 0.2 46.2 1.1
Oregon 2.2 0.7 4.2 10.7 1.8 0.4 60.6 19.5
Pennsylvania 0.1 0.8 21.9 13.0 1.3 0.0 54.5 8.4
Puerto Rico 0.1 0.0 1.0 91.4 0.1 0.0 2.5 4.9
Rhode Island 0.7 1.3 15.3 26.3 2.7 0.1 50.5 3.2
South Carolina 0.2 0.2 37.6 5.3 0.9 0.1 48.5 7.3
South Dakota
42.8 0.1 2.4 6.3 8.8 0.2 36.2 3.2
Tennessee - - - - -
- - -
Texas 0.2 0.8 22.7 41.0 0.9 0.2 30.9 3.4
Utah 2.1 0.9 3.4 21.3 1.3 2.1 68.0 0.9
Vermont 0.0 1.1 4.1 1.1 0.0 0.0 83.6 10.1
Virginia 0.1 0.6 23.0 11.4 0.8 0.2 55.3 8.6
Washington 4.2 1.5 7.5 16.6 5.2 2.2 54.5 8.3
West Virginia 0.0 0.0 3.6 0.8 2.0 0.0 92.4 1.1
Wisconsin 3.8 1.3 17.4 8.2 1.5 0.0 50.3 17.4
Wyoming 3.4 0.3 2.1 10.4 0.0 0.3 79.0 4.4
National 1.4 1.1 21.0 20.3 2.3 0.3 47.4 6.1
Reporting States - - - - - - - -

Child Maltreatment 2022
chApter 5: Perpetrators 74
Table 5–5 Perpetrators by Relationship to Their Victims, 2022 (continues next page)
State Parent
Child Daycare
Provider Foster Parent Friend and Neighbor
Group Home
and Residential
Facility Staff L e g a l G u a r d i a n
Multiple
Relationships
Alabama 5,769 19 14 138 21 37 396
Alaska 1,639 - 31 - - 9 70
Arizona - - - - - - -
Arkansas 5,111 44 12 122 3 13 273
California 38,818 - 169 - 9 - 1,410
Colorado 5,754 14 6 1 2 3 510
Connecticut 3,099 20 15 25 27 81 213
Delaware 556 - - - - 4 35
District of Columbia 958 - 2 - - 4 17
Florida 13,239 26 3 - - 21 1,238
Georgia 6,437 26 28 13 11 50 147
Hawaii 987 - 5 - - 21 46
Idaho 1,548 2 3 13 - 12 15
Illinois 18,920 168 120 - 16 - 1,056
Indiana 11,855 41 25 343 1 47 775
Iowa 6,303
66 10 - 16
67 292
Kansas 1,049 - 6 8 5 - 23
Kentucky 7,050 5 4 194 - 210 633
Louisiana - - - - - - -
Maine - - - - - - -
Maryland 3,065 - 24 - 36 23 214
Massachusetts 14,225 86 47 - 68 104 924
Michigan 13,747 - 73 902 32 75 1,545
Minnesota 2,738 33 45 14 3 38 227
Mississippi 5,336 25 76 164 16 8 241
Missouri 1,990 24 12 109 45 - 168
Montana 1,665 8 12 - 2 7 14
Nebraska 1,038 10 12 - 3 2 88
Nevada 3,869 - 5 121 15 1 218
New Hampshire 772 - - - - 9 41
New Jersey 1,845 16 5 41 2 - 87
New Mexico 4,003 - 3 1 - 53 135
New York 32,314 228 162
- 79 135 378
North Carolina - - - - - - -
North Dakota 701 - 1 19 - - 41
Ohio 11,511 28 67 162 34 - 1,082
Oklahoma 9,110 60 57 - 16 116 612
Oregon 5,300 5 - - - 32 629
Pennsylvania 2,783 19 12 113 15 8 95
Puerto Rico 2,679 - 10 - 25 5 278
Rhode Island 1,539 23 17 - 36 11 128
South Carolina 9,305 1 19 - 15 91 474
South Dakota 846 13 2 - - 3 57
Tennessee 3,710 7 18 410 11 50 88
Texas 31,538 290 60 211 83 - 610
Utah 4,121 12 6 249 23 21 356
Vermont 309 4 4 65 - - 11
Virginia 2,781 64 13 - 11 27 145
Washington 2,537 20 10 1 -
- 78
West Virginia 3,540
2 10 - 4 57 374
Wisconsin 1,971 19 11 30 5 6 128
Wyoming 531 2 1 - 2 4 14
National Total 310,511 1,430 1,247 3,469 692 1,465 16,629
National Percent 76.0 0.4 0.3 0.8 0.2 0.4 4.1
Reporting States 48 35 45 25 34 38 48
Child Maltreatment 2022
chApter 5: Perpetrators 75
Table 5–5 Perpetrators by Relationship to Their Victims, 2022
State Other Other Professional Relative
Unmarried Partner of
Parent U n k n o w n Total Perpetrators
Alabama 604 16 712 288 148 8,162
Alaska 39 - 96 63 17 1,964
Arizona - - - - - -
Arkansas 694 34 824 273 232 7,635
California 2 - 2,078 2,803 - 45,289
Colorado 328 1 717 4 740 8,080
Connecticut 217 46 146 201 - 4,090
Delaware 67 - 116 51 - 829
District of Columbia 12 - 23 - - 1,016
Florida 660 141 837 895 1,587 18,647
Georgia 515 22 471 177 - 7,897
Hawaii 47 - 33 - 5 1,144
Idaho 1 - 50 49 9 1,702
Illinois 459 64 1,379 917 260 23,359
Indiana 831 16 821 - 547 15,302
Iowa 272 - 445 525 7 8,003
Kansas 214 - 222 - 24 1,551
Kentucky 76 - 597 528 102 9,399
Louisiana
- - - - - -
Maine - - - - - -
Maryland 631 - 628 - 1,346 5,967
Massachusetts 457 62 653 771 414 17,811
Michigan 215 2 930 893 3 18,417
Minnesota 85 1 334 234 16 3,768
Mississippi 208 21 874 307 335 7,611
Missouri 457 21 354 286 159 3,625
Montana 21 - 64 77 - 1,870
Nebraska 60 - 55 51 19 1,338
Nevada 1 - 155 249 9 4,643
New Hampshire - - 30 16 45 913
New Jersey 54 44 175 142 23 2,434
New Mexico 41 - 183 197 52 4,668
New York 551 - 2,393 2,324 33 38,597
North Carolina - - - - - -
North Dakota - - 20 - 70 852
Ohio 2,291 96 2,142 - 1,011 18,424
Oklahoma 724 6 505 44 82 11,332
Oregon
-
- 357 136 1,510 7,969
Pennsylvania 529 100 910 379 77 5,040
Puerto Rico 15 10 100 1 349 3,472
Rhode Island 78 - 34 81 1 1,948
South Carolina 337 - 382 305 1 10,930
South Dakota 17 - 28 44 18 1,028
Tennessee 1,459 5 1,001 66 3 6,828
Texas 1,076 194 5,017 3,040 121 42,240
Utah 548 11 720 257 63 6,387
Vermont 64 1 50 33 15 556
Virginia 232 56 324 117 112 3,882
Washington 37 - 96 206 1 2,986
West Virginia 313 4 296 22 199 4,821
Wisconsin 263 11 311 273 297 3,325
Wyoming 27 1 30 1 - 613
National Total 15,829 986 28,718 17,326 10,062 408,364
National Percent 3.9 0.2 7.0 4.2 2.5 100.0
Reporting States 45 26 48 41 41 48

chApter 6: Services 76
Child Maltreatment 2022
Services
The mandate of child protection is not only to investigate or assess maltreatment allegations,
but also to provide services. CPS agencies promote children’s safety and well-being with a
broad range of prevention activities and by providing services to children who were maltreated
or are at-risk of maltreatment. CPS agencies may use several options for providing services:
agency staff may provide services directly to children and their families, the agency may hire a
service provider, or CPS may work with other agencies (e.g., public health agencies).
NCANDS collects data for 26 types of services including adoption, employment, mental
health, and substance abuse. States have their own typologies of services, which they map or
crosswalk to the NCANDS services categories. In this chapter, services are examined from two
perspectives:
(1) Prevention services–consists of aggregated data from states about the use of various
funding streams for prevention services, which are provided to parents whose children
are at risk of abuse and neglect. These services are designed to improve child-rearing
competencies of the parents and other caregivers via education on the developmental
stages of childhood and the provision of other types of assistance.
(2)
Postresponse services–consists of case-level data about children who receive services
as a result of an investigation response or alternative response. Postresponse services
address the safety of the child and usually are based on an assessment of the family’s
situation, including service needs and family strengths.
Prevention Services (duplicate count of children)
States and local agencies determine who will receive prevention services, which services will
be offered, and how the services will be provided. Prevention services may be funded by the
state or the following federal programs:
■ Section 106 of Title I of the Child Abuse Prevention and Treatment Act (CAPTA), as
amended [P.L. 100–294] (State Grant): Under this program, states perform a range
of prevention activities, including addressing the needs of infants born with prenatal
drug exposure, referring children not at risk of imminent harm to community services,
implementing criminal record checks for prospective foster and adoptive parents and
other adults in their homes, training child protective services workers, protecting the legal
rights of families and alleged perpetrators, and supporting citizen review panels. CAPTA
requires states to convene multidisciplinary teams to review the circumstances of child
fatalities in the state and make recommendations.
■ Title II of CAPTA, as amended [P.L. 100–294]: The Community-Based Child Abuse
Prevention Grants (CBCAP) provides funding to a lead state agency (designated by the
governor) to support community-based efforts to develop, operate, expand, enhance, and
CHAPTER 6

Child Maltreatment 2022
chApter 6: Services 77
coordinate initiatives, programs, and activities to prevent child abuse and neglect and sup-
port the coordination of resources and activities; and to foster understanding, appreciation
and knowledge of diverse populations in order to effectively prevent and treat child abuse
and neglect.
■ Title IV–B, Subpart 2, as amended [P.L. 107–133] Promoting Safe and Stable Families:
The primary goals of Promoting Safe and Stable Families (PSSF) are to prevent the
unnecessary separation of children from their families, improve the quality of care and
services to children and their families, and ensure permanency for children by reuniting
them with their parents, by adoption, or by another permanent living arrangement. States
are to spend most of the funding for services that address family support, family preserva-
tion, time-limited family reunication, and adoption promotion and support. The services
are designed to help state child welfare agencies and eligible Indian tribes establish and
operate integrated, preventive family preservation services and community-based family
support services for families at risk or in crisis.
■ Title IV–E of the Social Security Act as amended [P.L.115–123] Family First Prevention
Services Act (FFPSA): This act authorized new optional title IV–E funding for time-lim-
ited prevention services for mental health, substance abuse, and in-home parent skill-based
programs for children or youth who are candidates for foster care, pregnant or parenting
youth in foster care, and the parents or kin caregivers of those children and youth. States
do not report these services to NCANDS.
■ Title XX of the Social Security Act, [P.L. 93–647], Social Services Block Grant (SSBG):
This grant is a exible funding source that allows states and territories to tailor social ser-
vice programming to their population’s needs. Through the SSBG, states provide essential
social services that help achieve goals to reduce dependency and promote self-sufciency;
protect children and adults from neglect, abuse and exploitation; and help individuals who
are unable to take care of themselves to stay in their homes or to nd the best institutional
arrangements.
For each funding source, states are asked to provide to NCANDS a count of child recipients.
Some states are not able to report all child recipients and may report a count of family
recipients either instead of or in combination with a count of child recipients. A calculation is
performed on the count of family recipients to derive a child count.
The estimated total child recipient count by funding source is a sum of the reported child
count and the calculated child count. The calculated child count is computed by multiplying
the family count by the average number of children in a family. States are asked to provide
unique and mutually exclusive counts (e.g., if reporting a child in the child count, the child is
not also included in the family count) within each source. However, because a child or family
may receive multiple services, there may be duplication across funding sources.
Based on data from 45 states, the FFY 2022 estimated total child recipients of prevention
services is 1,922,792. See table 6–1 and related notes. This is an increase from the FFY
2021 estimated total child recipients of 1,761,128, based on data from 45 states. For 2022, the
average number of own children under 18 in families is 1.94.
20
20
Source: U.S. Census Bureau, Current Population Survey. (2022). Annual Social and Economic Supplement AVG3.
Average Number of People per Family Household with Own Children Under 18, by Race and Hispanic Origin,
Marital Status, Age, and Education of Householder: 2022 [data le]. Retrieved March 2023 from
https://www.census.gov/data/tables/2022/demo/families/cps-2022.html

Child Maltreatment 2022
chApter 6: Services 78
The funding source with the largest number of estimated total child recipients is Community-
Based Child Abuse Prevention Grants (CBCAP) with 38 states reporting 561,247 estimated
recipients. The Promoting Safe and Stable Families (PSSF) source has 36 states reporting an
estimated total child recipients of 483,862.
21
Due to the nature of these funds and the ways
states use them, the number of recipients uctuates from one year to the next. Information
about state increases and decreases in recipients and funding may be found in Appendix D,
State Commentary. States continue to work on improving the ability to measure prevention
services. Some of the difculties with collecting and reporting these elements are listed below:
■ CPS agencies may contract out some or all prevention services to local community-based
agencies, and they may not report on the number of clients they serve.
■ CPS agencies may have difculty collecting data from all funders or all funded agencies.
■ The prevention program may be on a different scal schedule (e.g., state scal year) and it
may be difcult to provide accurate data on an FFY schedule.
Postresponse Services (duplicate count of children)
All children and families who are involved with a child welfare agency receive services to some
degree. NCANDS and the Child Maltreatment report focus on only those services that were
initiated or continued as a result of the investigation response or alternative response. NCANDS
collects data for 26 services categories, states have their own service categories which they
crosswalk (map) to the NCANDS categories. Not every state reports data for every service.
Readers should see Appendix B, Glossary, for denitions of service categories and Appendix
D, State Commentary, for state-specic information on services reporting.
22
States continue to
work on improving the ability to report postresponse services data. Some states say they are
only able to report on those services that the CPS agency provides and are not able to report on
those services provided by an external agency or vendors.
The analyses include those services that were provided between the report date (date the mal-
treatment report is received) and up to 90 days after the disposition date (date of determination
about whether the maltreatment occurred). For services that began prior to the report date, if
they continue past the report disposition date, this would imply that the investigation or alterna-
tive response reafrmed the need and continuation of the services, and they should be reported
to NCANDS as postresponse services. Services that do not meet the denition of postresponse
services are those that (1) began prior to the report date but did not continue past the disposition
date or (2) began more than 90 days after the disposition date.
During FFY 2022, 897,486 children received postresponse services from a CPS agency. Fifty-
one states reported 55.0 percent of duplicate victims received postresponse services and 20.3
percent of duplicate nonvictims received postresponse services. See table 6–2 and related notes.
This is a decrease from FFY 2021 when 50 states reported 1,051,818 children who received
postresponse services. Comments provided by states attribute changes in FFY 2022 data when
compared with 2021 are due to improved reporting. One state was previously reporting services
that did not continue past the disposition date.
23
Children who received postresponse services
are counted per response by CPS and may be counted more than once. States provide data on
the start of postresponse services.
21
P.L. 116–94 Family First Transition Act of 2020 renamed this program to Marylee Allen Promoting Safe and Stable
Families.
22
For a listing of all 26 services categories and denitions, please see the NCANDS Child File Code Book on the Children’s
Bureau website at https://www.acf.hhs.gov/cb/training-technical-assistance/ncands-child-le-codebook
23
California

Child Maltreatment 2022
chApter 6: Services 79
Table 6–3 calculates the national average by dividing the total number of days to services by
the number of children who received services on or after the report date (mean). Based on data
from 45 states, the average number of days from receipt of a report to initiation of services for
FFY 2022 is 40 days and a midpoint (median) of 22 days. See table 6–3 and related notes. This
is a increase from FFY 2021 when 44 states reported an average of 29 days and a median of
18 days. Several states provided comments about the increase in days to services receipt and
attributed the increase to: only counting the children with services during the reporting period,
improved data entry, a new Comprehensive Child Welfare System (CCWIS), new service
interface, and the addition of three services to the service array.
Table 6–4 displays the number of children who received foster care services and are
removed from home. Only the children who are removed from their home on or after the
report date are counted. This is because some children were already in foster care when
the allegation of maltreatment was made, and readers and researchers want to know
the number of children who were removed as a result of the investigation or alternative
response. Readers interested in more complete adoption and foster care statistics should
refer to the Adoption and Foster Care Analysis and Reporting System (AFCARS) data at
https://www.acf.hhs.gov/cb/data-research/adoption-fostercare. AFCARS collects case-level
information on all children in foster care and those who are adopted with title IV–E agency
involvement.
Based on FFY 2022 data from 49 states, 104,747 victims (19.6%) and 40,702 nonvictims
(1.4%) were removed from their homes. For FFY 2021, 48 states reported 113,324 victims
(20.2%) and 43,252 nonvictims (1.6%) were removed. Some states report low percentages
of victims and nonvictims who received foster care services due to system limitations or
other difculties with collecting and reporting the data as mentioned above. See table 6–4
and related notes. There may be several explanations as to why nonvictims are placed in
foster care. For example, if one child in a household is deemed to be in danger or at-risk of
maltreatment, the state may remove all of the children in the household to ensure their safety.
(E.g., if a CPS worker nds a drug lab in a house or nds a severely intoxicated caregiver, the
worker may remove all children, even if there is only a maltreatment allegation for one child
in the household.) Another reason for a nonvictim to be removed has to do with voluntary
placements. This is when a parent voluntarily agrees to place a child in foster care even if the
child was not determined to be a victim of maltreatment.
Twenty-ve states reported 51,193 victims (19.0%) have court-appointed representatives.
See table 6–5 and related notes. This is a decrease from FFY 2021 when 25 states reported
52,222 victims (19.7%) had court-appointed representatives. The representatives act on
behalf of a child in court proceedings and make recommendations to the court in the best
interests of the child. According to states, Guardians ad Litem, children’s attorneys, and
Court Appointed Special Advocates (CASAs) are included in these counts to NCANDS.
These numbers are likely to be an undercount given the statutory requirement in CAPTA that
says, “in every case involving a victim of child abuse or neglect which results in a judicial
proceeding, a guardian ad litem who has received training appropriate to the role, including
training in early childhood, child and adolescent development, and who may be an attorney
Child Maltreatment 2022
chApter 6: Services 80
or a court-appointed special advocate who has received training appropriate to that role (or
both), shall be appointed to represent the child in such proceedings…” States provide the
following possible reasons for not reporting data:
■ The data is provided by contracted vendors and is not available at the child level.
■ The lack of a centralized database.
■ The court system is not able to interface with the child welfare system.
■ The court system does not record information at the child level.
The NCANDS Technical Team is continuing to work with states on improving reporting in this
area.
History of Receiving Services (unique count of victims)
Two data elements in the Agency File collect information on histories of victims with prior
CPS involvement. For FFY 2022, 28 states reported 49,703 victims (15.2%) received fam-
ily preservation services within the previous 5 years. This is an increase from FFY 2021
when 29 states reported 45,440 victims (14.0%) received family preservation services.
See table 6–6 and related notes. Several states subcontract family preservation services to
outside vendors and are not able to report this data to NCANDS. FFY 2022 data from 37
states show 18,327 victims (4.8%) were reunited with their families within the previous
5 years. This is similar to FFY 2021 when 38 states reported 19,588 victims (4.8%) were
reunited. See table 6–7 and related notes.
Part C of the Individuals with Disabilities Education Act (IDEA)
(unique count of victims)
Federal guidance asks for states to report the number of victims who are younger than 3 years
who are eligible for and referred to agencies providing early intervention services under Part
C of the Individuals with Disabilities Education Act. However, some states have policies in
place to allow older children to be considered eligible for referral and receipt of these services
and these states may report victims who are older than 3 years. NCANDS uses the following
denitions:
■ Number of Children Eligible for Referral to Agencies Providing Early Intervention
Services Under Part C of the Individuals with Disabilities Education Act: a unique count
of the number of victims eligible for referral to agencies providing early intervention
services under Part C of the Individuals with Disabilities Act.
■ Number of Children Referred to Agencies Providing Early Intervention Services Under
Part C of the Individuals with Disabilities Education Act: a unique count of the number of
victims actually referred to agencies providing early intervention services under Part C of
the Individuals with Disabilities Education Act.
Thirty-eight states reported 88,725 victims who are eligible for referral to agencies providing
early intervention services and 32 states reported 37,588 victims who are referred. Of the states
that are able to report both the victims who are eligible and referred (31 states), 57.9 percent of
victims who are eligible are referred to the agencies. See table 6–8 and related notes.
Exhibit and Table Notes
The following pages contain the data tables referenced in chapter 6. Specic information
about state submissions can be found in Appendix D, State Commentary. Additional infor-
mation regarding the exhibits and tables is provided below.

Child Maltreatment 2022
chApter 6: Services 81
General
During data analyses, thresholds are set to ensure data quality is balanced with the need to
report data from as many states as possible. States may be excluded from an analysis for data
quality issues. Exclusion rules are listed in the table notes below. Not every table has exclu-
sion rules or notes.
■ The data for all tables are from the Child File unless otherwise noted.
■ Due to the large number of categories, most services are defined in Appendix B, Glossary.
■ The row labeled Reporting States displays the count of states that provide data for that
analysis.
■ The Child File Codebook, which includes the services fields, is located on the Children’s
Bureau website at https://www.acf.hhs.gov/cb/training-technical-assistance/ncands-child-
file-codebook.
■ National totals and calculations appear in a single row labeled National instead of separate
rows labeled total, rate, or percent.
■ Dashes are inserted into cells without any data for this analysis.
Table 6–1 Children Who Received Prevention Services by
Funding Source, 2022
■ Data is from the Agency File.
■ The number of total recipients is a duplicate count.
■ Children may be counted more than once, under a single funding source and across fund-
ing sources.
■ Children who received prevention services may have received them via CPS or other
agencies.
■ Funds used for public service announcements or campaigns are not included in NCANDS
reporting.
■ Some programs maintain their data as counts of families rather than counts of children. If a
family count was provided, the number of families was multiplied by the average number of
children per family (1.94) and used as the estimate of the number of children who received
services or added to any counts of children that were also provided. The estimated total child
recipient count by funding source is a sum of the reported child count and the calculated
child count.
Table 6–2 Children Who Received Postresponse Services, 2022
■ The numbers of victims and nonvictims are duplicate counts.
■ A child is counted each time that a CPS response is completed and services are provided.
■ This analysis includes only those services that continue past or are initiated after the
completion of the CPS response.
■ States are excluded from this analysis if they report fewer than 1.0 percent of victims or
fewer than 1.0 percent of nonvictims with postresponse services.
■ A couple of states reported that 100.0 percent of its victims, nonvictims, or both received
services. These states may be reporting case management services and information and
referral services for all children who received a CPS response.
Table 6–3 Average and Median Number of Days to Initiation of Services, 2022
■ The number of children is a duplicate count.
■ This analysis uses subset of children whose service date is the same day or later than the report
date. The subset is created by excluding any report with a service date prior to the report date.
■ The average is displayed at the state and national level. The state average is rounded to
a whole day. The national average is calculated by dividing the total number of days to

chApter 6: Services 82
Child Maltreatment 2022
services by the number of children who received services on or after the report date. The
total number of days to the initiation of services is not shown.
■ The median is displayed for both the national and the state level. The median is determined
by nding the midpoint of the number of days to services for children who received ser-
vices on or after the report date.
■ States are excluded from this analysis if they report fewer than 1.0 percent of victims or
fewer than 1.0 percent of nonvictims with postresponse services.
■ States are excluded from this analysis if fewer than 80.0 percent of records with a service
have a service date.
■ States are excluded from this analysis if fewer than 40.0 percent of records with a service
have a service date after the report date.
■ States are excluded from this analysis if more than 40.0 percent of records have the same
report date and service date.
Table 6–4 Children Who Received Foster Care Postresponse Services and
Who Had a Removal Date on or After the Report Date, 2022
■ The numbers of victims and nonvictims are a duplicate count.
■ A child is counted each time that a CPS response is completed and services are provided.
■ Only the children who are removed from their home on or after the report and up to 90
days after the disposition date are counted.
■ States are excluded from this analysis if fewer than 1.0 percent of victims received foster
care services.
■ States were excluded from this analysis if more than 25.0 percent of victims with foster care
services or more than 70.0 percent of nonvictims with foster care services did not have a
removal date.
Table 6–5 Victims with Court-Appointed Representatives, 2022
■ The number of victims is a duplicate count.
■ The NCANDS category of court-appointed representatives includes attorneys and court-
appointed special advocates who represent the interests of the child in a maltreatment
hearing.
■ States are excluded from this analysis if fewer than 5.0 percent of victims have a court-
appointed representative.
Table 6–6 Victims Who Received Family Preservation Services within the
Previous 5 Years, 2022
■ Data is from the Child File and Agency File.
■ The number of victims is a unique count.
Table 6–7 Victims Who Were Reunited with Their Families within the
Previous 5 Years, 2022
■ Data is from the Child File and the Agency File.
■ The number of victims is a unique count.
Table 6–8 IDEA: Victims Who Were Eligible and Victims Who Were
Referred to Part C Agencies, 2022
■ Data is from the Agency File.
■ The number of victims is a unique count.

chApter 6: Services 83
Child Maltreatment 2022
Table 6–1 Children Who Received Prevention Services by Funding Source, 2022
(continues next page)
State
Child Abuse and
Neglect State
Grant (State Grant)
Children
State Grant
Calculated Child
Count
State Grant
Estimated Total
Child Recipients
Community-Based
Child Abuse
Prevention Grants
(CBCAP) Children
CBCAP Calculated
Child Count
CBCAP Estimated
Total Child
Recipients
Alabama - 1,197 1,197 1,634 - 1,634
Alaska - - - 354 - 354
Arizona - - - - 5,449 5,449
Arkansas 19 175 194 - 1,752 1,752
California - 1,383 1,383 1,933 4,988 6,921
Colorado - - - - - -
Connecticut 37,202 - 37,202 - 378 378
Delaware - - - - - -
District of Columbia 54 - 54 - - -
Florida - - - - - -
Georgia 13,176 44,240 57,416 6,963 21,759 28,722
Hawaii - - - - 1,502 1,502
Idaho - - - 5,143 8,239 13,382
Illinois 2,632 4,437 7,069 5,252 7,964 13,216
Indiana 23,588 - 23,588 3,642 - 3,642
Iowa - 142 142 - 1,410 1,410
Kansas -
- - - - -
Kentucky - - - 1,160 - 1,160
Louisiana
- - - 18,636 30,285 48,921
Maine - - - - - -
Maryland - - - - - -
Massachusetts - - - - - -
Michigan 2,225 5,958 8,183 177,575 32,012 209,587
Minnesota 3,812 - 3,812 8,278 - 8,278
Mississippi - - - 3,147 8,270 11,417
Missouri - - - 648 - 648
Montana - - - 959 1,020 1,979
Nebraska - - - 3,143 - 3,143
Nevada 42 - 42 1,785 - 1,785
New Hampshire - - - 2,730 - 2,730
New Jersey - 1,868 1,868 62,679 47,827 110,506
New Mexico - - - 131 - 131
New York - - - 2,278 4,456 6,734
North Carolina - - - 229 275 504
North Dakota - - - 217 2,089 2,306
Ohio - -
- 1,284 1,385 2,669
Oklahoma - - - - 871 871
Oregon -
- - - - -
Pennsylvania - - - 4,078 - 4,078
Puerto Rico 5,224 44,216 49,440 994 4,928 5,922
Rhode Island - - - - - -
South Carolina - - - - - -
South Dakota - - - 1,165 918 2,083
Tennessee - - - - - -
Texas - - - 887 1,989 2,876
Utah - - - 11,558 - 11,558
Vermont - - - - - -
Virginia 54,900 - 54,900 1,179 5,461 6,640
Washington 4,354 - 4,354 - 2,031 2,031
West Virginia 7,558 11,112 18,670 22,830 - 22,830
Wisconsin - - - - - -
Wyoming - - - 3,500 7,997 11,497
National 154,786 114,728 269,514 355,991 205,256 561,247
Reporting States 13 10 17 31 25 38

Child Maltreatment 2022
chApter 6: Services 84
Table 6–1 Children Who Received Prevention Services by Funding Source, 2022
(continues next page)
State
Promoting Safe
and Stable Families
(PSSF) Children
PSSF Calculated
Child Count
PSSF Estimated
Total Child
Recipients
Social Services
Block Grant (SSBG)
Children
SSBG Calculated
Child Count
SSBG Estimated
Total Child
Recipients
Alabama - 35,479 35,479 13,768 - 13,768
Alaska 243 163 406 125 4,210 4,335
Arizona - 7,463 7,463 - - -
Arkansas 20 522 542 - 60,159 60,159
California 6,237 43,239 49,476 - - -
Colorado - - - - - -
Connecticut 48,383 - 48,383 - - -
Delaware 1,843 - 1,843 - 811 811
District of Columbia 149 - 149 - - -
Florida 32,453 - 32,453 - - -
Georgia 15,358 - 15,358 - - -
Hawaii - - - - - -
Idaho 809 - 809 109 - 109
Illinois - - - 4,894 7,979 12,873
Indiana 1,775 - 1,775 15 - 15
Iowa - 1,042 1,042 - - -
Kansas 1,757 - 1,757 -
- -
Kentucky 618 - 618 - - -
Louisiana
2,704 3,325 6,029 6,049 - 6,049
Maine - - - - - -
Maryland - - - 13,433 - 13,433
Massachusetts - - - - - -
Michigan 11,756 9,423 21,179 - - -
Minnesota 1,907 - 1,907 10,937 - 10,937
Mississippi 537 - 537 - - -
Missouri - - - - - -
Montana 2,310 3,603 5,913 - - -
Nebraska - 14,125 14,125 - - -
Nevada 7,174 - 7,174 24,109 - 24,109
New Hampshire 120 - 120 413 - 413
New Jersey - - - - - -
New Mexico 2,138 - 2,138 - - -
New York - - - - - -
North Carolina 2,015 3,116 5,131 1,040 2,018 3,058
North Dakota - 3,944 3,944 - - -
Ohio - - - 35,097 -
35,097
Oklahoma 140 386 526 - - -
Oregon -
1,808 1,808 - 3,449 3,449
Pennsylvania 3,919 - 3,919 147,277 - 147,277
Puerto Rico 1,398 3,251 4,649 1,098 3,641 4,739
Rhode Island - 2,797 2,797 - - -
South Carolina - - - - - -
South Dakota - - - - - -
Tennessee - - - - - -
Texas 18,403 31,422 49,825 - - -
Utah - - - - - -
Vermont - - - - - -
Virginia 18,016 31,445 49,461 - - -
Washington 5,244 19,759 25,003 - - -
West Virginia 27,846 48,651 76,497 31,537 19,790 51,327
Wisconsin - - - - - -
Wyoming 1,900 1,727 3,627 4,314 - 4,314
National 217,172 266,690 483,862 294,215 102,058 396,273
Reporting States 29 21 36 16 8 19

Child Maltreatment 2022
chApter 6: Services 85
Table 6–1 Children Who Received Prevention
Services by Funding Source, 2022
State
Other Funding
(Other) Children
Other Calculated
Child Count
Other Estimated
Total Child
Recipients
Estimated Total
Child Recipients
Alabama - - - 52,078
Alaska 137 83 220 5,315
Arizona - 6,866 6,866 19,778
Arkansas - - - 62,647
California 781 8,947 9,728 67,508
Colorado - - - -
Connecticut 2,378 58 2,436 88,400
Delaware 2,896 3,021 5,917 8,571
District of Columbia 1,139 - 1,139 1,342
Florida - - - 32,453
Georgia - - - 101,496
Hawaii - - - 1,502
Idaho 141 - 141 14,441
Illinois - - - 33,158
Indiana 8,914 - 8,914 37,934
Iowa - - - 2,594
Kansas 14 - 14 1,771
Kentucky 230 - 230 2,008
Louisiana 2,205 5,601 7,806 68,805
Maine - - - -
Maryland - - - 13,433
Massachusetts - - - -
Michigan - - - 238,948
Minnesota - - - 24,934
Mississippi 1,197 - 1,197
13,151
Missouri 1,147 - 1,147
1,795
Montana - - - 7,892
Nebraska - - - 17,268
Nevada 15,524 - 15,524 48,634
New Hampshire 1,247 - 1,247 4,510
New Jersey - 5,775 5,775 118,149
New Mexico 2,450 2,937 5,387 7,656
New York 73,940 - 73,940 80,674
North Carolina 3,255 5,948 9,203 17,896
North Dakota - - - 6,250
Ohio - - - 37,766
Oklahoma 3,987 8,804 12,791 14,188
Oregon - 332 332 5,589
Pennsylvania 5,862 - 5,862 161,136
Puerto Rico 789 3,851 4,640 69,391
Rhode Island - - - 2,797
South Carolina - - - -
South Dakota - - - 2,083
Tennessee - - - -
Texas - - - 52,701
Utah 7,708 - 7,708 19,266
Vermont - - - -
Virginia 4,977 8,191 13,168 124,169
Washington - - - 31,388
West Virginia 10,565 - 10,565 179,890
Wisconsin - - - -
Wyoming - -
- 19,437
National 151,483 60,414 211,897 1,922,792
Reporting States 23 13 26 45

Child Maltreatment 2022
chApter 6: Services 86
Table 6–2 Children Who Received Postresponse Services, 2022
State Victims
Victims Who
Received
Postresponse
Services
Victims Who
Received
Postresponse
Services Percent Nonvictims
Nonvictims
Who Received
Postresponse
Services
Nonvictims
Who Received
Postresponse
Services Percent
Alabama 11,941 6,818 57.1 27,629 4,541 16.4
Alaska 2,794 1,494 53.5 9,544 464 4.9
Arizona 13,540 4,620 34.1 51,631 1,015 2.0
Arkansas 9,363 7,781 83.1 55,740 8,084 14.5
California 53,973 34,789 64.5 295,721 61,414 20.8
Colorado 10,572 1,919 18.2 38,824 675 1.7
Connecticut 5,394 5,255 97.4 12,578 11,744 93.4
Delaware 1,104 440 39.9 12,514 1,589 12.7
District of Columbia 1,689 215 12.7 8,002 184 2.3
Florida 25,697 9,405 36.6 276,720 9,003 3.3
Georgia 10,820 8,263 76.4 113,262 66,232 58.5
Hawaii 1,342 784 58.4 4,521 581 12.9
Idaho 2,065 1,231 59.6 10,848 1,017 9.4
Illinois 37,077 17,096 46.1 171,695 27,633 16.1
Indiana 20,184 11,100 55.0 145,902 9,640 6.6
Iowa 13,150 13,150 100.0 43,055 43,055 100.0
Kansas 1,974 1,060
53.7 29,422 7,112 24.2
Kentucky 13,492 9,415 69.8 49,442 3,155 6.4
Louisiana
7,861 4,046 51.5 18,092 1,136 6.3
Maine 4,094 898 21.9 16,516 215 1.3
Maryland 7,080 1,344 19.0 18,567 1,126 6.1
Massachusetts 24,582 22,347 90.9 54,621 32,602 59.7
Michigan 24,916 9,659 38.8 150,151 17,941 11.9
Minnesota 5,521 3,333 60.4 32,587 8,161 25.0
Mississippi 9,797 4,489 45.8 35,338 2,634 7.5
Missouri 4,004 2,352 58.7 70,288 14,617 20.8
Montana 2,913 1,327 45.6 10,703 774 7.2
Nebraska 2,126 1,588 74.7 32,784 12,710 38.8
Nevada 6,273 3,047 48.6 30,095 5,309 17.6
New Hampshire 1,053 618 58.7 14,448 2,028 14.0
New Jersey 3,217 1,655 51.4 86,159 14,088 16.4
New Mexico 6,616 1,650 24.9 25,739 1,723 6.7
New York - - - - - -
North Carolina 24,803 16,665 67.2 106,363 21,133 19.9
North Dakota 1,154 705 61.1 4,035 482 11.9
Ohio 24,677 15,071 61.1
98,896 26,953 27.3
Oklahoma 14,240 12,280 86.2 44,436 30,944 69.6
Oregon 11,397
3,447 30.2 46,576 2,949 6.3
Pennsylvania 5,201 1,119 21.5 34,574 2,086 6.0
Puerto Rico 5,127 4,310 84.1 9,276 2,976 32.1
Rhode Island 2,601 1,023 39.3 4,410 539 12.2
South Carolina 15,680 5,210 33.2 67,233 8,293 12.3
South Dakota 1,546 718 46.4 2,933 222 7.6
Tennessee 7,024 7,024 100.0 95,990 89,337 93.1
Texas 55,942 19,595 35.0 267,740 8,124 3.0
Utah 9,253 7,907 85.5 22,223 14,371 64.7
Vermont 761 258 33.9 3,813 509 13.3
Virginia 4,694 1,270 27.1 45,451 2,222 4.9
Washington 3,995 2,109 52.8 56,945 3,800 6.7
West Virginia 5,740 5,555 96.8 44,399 5,461 12.3
Wisconsin 4,259 1,721 40.4 31,890 2,213 6.9
Wyoming 851 701 82.4 3,463 2,794 80.7
National 545,169 299,876 55.0 2,943,784 597,610 20.3
Reporting States 51 51 - 51 51 -

Child Maltreatment 2022
chApter 6: Services 87
Table 6–3 Average and Median Number of Days to Initiation of Services, 2022
State Children Who Received Services
Children Who Received Services
on or After the Report Date
Average Number of Days
to Initiation of Services
Median Number of Days
to Initiation of Services
Alabama 11,359 11,323 41 35
Alaska 1,958 1,958 46 34
Arizona 5,635 4,720 39 15
Arkansas 15,865 15,166 39 40
California 96,203 90,241 58 43
Colorado 2,594 2,356 22 14
Connecticut - - - -
Delaware 2,029 2,029 79 65
District of Columbia 399 391 49 35
Florida 18,408 12,497 31 14
Georgia 74,495 73,228 13 6
Hawaii 1,365 1,052 21 2
Idaho 2,248 2,246 27 20
Illinois 44,729 21,070 48 33
Indiana 20,740 20,691 31 19
Iowa 56,205 56,205 25 28
Kansas 8,172 5,172 51 32
Kentucky 12,570 10,838 78 65
Louisiana 5,182 4,885 44 27
Maine 1,113 916 29 10
Maryland - - - -
Massachusetts 54,949 37,230 14 14
Michigan 27,600 14,722 44 36
Minnesota 11,494 11,494 63 45
Mississippi 7,123 7,069
28 28
Missouri 16,969 14,877 55
37
Montana 2,101 1,663 48 30
Nebraska 14,298 6,279 56 36
Nevada 8,356 8,035 66 56
New Hampshire 2,646 2,221 60 47
New Jersey 15,743 10,508 50 43
New Mexico 3,373 2,673 31 15
New York - - - -
North Carolina - - - -
North Dakota 1,187 1,177 57 47
Ohio 42,024 33,420 42 34
Oklahoma 43,224 43,136 50 49
Oregon 6,396 4,997 56 27
Pennsylvania 3,205 2,377 29 29
Puerto Rico 7,286 5,859 84 28
Rhode Island 1,562 1,057 35 21
South Carolina 13,503 7,916 39 42
South Dakota - - - -
Tennessee - - - -
Texas 27,719 27,208 44 26
Utah - - - -
Vermont 767 479 44 17
Virginia 3,492 2,000 38 23
Washington 5,909 4,636 35 21
West Virginia 11,016 6,475 37 22
Wisconsin 3,934 3,934 51 56
Wyoming 3,495
3,467 13 6
National 720,640 601,893 40 22
Reporting States 45 45 45 45

Child Maltreatment 2022
chApter 6: Services 88
Table 6–4 Children Who Received Foster Care Postresponse Services and
Who had a Removal Date On or After the Report Date, 2022
State Victims
Victims Who
Received Foster Care
Postresponse Services
Victims Who
Received Foster Care
Postresponse Services
Percent Nonvictims
Nonvictims Who
Received Foster Care
Postresponse Services
Nonvictims Who
Received Foster Care
Postresponse Services
Percent
Alabama 11,941 2,002 16.8 27,629 661 2.4
Alaska 2,794 651 23.3 9,544 288 3.0
Arizona 13,540 2,363 17.5 51,631 191 0.4
Arkansas 9,363 1,478 15.8 55,740 885 1.6
California 53,973 18,144 33.6 295,721 5,426 1.8
Colorado 10,572 1,201 11.4 38,824 188 0.5
Connecticut 5,394 791 14.7 12,578 215 1.7
Delaware 1,104 188 17.0 12,514 62 0.5
District of Columbia 1,689 167 9.9 8,002 45 0.6
Florida 25,697 8,658 33.7 276,720 2,431 0.9
Georgia 10,820 2,468 22.8 113,262 1,503 1.3
Hawaii 1,342 563 42.0 4,521 79 1.7
Idaho 2,065 718 34.8 10,848 161 1.5
Illinois 37,077 5,653 15.2 171,695 1,972 1.1
Indiana 20,184 5,358 26.5 145,902 1,765 1.2
Iowa 13,150 1,551 11.8 43,055 71 0.2
Kansas 1,974 155 7.9 29,422
615 2.1
Kentucky 13,492 698 5.2 49,442 126 0.3
Louisiana
7,861 2,225 28.3 18,092 300 1.7
Maine 4,094 832 20.3 16,516 78 0.5
Maryland 7,080 624 8.8 18,567 130 0.7
Massachusetts 24,582 3,180 12.9 54,621 837 1.5
Michigan 24,916 2,760 11.1 150,151 956 0.6
Minnesota 5,521 1,526 27.6 32,587 1,666 5.1
Mississippi 9,797 1,235 12.6 35,338 309 0.9
Missouri 4,004 1,400 35.0 70,288 3,100 4.4
Montana 2,913 1,093 37.5 10,703 295 2.8
Nebraska 2,126 744 35.0 32,784 925 2.8
Nevada 6,273 2,101 33.5 30,095 634 2.1
New Hampshire 1,053 392 37.2 14,448 251 1.7
New Jersey 3,217 553 17.2 86,159 1,068 1.2
New Mexico 6,616 773 11.7 25,739 396 1.5
New York - - - - - -
North Carolina 24,803 3,109 12.5 106,363 388 0.4
North Dakota 1,154 319 27.6 4,035 105 2.6
Ohio 24,677 5,216 21.1 98,896 2,463
2.5
Oklahoma 14,240 2,919 20.5 44,436 41 0.1
Oregon 11,397
2,219 19.5 46,576 673 1.4
Pennsylvania - - - - - -
Puerto Rico 5,127 421 8.2 9,276 28 0.3
Rhode Island 2,601 502 19.3 4,410 79 1.8
South Carolina 15,680 2,106 13.4 67,233 681 1.0
South Dakota 1,546 677 43.8 2,933 176 6.0
Tennessee 7,024 1,429 20.3 95,990 3,721 3.9
Texas 55,942 7,351 13.1 267,740 744 0.3
Utah 9,253 921 10.0 22,223 30 0.1
Vermont 761 148 19.4 3,813 158 4.1
Virginia - - - - - -
Washington 3,995 1,409 35.3 56,945 1,322 2.3
West Virginia 5,740 1,871 32.6 44,399 617 1.4
Wisconsin 4,259 1,488 34.9 31,890 1,802 5.7
Wyoming 851 397 46.7 3,463 45 1.3
National 535,274 104,747 19.6 2,863,759 40,702 1.4
Reporting States 49 49 49 49 49 49

chApter 6: Services 89
Child Maltreatment 2022
Table 6–5 Victims with Court-Appointed Representatives, 2022
State Victims
Victims with Court-Appointed
Representatives
Victims with Court-Appointed
Representatives Percent
Alabama 11,941 806 6.7
Alaska 2,794 641 22.9
Arizona 13,540 1,327 9.8
Arkansas - - -
California 53,973 14,909 27.6
Colorado - - -
Connecticut - - -
Delaware 1,104 206 18.7
District of Columbia - - -
Florida - - -
Georgia 10,820 2,237 20.7
Hawaii 1,342 703 52.4
Idaho - - -
Illinois - - -
Indiana 20,184 4,087 20.2
Iowa 13,150 1,834 13.9
Kansas - - -
Kentucky 13,492 3,283 24.3
Louisiana - - -
Maine - - -
Maryland - - -
Massachusetts 24,582 4,290 17.5
Michigan - - -
Minnesota 5,521 1,134 20.5
Mississippi 9,797 850 8.7
Missouri - - -
Montana 2,913 527 18.1
Nebraska 2,126 824 38.8
Nevada 6,273 528 8.4
New Hampshire 1,053 526 50.0
New Jersey - - -
New Mexico 6,616 726 11.0
New York -
- -
North Carolina - - -
North Dakota - - -
Ohio 24,677 4,846 19.6
Oklahoma 14,240 1,028 7.2
Oregon 11,397 2,584 22.7
Pennsylvania - - -
Puerto Rico - - -
Rhode Island 2,601 537 20.6
South Carolina - - -
South Dakota - - -
Tennessee - - -
Texas - - -
Utah 9,253 1,471 15.9
Vermont 761 208 27.3
Virginia 4,694 1,081 23.0
Washington - - -
West Virginia - - -
Wisconsin - - -
Wyoming - - -
National 268,844 51,193 19.0
Reporting States 25 25 -

chApter 6: Services 90
Child Maltreatment 2022
Table 6–6 Victims Who Received Family Preservation
Services within the Previous 5 Years, 2022
State Victims
Victims Who Received Family
Preservation Services within the
Previous 5 Years
Victims Who Received Family
Preservation Services within the
Previous 5 Years Percent
Alabama 11,618 1,067 9.2
Alaska - - -
Arizona - - -
Arkansas 8,927 1,658 18.6
California 50,869 7,232 14.2
Colorado - - -
Connecticut - - -
Delaware - - -
District of Columbia 1,574 230 14.6
Florida 24,505 4,022 16.4
Georgia 10,524 1,596 15.2
Hawaii - - -
Idaho 2,005 1,008 50.3
Illinois 32,433 7,503 23.1
Indiana - - -
Iowa - - -
Kansas 1,861 435 23.4
Kentucky 12,340 1,217 9.9
Louisiana 7,572 1,433 18.9
Maine - - -
Maryland - - -
Massachusetts 22,075 7,682 34.8
Michigan - - -
Minnesota 5,299 1,812 34.2
Mississippi 9,028 55 0.6
Missouri 3,932 405 10.3
Montana - - -
Nebraska 2,026 291 14.4
Nevada 5,851 425 7.3
New Hampshire 1,034 124 12.0
New Jersey 3,146 228 7.2
New Mexico 5,817
409 7.0
New York -
- -
North Carolina - - -
North Dakota - - -
Ohio - - -
Oklahoma 13,546 488 3.6
Oregon 10,507 671 6.4
Pennsylvania - - -
Puerto Rico 4,320 895 20.7
Rhode Island 2,444 669 27.4
South Carolina - - -
South Dakota - - -
Tennessee 6,924 1,304 18.8
Texas 54,207 6,572 12.1
Utah 8,765 20 0.2
Vermont - - -
Virginia - - -
Washington 3,389 252 7.4
West Virginia - - -
Wisconsin - - -
Wyoming - - -
National 326,538 49,703 15.2
Reporting States 28 28 -

chApter 6: Services 91
Child Maltreatment 2022
Table 6–7 Victims Who Were Reunited with Their
Families within the Previous 5 Years, 2022
State Victims
Victims Who Were Reunited with
Their Families within the Previous
5 Years
Victims Who Were Reunited with
Their Families within the Previous 5
Years Percent
Alabama 11,618 253 2.2
Alaska 2,581 255 9.9
Arizona - - -
Arkansas 8,927 173 1.9
California - - -
Colorado 9,777 389 4.0
Connecticut 5,032 185 3.7
Delaware 1,077 11 1.0
District of Columbia - - -
Florida 24,505 1,930 7.9
Georgia 10,524 437 4.2
Hawaii 1,228 85 6.9
Idaho 2,005 130 6.5
Illinois 32,433 1,706 5.3
Indiana 19,185 1,397 7.3
Iowa - - -
Kansas 1,861 269 14.5
Kentucky 12,340 1,153 9.3
Louisiana 7,572 319 4.2
Maine - - -
Maryland 6,564 227 3.5
Massachusetts 22,075 1,701 7.7
Michigan - - -
Minnesota 5,299 415 7.8
Mississippi 9,028 25 0.3
Missouri 3,932 171 4.3
Montana - - -
Nebraska 2,026 173 8.5
Nevada 5,851 497 8.5
New Hampshire 1,034 69 6.7
New Jersey 3,146 162 5.1
New Mexico 5,817
331 5.7
New York -
- -
North Carolina 23,134 442 1.9
North Dakota - - -
Ohio 22,439 1,188 5.3
Oklahoma 13,546 597 4.4
Oregon 10,507 998 9.5
Pennsylvania - - -
Puerto Rico 4,320 21 0.5
Rhode Island 2,444 165 6.8
South Carolina 14,572 194 1.3
South Dakota - - -
Tennessee 6,924 254 3.7
Texas 54,207 1,043 1.9
Utah 8,765 285 3.3
Vermont - - -
Virginia - - -
Washington 3,389 367 10.8
West Virginia - - -
Wisconsin 4,082 310 7.6
Wyoming - - -
National 383,766 18,327 4.8
Reporting States 37 37 -
chApter 6: Services 92
Child Maltreatment 2022
Table 6–8 IDEA: Victims Who Were Eligible and Victims Who
Were Referred to Part C Agencies, 2022
State
Victims Who Were Eligible for
Referral to Part C Agencies
Victims Who Were Referred to
Part C Agencies
Victims Who Were Referred to
Part C Agencies Percent
Alabama 3,383 515 15.2
Alaska 671 671 100.0
Arizona 775 64 8.3
Arkansas 2,725 - -
California 14,485 1,654 11.4
Colorado 2,378 1,661 69.8
Connecticut 1,266 625 49.4
Delaware - - -
District of Columbia 404 5 1.2
Florida - - -
Georgia 7,211 6,789 94.1
Hawaii - - -
Idaho 672 542 80.7
Illinois - - -
Indiana - - -
Iowa 3,422 3,422 100.0
Kansas 183 140 76.5
Kentucky 3,409 - -
Louisiana 3,378 3,111 92.1
Maine 892 892 100.0
Maryland - - -
Massachusetts 4,871 - -
Michigan - - -
Minnesota 1,631 1,575 96.6
Mississippi 566 319 56.4
Missouri 732 148 20.2
Montana - - -
Nebraska 509 509 100.0
Nevada 651 621 95.4
New Hampshire 290 - -
New Jersey 672 566 84.2
New Mexico
1,256 884 70.4
New York 10,583
- -
North Carolina - 805 -
North Dakota 374 360 96.3
Ohio 4,222 4,222 100.0
Oklahoma 3,897 789 20.2
Oregon 2,370 - -
Pennsylvania - - -
Puerto Rico 617 101 16.4
Rhode Island 624 616 98.7
South Carolina 4,034 2,804 69.5
South Dakota 505 410 81.2
Tennessee - - -
Texas - - -
Utah 1,562 1,562 100.0
Vermont - - -
Virginia - - -
Washington 849 200 23.6
West Virginia 1,500 789 52.6
Wisconsin 939 - -
Wyoming 217 217 100.0
National 88,725 37,588 42.4
Reporting States 38 32 31
National for States
Reporting Both Victims
Eligible and Referred
63,538 36,783 57.9
Reporting States for
States Reporting Both
Victims Eligible and Referred
31 31 -

Child Maltreatment 2022
chApter 7: Special Focus 93
The purpose of this chapter is to highlight analyses of specic subsets of children or data
analyses focusing on a specic topic. The analyses in this chapter include both new analyses
not presented in the previous chapters as well as existing analyses. The information is presented
together in this chapter to allow readers to see the complete analytical picture of the topic.
Introduction
Each state denes child abuse and neglect in its own statutes and policies and the child
welfare agencies determine the appropriate response for the alleged maltreatment based
on those statutes and policies. The purpose of the National Child Abuse and Neglect Data
System (NCANDS) project is to collect nationally standardized aggregate and case-level child
maltreatment data. This means that states must crosswalk or map their state categories to the
broader NCANDS categories and states may have multiple state categories that map to a single
NCANDS category. Although states are routinely asked to provide updated mapping as their
policies and procedures change, because NCANDS is a voluntary system and there is not a
requirement to update mapping forms.
The analyses in this chapter review the different dimensions of maltreatment type data to deter-
mine if there are any patterns within the data that may assist with targeting specic programs
or policies to aid the victims and their families. To fully consider the different dimensions,
some analyses use a duplicate count of victims, maltreatment types, or perpetrators which is
dened as:
■ Duplicate count: Counting each occurrence. For example, a duplicate count of maltreat-
ment types may count every substantiated maltreatment type every time it is reported.
NCANDS uses the following maltreatment type denitions (see Appendix B, Glossary for
these and additional denitions):
■ Medical neglect: A type of maltreatment caused by a failure of the caregiver to provide
appropriate health care of the child although nancially able to do so or offered nancial
or other resources to do so.
■ Neglect or deprivation of necessities: A type of maltreatment that refers to the failure by
the caregiver to provide needed, age-appropriate care although nancially able to do so or
offered nancial or other means to do so.
■ Physical abuse: Type of maltreatment that refers to physical acts that caused or could have
caused physical injury to a child.
■ Psychological or emotional maltreatment: Acts or omissions—other than physical abuse or
sexual abuse—that caused or could have caused—conduct, cognitive, affective, or other
behavioral or mental disorders. Frequently occurs as verbal abuse or excessive demands on
a child’s performance.
CHAPTER 7
Special Focus

Child Maltreatment 2022
chApter 7: Special Focus 94
■ Sexual abuse: A type of maltreatment that refers to the involvement of the child in sexual
activity to provide sexual gratication or nancial benet to the perpetrator, including
contacts for sexual purposes, molestation, statutory rape, prostitution, pornography,
exposure, incest, or other sexually exploitative activities.
■ Sex trafcking: A type of maltreatment that refers to the recruitment, harboring, transporta-
tion, provision, or obtaining of a person for the purpose of a commercial sex act. States have
the option to report to NCANDS any sex trafcking victim who is younger than 24 years.
■ Other: The state coding for this maltreatment type is not one of the codes in the NCANDS
record layout. According to some states’ policies and legislation, state categories of “other”
include threatened harm, threatened abuse, and threat of family violence.
Maltreatment Type Substantiations (unique count of victims)
Unfortunately, a child may be a victim of abuse and neglect more than once within a federal
scal year (FFY). Depending on state policy and procedure:
■ Some states may open a new report and conduct a new investigation or assessment of the
same incident if an allegation is received from more than one report source.
■ Some states may consolidate multiple allegations of the same incident into a single investi-
gation or assessment.
This analysis counts how many substantiations of each selected maltreatment type the victim
experienced within FFY 2022. A child is counted each time the child is determined to be
a victim of the selected maltreatment type either alone or in a combination with additional
maltreatment type(s).
Nationally, most victims are reported with a specic maltreatment type once within FFY 2022.
Victims of neglect have the most multiple substantiations with 93.2 percent of neglect victims
having a single neglect substantiation, 6.0 percent having two substantiations and fewer than
1.0 percent of victims having three substantiations. Victims of sexual abuse have the fewest
number of multiple substantiations with 97.9 percent having one sexual abuse substantiation
and 2.0 percent having two substations. See table 7–1 and related notes.
Maltreatment Type Combinations of Victims (duplicate count of victims)
Polyvictimization in child welfare refers to victims who have two or more types of maltreat-
ment. A child may be reported to NCANDS with up to four maltreatment types in each record
and a victim may have one or up to all four of those maltreatment types substantiated. The
purpose of this analysis is to display the most prevalent substantiated maltreatment type combi-
nations. Combinations are at the record level to show the result of the investigation for example:
■ If a victim has two substantiated reports, one of neglect and one of physical abuse, the
victim is counted once in neglect only and once in physical abuse only.
■ If a victim has one report with both substantiated neglect and substantiated physical abuse,
the victim is counted once in the neglect and physical abuse combination.
■ If a victim has two substantiated reports of neglect, the victim is counted twice in neglect
only.
The FFY 2022 data shows 88.6 percent of victims experience one type of substantiated mal-
treatment, although as discussed above, they could have any one type of substantiated mal-
treatment multiple times. More than three-fths of all victims are neglected only. Reviewing
state mapping for neglect reveals that the most common state categories that are mapped to

Child Maltreatment 2022
chApter 7: Special Focus 95
the NCANDS category of neglect include a state neglect category, abandonment, inadequate
supervision, and infants with prenatal substance exposure. Approximately 10 percent of victims
are physically abused only and 8.1 percent are sexually abused only.
The most common maltreatment type
combination is neglect and physical
abuse (4.2%). Neglect and psychological
maltreatment (1.7%) and neglect and
sexual abuse (1.3%) are the other
common combinations. Fewer than 1.0
percent of all victims experience three
types of substantiated maltreatment.
24
See table 7–2, exhibit 7–A, and related
notes.
Maltreatment Types and Report
Sources of Victims
(duplicate count of victims and duplicate
count of report sources)
The report source is the role of the
person who notied a CPS agency of
the alleged child abuse or neglect in a
referral. Only those sources in reports
(screened-in referrals) that receive an
investigation response or alternative
response are submitted to NCANDS.
See Chapter 2, Reports, and Appendix B, Glossary, for more information and denitions of
report sources. This table analyzes the substantiated maltreatment types of victims reported by
report source. This is different from Exhibit 2–E, Report Sources, in chapter 2 because:
■ Exhibit 2–E counts screened-in referrals (reports) while table 7–3 counts all substantiated
maltreatment types in a report.
■ Exhibit 2–E analyzes all report sources regardless of whether the report is substantiated,
unsubstantiated, etc., while table 7–3 only analyzes the report sources of victims.
For all report sources, neglect is the most common maltreatment type. Percentages range from
51.0 percent from mental health personnel to 71.7 from unclassied. For most report sources,
physical abuse is the second highest reported maltreatment type with percentages ranging
from 11.3 percent from unclassied to 30.4 percent for child daycare providers. There are two
exceptions; foster care providers and mental health personnel sources both report sexual abuse
as their second highest percentage at 18.0 and 23.7 percent, respectively.
This table also highlights the report sources that have more substantiations. As shown in exhibit
2–E, the two report sources with the highest and nearly identical percentages of referrals alleg-
ing maltreatment are education personnel (20.7%) and legal and law enforcement personnel
(21.2%.). Looking at the counts in table 7–3, legal and law enforcement personnel report more
than 2.5 times the number of substantiated maltreatment types than any other report source.
See table 7–3 and related notes.
Exhibit 7–A Children by Number of Maltreatment
Type Combinations, 2022
Fewer than 12 percent of victims have multiple
substantiated maltreatment types in the same record
Based on data from 52 states. See table 7–2.
24
The maltreatment type category called remaining combinations has fewer than 300 victims for each combination.

Child Maltreatment 2022
chApter 7: Special Focus 96
Maltreatment Types by Race and Ethnicity
(duplicate victims and duplicate maltreatment types)
Analyzing the maltreatment types of victims within race and ethnicity shows some differences
in the types of substantiated maltreatment. Within each race or ethnicity, most are victims of
neglect. Also, most races or ethnicities have physical abuse as the second highest percentage
of maltreatment. Black or African-American victims have the highest percentage of physical
abuse at 17.1 percent. The exceptions are American Indian or Alaska Native victims, which
have a high percentage (13.2%) of psychological maltreatment. Native Hawaiian or Other
Pacic Islander victims have some of the largest percentage (19.6%) of the “other” maltreatment
type.
25
Hispanic victims have similar percentages for sexual abuse 10.5 percent and physical
abuse 10.2 percent. See table 7–4, exhibit 7–B, and related notes.
Victims of Selected Maltreatment Types by Sex and Age
(unique count of victims and duplicate count of maltreatment types)
In this section the three most common maltreatment types–neglect, physical abuse, and
sexual abuse–are analyzed separately by the sex and single year age of victims. For these
analyses the victim could have the maltreatment type alone or in combination with additional
types of maltreatment.
25
There is variation in the use of the “other” maltreatment type among states. For example, Hawaii accounts for 87.8
percent of the Native Hawaiian or Other Pacic Islander victims with the “other” maltreatment type. According to
Hawaiian statutes, the state maltreatment types of threatened harm, threatened abuse, and threat of family violence are
mapped to the NCANDS category of “other” maltreatment type.
Exhibit 7–B Selected Maltreatment Types of Victims by Known Race or Ethnicity, 2022
Physical abuse is the second largest category for each race or ethnicity except Hispanic and American
Indian or Alaska Native
Based on data from 50 states. See table 7–4.

Child Maltreatment 2022
chApter 7: Special Focus 97
Victims of Neglect
Nationally, the victims of neglect are split relatively evenly between the sexes with 49.6
percent girls and 50.0 percent boys. Looking at the single year age reveals some differ-
ences between the sexes. There is a larger percentage of boys for all ages younger than
11 years ranging from <1 at 51.6 percent to 10 at 50.6 percent. Beginning at age 11, more
girls experience neglect ranging from 50.7 percent at age 11 years to 56.9 percent at age 17.
See table 7–5, exhibit 7–C, and related notes.
Victims of Physical Abuse
Nationally, there are slightly more boy victims of physical abuse at 51.5 percent than girl vic-
tims at 48.3 percent. Analyzing by single year age shows there is a larger percentage of boys for
all ages younger than 11 ranging from <1 at 53.5 percent to 53.2 percent at age 11. Beginning at
age 12, more girls are physically abused, ranging from 51.4 percent at age 12 to 60.2 percent at
age 17. See table 7–6, exhibit 7–D, and related notes.
Exhibit 7–C Victims of Neglect by Sex and Age, 2022
There are slightly more boys until age 11 when the percentage of girls becomes the majority
Based on data from 52 states. See table 7–5.

Child Maltreatment 2022
chApter 7: Special Focus 98
Victims of Psychological Maltreatment
Nationally, there are slightly more girl (52.7%) victims of psychological maltreatment than boy
(47.0%) victims. Analyzing by single-year age shows the percentage by sex uctuates until
age 10, when victims are predominately girls and steadily increase to 63.7 percent by age 17.
See table 7–7, exhibit 7–E, and related notes.
Exhibit 7–E Victims of Psychological Maltreatment by Sex and Age, 2022
Analyzing by single-year age shows the percentage by sex uctuates
until ages 10 through 17, when victims are predominately girls
Based on data from 47 states. See table 7–7.
Exhibit 7–D Victims of Physical Abuse by Sex and Age, 2022
There are slightly more boys until age 12 when the percentage of girls becomes the majority
Based on data from 52 states. See table 7–6.

Child Maltreatment 2022
chApter 7: Special Focus 99
Victims of Sexual Abuse
Nationally, most sexual abuse victims are girls, with boys comprising 16.3 percent. There is a
larger percentage of girl sexual abuse victims for all single year ages with the percentage of girl
victims steadily increasing each year. The percentages range from 55.3 percent for victims <1
to 87.4 percent for age 17. See table 7–8, exhibit 7–F, and related notes.
Maltreatment Types of Victims by Perpetrator Sex
(duplicate maltreatment types and duplicate perpetrators)
Each child in a report can have up to four different maltreatment types and up to three different
perpetrators. For this analysis, a victim is counted for each substantiated maltreatment and each
perpetrator. For example, if a victim has substantiated neglect by a female and male perpetrator,
the victim will be counted in the victim of neglect type once for the female perpetrator and
once for the male perpetrator. If a victim of neglect has two female perpetrators, the victim
will be counted twice in the female column on the neglect row in the table.
26
Percentages are
calculated against the total number of duplicate perpetrators for each maltreatment type.
Slightly more victims are maltreated by (51.9%) by female perpetrators than male perpetra-
tors (47.3%) nationally, but analyzing the maltreatment types by perpetrator sex reveals some
differences. Most victims with substantiated medical neglect have a female perpetrator at 70.5
percent, compared to 29.1 percent by a male perpetrator. More victims of neglect have female
perpetrators (58.5%) than male perpetrators (41.1%). Perpetrator sex is evenly split in victims
who are physically abused with 48.9 percent female and 49.5 percent male. Sexual abuse is
mostly perpetrated by males (88.7%) with less than 10 percent (8.4%) by female perpetrators.
More victims of the “other” maltreatment type have male perpetrators (64.9%) than female
perpetrators (34.4%). See table 7–9 and related notes.
26
Also known as a report, child, maltreatment type, perpetrator count. If a victim has more than one perpetrator, the
perpetrator may or may not be substantiated for all maltreatment types experienced by the victim.
Exhibit 7–F Victims of Sex Abuse by Sex and Age, 2022
Girls are the overwhelming majority of sex abuse victims for all ages
Based on data from 52 states. See table 7–8.

Child Maltreatment 2022
chApter 7: Special Focus 100
Conclusion
As shown in this chapter, conducting multidimensional analyses should continue to not only
deepen the child welfare eld’s understanding of the problem, but also to promote discussion
and inform policy and program decision makers about how to best support child welfare
involved families.
Exhibit and Table Notes
The following pages contain the data tables referenced in chapter 7. Specic information about
state submissions can be found in Appendix D, State Commentary. Additional information
regarding the exhibits and tables is provided below.
General
During data analyses, thresholds are set to ensure data quality is balanced with the need to
report data from as many states as possible. States may be excluded from an analysis for data
quality issues. Exclusion rules are listed in the individual table notes below. Not every table has
an exclusion rule or notes.
■ The data for all tables is from the Child File.
■ The number of victims is a duplicate count.
■ A child may have been the victim of more than one type of maltreatment, therefore, the
maltreatment type count is a duplicate count.
■ Only substantiated maltreatment types are included in this report and in this chapter each
maltreatment type is counted for each substantiation.
■ The count of victims includes children with dispositions of substantiated or indicated.
■ The row labeled Reporting States displays the count of states that provided data for that
analysis.
■ Not every state reports all maltreatment types.
■ National totals and calculations appear in a single row labeled National instead of separate
rows labeled total, rate, or percent.
■ Dashes are inserted into cells without any data.
Table 7–1 Victims by Number of Selected Maltreatment Type Substantiations,
2022
■ A child is counted in this analysis if the child is determined to be a victim of the selected
maltreatment type either alone or in a combination with additional maltreatment type(s).
Table 7–2 Maltreatment Type Combinations, 2022
■ A child may be reported with up to four maltreatment types in each record.
■ The maltreatment type category called remaining combinations has fewer than 300
victims for each combination.
■ Combinations are at the record level to show the result of the investigation.
Table 7–3 Maltreatment Types of Victims by Report Source, 2022
■ This analysis uses a duplicate count of report sources and substantiated maltreatments.
■ States with less than 85.0 percent of known report sources are excluded.
■ States with more than 20.0 percent of known report sources reported as “other” are
excluded.

Child Maltreatment 2022
chApter 7: Special Focus 101
■ One state is excluded at the state’s request for reporting errors.
■ If a child is reported twice with the same report source and substantiated maltreatments,
the child is counted both times.
■ Nonprofessional report sources are grouped into one category labeled nonprofessional and
unclassied report sources are grouped into one category labeled unclassied.
Table 7–4 Maltreatment Types of Victims by Known Race or Ethnicity, 2022
■ Counts associated with each racial group are exclusive and do not include Hispanic ethnicity.
Only those states that have both race and ethnicity population data are included in this analysis.
■ States were excluded from this analysis if more than 30.0 percent of victims were reported
without a race or ethnicity.
Table 7–5 Victims of Neglect by Sex and Age, 2022
■ Unknown gender includes not collected/not applicable, and unknown or missing.
■ Age is age at report. This means if a child has two substantiated reports, with a birthday in
between the two reports, both ages will be counted.
■ A child is counted in this analysis if the child is determined to be a victim of neglect either
alone or in combination with additional maltreatment types.
Table 7–6 Victims of Physical Abuse by Sex and Age, 2022
■ Unknown gender includes not collected/not applicable, and unknown or missing.
■ Age is age at report. This means if a child has two substantiated reports, with a birthday in
between the two reports, both ages will be counted.
■ A child is counted in this analysis if the child is determined to be a victim of physical
abuse either alone or in combination with additional maltreatment types.
Table 7–7 Victims of Psychological Maltreatment by Sex and Age, 2022
■ Unknown gender includes not collected/not applicable, and unknown or missing.
■ Age is age at report. This means if a child has two substantiated reports, with a birthday in
between the two reports, both ages will be counted.
■ A child is counted in this analysis if the child is determined to be a victim of psychological
maltreatment either alone or in combination with additional maltreatment types.
Table 7–8 Victims of Sexual Abuse by Sex and Age, 2022
■ Unknown gender includes not collected/not applicable, and unknown or missing.
■ Age is age at report. This means if a child has two substantiated reports, with a birthday in
between the two reports, both ages will be counted.
■ A child is counted in this analysis if the child is determined to be a victim of sexual abuse
either alone or in combination with additional maltreatment types.
Table 7–9 Maltreatment Types of Victims by Perpetrator Sex, 2022
■ Unknown gender includes not collected/not applicable, and unknown or missing.
■ For this analysis a victim is counted for each substantiated maltreatment and each
perpetrator.

Child Maltreatment 2022
chApter 7: Special Focus 102
Table 7–1 Victims by Number of Selected Maltreatment Type Substantiations, 2022
Maltreatment Type
Reporting
States
1
Substantiation
2
Substantiations
3
Substantiations
4 or More
Substantiations Total Victims
1
Substantiation
Percent
2
Substantiations
Percent
3
Substantiations
Percent
4 or More
Substantiations
Percent
Neglect 52 387,198 25,067 2,674 506 415,445 93.2 6.0 0.6 0.1
Physical Abuse 52 92,400 2,475 131 20 95,026 97. 2 2.6 0.1 0.0
Psychological
Maltreatment
47 36,869 1,057 86 18 38,030 96.9 2.8 0.2 0.0
Sexual Abuse 52 57,792 1,186 57 9 59,044 97.9 2.0 0.1 0.0
Table 7–2 Maltreatment Type Combinations, 2022
Maltreatment Type Combinations Maltreatment Type
Maltreatment Type
Percent
ONE TYPE -
-
Medical Neglect only 4,373 0.7
Neglect only 387,580 64.3
Other only 12,984 2.2
Physical Abuse only 59,829 9.9
Psychological Maltreatment only 18,883 3.1
Sexual Abuse only 49,086 8.1
Sex Trafcking only 755 0.1
Unknown only 343 0.1
Total One Type 533,833 88.6
TWO TYPES - -
Neglect and Medical Neglect 5,160 0.9
Neglect and Other 5,286 0.9
Neglect and Physical Abuse 25,597 4.2
Neglect and Psychological Maltreatment 10,408 1.7
Neglect and Sexual Abuse 7,534 1.3
Physical Abuse and Other 512 0.1
Physical Abuse and Psychological
Maltreatment 5,328 0.9
Physical Abuse and Sexual Abuse 1,254 0.2
Sexual Abuse and Psychological Maltreatment 468 0.1
Remaining combinations two types 1,006 0.2
Total Two Types 62,553 10.4
THREE TYPES - -
Neglect, Physical Abuse, and Psychological
Maltreatment
2,792 0.5
Physical, Neglect, and Medical Neglect 647 0.1
Neglect, Physical Abuse, and Sexual Abuse 595 0.1
Neglect, Sexual, and Psychological
Maltreatment
347 0.1
Remaining combinations three types 1,211 0.2
Total Three Types 5,592 0.9
FOUR TYPES 488 0.1
National 602,466 100.0
Based on data from 52 states.

Child Maltreatment 2022
chApter 7: Special Focus 103
Table 7–3 Maltreatment Types of Victims by Report Source, 2022 (continues below)
Maltreatment Types
Child Daycare
Providers
Education
Personnel
Foster Care
Providers
Legal and Law
Enforcement
Personnel
Medical
Personnel
Mental Health
Personnel
Social
Services
Personnel
Non-
professional Unclassied Total
Medical Neglect 31 1,948 41 1,101 3,439 383 2,053 1,292 969 11,257
Neglect 1,314 42,306 1,296 162,452 55,380 10,993 50,499 46,465 44,649 415,354
Other 53 598 14 7,849 1,243 208 1,463 1,240 815 13,483
Physical Abuse 710 14,541 405 30,265 16,293 2,994 10,541 9,868 7,005 92,622
Psychological Maltreatment
88 4,415 111 16,278 2,228 1,810 4,103 4,931 4,172 38,136
Sexual Abuse 139 8,253 416 19,397 4,886 5,101 6,921 6,190 4,527 55,830
Sex Trafcking 2 105 21 426 90 57 271 58 101 1,131
Unknown 1 23 1 69 84 - 58 94 23 353
National 2,338 72,189 2,305 237,837 83,643 21,546 75,909 70,138 62,261 628,166
Based on data from 48 states.
Table 7–3 Maltreatment Types of Victims by Report Source, 2022
Maltreatment Types
Child Daycare
Providers
Percent
Education
Personnel
Percent
Foster Care
Providers
Percent
Legal and Law
Enforcement
Personnel
Percent
Medical
Personnel
Percent
Mental Health
Personnel
Percent
Social
Services
Personnel
Percent
Non-
professional
Percent
Unclassied
Percent Total Percent
Medical Neglect 1.3 2.7 1.8 0.5 4.1 1.8 2.7 1.8 1.6 1.8
Neglect 56.2 58.6 56.2 68.3 66.2 51.0 66.5 66.2 71.7 66.1
Other 2.3 0.8 0.6 3.3 1.5 1.0 1.9 1.8 1.3 2.1
Physical Abuse 30.4 20.1 17.6 12.7 19.5 13.9 13.9 14.1 11.3 14.7
Psychological Maltreatment
3.8 6.1 4.8 6.8 2.7 8.4 5.4 7.0 6.7 6.1
Sexual Abuse 5.9 11.4 18.0 8.2 5.8 23.7 9.1 8.8 7.3 8.9
Sex Trafcking 0.1 0.1 0.9 0.2 0.1 0.3 0.4 0.1 0.2 0.2
Unknown 0.0 0.0 0.0 - 0.1 0.0 0.1 0.1 0.0 0.1
National 100.0 100.0 100.0 100.0 100.0 100.0 100.0 100.0 100.0 100.0
Based on data from 48 states.

Child Maltreatment 2022
Chapter 7: Special Focus 104
Table 7–4 Maltreatment Types of Victims by Known Race or Ethnicity, 2022 (continues below)
Race or Ethnicity Medical Neglect Neglect Other Physical Abuse
Psychological
Maltreatment Sexual Abuse Sex Trafcking Unknown
Total
Maltreatment
Typ es
American Indian or Alaska Native 110 7,148 145 908 1,326 427 7 3 10,074
Asian 103 4,310 157 783 265 634 10 1 6,263
Black or African-American 3,052 94,542 4,160 24,088 5,912 8,606 239 131 140,730
Hispanic 2,097 109,542 3,160 15,764 7,912 16,212 207 45 154,939
Two or More Races 625 26,444 1,455 5,867 2,934 2,382 56 12 39,775
Native Hawaiian or Other
Pacic Islander
20 820 370 288 213 171 1 - 1,883
White 4,408 181,934 8,139 41,941 16,599 26,492 416 150 280,079
National 10,415 424,740 17,586 89,639 35,161 54,924 936 342 633,743
Based on data from 50 states.
Table 7–5 Victims of Neglect by Sex and Age, 2022
Age Boys Girls Unknown
Total Duplicate
Victims
Boys Percent
Age
Girls Percent
Age
Unknown
Percent Age
<1 36,939 34,374 309 71,622 51.6 48.0 0.4
1 17,15 8 15,697 127 32,982 52.0 47.6 0.4
2 16,555 14,869 141 31,565 52.4 47.1 0.4
3 15,480 14,009 110 29,599 52.3 47.3 0.4
4 14,169 12,863 79 27,111 52.3 47.4 0.3
5 13,591 12,551 91 26,233 51.8 47.8 0.3
6 13,417 12,007 68 25,492 52.6 47.1 0.3
7 12,349 11,457 88 23,894 51.7 47.9 0.4
8 11,326 10,879 51 22,256 50.9 48.9 0.2
9 10,603 10,251 53 20,907 50.7 49.0 0.3
10 10,010 9,736 50 19,796 50.6 49.2 0.3
11 9,222 9,523 48 18,793 49.1 50.7 0.3
12 9,166 9,933 40 19,139 47.9 51.9 0.2
13 8,412 10,365 44 18,821 44.7 55.1 0.2
14 7,803 10,262 34 18,099 43.1 56.7 0.2
15 7,157
9,494 27 16,678 42.9
56.9 0.2
16 6,050 8,036 30 14,116 42.9 56.9 0.2
17 3,919 5,215 37 9,171 42.7 56.9 0.4
18 and older, unborn,
unknown
606 535 69 1,210 50.1 44.2 5.7
National 223,932 222,056 1,496 447,484 50.0 49.6 0.3
Based on data from 52 states.
Table 7–4 Maltreatment Types of Victims by Known Race or Ethnicity, 2022
Race or Ethnicity
Medical Neglect
Percent Neglect Percent Other Percent
Physical Abuse
Percent
Psychological
Maltreatment
Percent
Sexual Abuse
Percent
Sex Trafcking
Percent
Unknown
Percent
Total
Maltreatment
Typ es
American Indian or Alaska Native 1.1 71.0 1.4 9.0 13.2 4.2 0.1 0.0 100.0
Asian 1.6 68.8 2.5 12.5 4.2 10.1 0.2 0.0 100.0
Black or African-American 2.2 67.2 3.0 17.1 4.2 6.1 0.2 0.1 100.0
Hispanic 1.4 70.7 2.0 10.2 5.1 10.5 0.1 0.0 100.0
Two or More Races 1.6 66.5 3.7 14.8 7.4 6.0 0.1 0.0 100.0
Native Hawaiian or Other
Pacic Islander
1.1 43.5 19.6 15.3 11.3 9.1 0.1 0.0 100.0
White 1.6 65.0 2.9 15.0 5.9 9.5 0.1 0.1 100.0
National 1.6 67.0 2.8 14.1 5.5 8.7 0.1 0.1 100.0
Based on data from 50 states.

Child Maltreatment 2022
chApter 7: Special Focus 105
Table 7–6 Victims of Physical Abuse by Sex and Age, 2022
Age Boys Girls Unknown
Total Duplicate
Victims
Boys Percent
Age
Girls Percent
Age
Unknown
Percent Age
<1 8,205 7,095 34 15,334 53.5 46.3 0.2
1 2,810 2,338 15 5,16 3 54.4 45.3 0.3
2 2,615 2,128 26 4,769 54.8 44.6 0.5
3 2,629 2,171 14 4,814 54.6 45.1 0.3
4 2,727 2,028 6 4,761 57.3 42.6 0.1
5 2,918 2,221 5 5,144 56.7 43.2 0.1
6 3,051 2,145 14 5,210 58.6 41.2 0.3
7 2,829 2,095 11 4,935 57.3 42.5 0.2
8 2,663 2,044 15 4,722 56.4 43.3 0.3
9 2,551 2,051 16 4,618 55.2 44.4 0.3
10 2,455 1,953 5 4,413 55.6 44.3 0.1
11 2,405 2,110 5 4,520 53.2 46.7 0.1
12 2,389 2,535 12 4,936 48.4 51.4 0.2
13 2,447 3,017 5 5,469 44.7 55.2 0.1
14 2,238 3,292 15 5,545 40.4 59.4 0.3
15 2,128
3,212 7 5,347
39.8 60.1 0.1
16 1,872 2,691 12 4,575 40.9 58.8 0.3
17 1,282 1,951 9 3,242 39.5 60.2 0.3
18 and older, unborn,
unknown age
159 126 23 308 51.6 40.9 7.5
National 50,373 47,203 249 97,825 51.5 48.3 0.3
Based on data from 52 states.
Table 7–7 Victims of Psychological Maltreatment by Sex and Age, 2022
Age Boys Girls Unknown
Total Duplicate
Victims
Boys Percent
Age
Girls Percent
Age
Unknown
Percent Age
<1 1,452 1,456 - 2,917 49.8 49.9 -
1 1,218 1,15 8 7 2,383 51.1 48.6 0.3
2 1,162 1,129 - 2,300 50.5 49.1 -
3 1,083 1,134 4 2,221 48.8 51.1 0.2
4 1,164 1,114 3 2,281 51.0 48.8 0.1
5 1,147 1,149 3 2,299 49.9 50.0 0.1
6 1,226 1,097 6 2,329 52.6 47.1 0.3
7 1,179 1,165 7 2,351 50.1 49.6 0.3
8 1,169 1,139 3 2,311 50.6 49.3 0.1
9 1,091 1,120 3 2,214 49.3 50.6 0.1
10 1,027 1,129 3 2,159 47.6 52.3 0.1
11 1,078 1,155 4 2,237 48.2 51.6 0.2
12 957 1,221 6 2,184 43.8 55.9 0.3
13 890 1,304 2 2,196 40.5 59.4 0.1
14 855 1,264 6 2,125 40.2 59.5 0.3
15
727 1,172 7 1,906
38.1 61.5 0.4
16 652 1,108 7 1,767 36.9 62.7 0.4
17 379 669 2 1,050 36.1 63.7 0.2
18 and older, unborn,
and unknown
43 46 4 93 46.2 49.5 4.3
National 18,499 20,729 95 39,323 47.0 52.7 0.2

Child Maltreatment 2022
Chapter 7: Special Focus 106
Table 7–9 Maltreatment Types of Victims by Perpetrator Sex, 2022
Maltreatment Type Female Male Unknown Total
Female
Percent Total Percent
Unclassied
Percent
Total Report
Sources
Percent
Medical Neglect 9,575 3,960 54 13,589 70.5 29.1 0.4 100.0
Neglect 317,821 223,285 2,149 543,255 58.5 41.1 0.4 100.0
Other 7,732 14,572 143 22,447 34.4 64.9 0.6 100.0
Physical Abuse 52,842 53,537 1,715 108,094 48.9 49.5 1.6 100.0
Psychological or Emotional
Maltreatment
17,354 24,969 111 42,434 40.9 58.8 0.3 100.0
Sexual Abuse 5,095 53,513 1,738 60,346 8.4 88.7 2.9 100.0
Sex Trafcking 144 541 351 1,036 13.9 52.2 33.9 100.0
Unknown 24 24 1 49 49.0 49.0 2.0 100.0
National 410,587 374,401 6,262 791,250 51.9 47.3 0.8 100.0
Based on data from 50 states.
Table 7–8 Victims of Sexual Abuse by Sex and Age, 2022
Age Boys Girls Unknown
Total Duplicate
Victims
Girls Percent
Age
Boys
Percent
Age
U
nknown
Percent Age
<1 135 167 - 302 55.3 44.7 -
1 143 182 3 328 55.5 43.6 0.9
2 197 297 - 494 60.1 39.9 -
3 324 737 5 1,066 69.1 30.4 0.5
4 470 1,213 5 1,688 71.9 27.8 0.3
5 578 1,422 3 2,003 71.0 28.9 0.1
6 686 1,591 7 2,284 69.7 30.0 0.3
7 700 1,711 4 2,415 70.8 29.0 0.2
8 720 1,911 17 2,648 72.2 27.2 0.6
9 650 2,397 8 3,055 78.5 21.3 0.3
10 641 3,070 13 3,724 82.4 17.2 0.3
11 658 4,078 19 4,755 85.8 13.8 0.4
12 687 5,114 19 5,820 87.9 11.8 0.3
13 701 6,089 22 6,812 89.4 10.3 0.3
14 713 6,160 19 6,892 89.4 10.3 0.3
15
710 5,997 20 6,727 89.1 10.6 0.3
16 607 4,698 15 5,320
88.3 1
1.4 0.3
17 466 3,286 8 3,760 87.4 12.4 0.2
18 and older, unborn,
unknown age
59 214 5 278 77.0 21.2 1.8
National 9,845 50,334 192 60,371 83.4 16.3 0.3
Based on data from 52 states.

Appendixes
107
Child Maltreatment 2022
Appendixes

1
The items listed under number (10), (13), and (14) are not collected by NCANDS. Items (17) and (18) were enacted with the
Justice for Victims of Trafcking Act of 2015 (P.L. 114–22) and The Comprehensive Addiction and Recovery Act (CARA) of
2016 (P.L. 114–198). States began reporting these items with FFY 2018 data.
CAPTA Data Items
The Child Abuse Prevention and Treatment Act (CAPTA), as amended by P.L. 111–320,
the CAPTA Reauthorization Act of 2010, afrms, “Each State to which a grant is made
under this section shall annually work with the Secretary to provide, to the maximum
extent practicable, a report that includes the following:”
1
1) The number of children who were reported to the state during the year as victims
of child abuse or neglect.
2) Of the number of children described in paragraph (1), the number with respect to
whom such reports were—
a) Substantiated;
b) Unsubstantiated; or
c) Determined to be false.
3) 3) Of the number of children described in paragraph (2)—
a) the number that did not receive services during the year under the state
program funded under this section or an equivalent state program;
b) the number that received services during the year under the state program
funded under this section or an equivalent state program; and
c) the number that were removed from their families during the year by disposi-
tion of the case.
4) The number of families that received preventive services, including use of dif-
ferential response, from the state during the year.
5) The number of deaths in the state during the year resulting from child abuse or
neglect.
6) Of the number of children described in paragraph (5), the number of such
children who were in foster care.
7)
a) The number of child protective service personnel responsible for the—
i.) intake of reports led in the previous year;
ii.) screening of such reports;
iii.) assessment of such reports; and
iv.) investigation of such reports.
b) The average caseload for the workers described in subparagraph (A).
8) The agency response time with respect to each such report with respect to initial
investigation of reports of child abuse or neglect.
9) The response time with respect to the provision of services to families and
children where an allegation of child abuse or neglect has been made.
APPENDIX A
Appendix A: CAPTA Data Items 108
Child Maltreatment 2022

10) For child protective service personnel responsible for intake, screening, assess-
ment, and investigation of child abuse and neglect reports in the state—
a) information on the education, qualications, and training requirements
established by the state for child protective service professionals, including
for entry and advancement in the profession, including advancement to
supervisory positions;
b) data of the education, qualications, and training of such personnel;
c) demographic information of the child protective service personnel; and
d) information on caseload or workload requirements for such personnel,
including requirements for average number and maximum number of cases
per child protective service worker and supervisor.
11) The number of children reunited with their families or receiving family preserva-
tion services that, within ve years, result in subsequent substantiated reports of
child abuse or neglect, including the death of the child.
12) The number of children for whom individuals were appointed by the court to
represent the best interests of such children and the average number of out of
court contacts between such individuals and children.
13) The annual report containing the summary of activities of the citizen review
panels of the state required by subsection (c)(6).
14) The number of children under the care of the state child protection system who
are transferred into the custody of the state juvenile justice system.
15) The number of children referred to a child protective services system under
subsection (b)(2)(B)(ii).
16) The number of children determined to be eligible for referral, and the number
of children referred, under subsection (b)(2)(B)(xxi), to agencies providing early
intervention services under part C of the Individuals with Disabilities Education
Act (20 U.S.C. 1431 et seq.).
17) The number of children determined to be victims described in subsection (b) (2)
(B)(xxiv).
18) The number of infants—
a) identied under subsection (b)(2)(B)(ii);
b) for whom a plan of safe care was developed under subsection (b)(2)(B) (iii);
and
c) for whom a referral was made for appropriate services, including services for
the affected family or caregiver, under subsection (b)(2)(B) (iii).
Appendix A: CAPTA Data Items 109
Child Maltreatment 2022

Glossary
Acronyms
AFCARS: Adoption and Foster Care Analysis and Reporting System
AFCARS ID: Adoption and Foster Care Analysis and Reporting System identier
CAPTA: Child Abuse Prevention and Treatment Act
CARA: Comprehensive Addiction and Recovery Act
CASA: Court Appointed Special Advocate
CBCAP: Community-Based Child Abuse Prevention
CFSR: Child and Family Services Reviews
CHILD ID: Child identier
CPS: Child protective services
FFY: Federal scal year
FIPS: Federal Information Processing Standards
FTE: Full-time equivalent
GAL: Guardian ad litem
IDEA: Individuals with Disabilities Education Act
IPSE: Infants with prenatal substance exposure
NCANDS: National Child Abuse and Neglect Data System
NYTD: National Youth in Transition Database
MIECHV: Maternal, Infant, and Early Childhood Home Visiting
OMB: Ofce of Management and Budget
PERPETRATOR ID: Perpetrator identier
PSSF: Promoting Safe and Stable Families
REPORT ID: Report identier
SDC: Summary data component
SSBG: Social Services Block Grant
TANF: Temporary Assistance for Needy Families
WORKER ID: Worker identier
APPENDIX B
Appendix B: Glossary 110
Child Maltreatment 2022

Denitions
ADOPTION AND FOSTER CARE ANALYSIS AND REPORTING SYSTEM
(AFCARS): The federal collection of case-level information on all children in foster care
for whom state child welfare agencies have responsibility for placement, care, or supervision
and on children who are adopted under the auspices of the state’s public child welfare agency.
AFCARS also includes information on foster and adoptive parents.
ADOPTION SERVICES: Activities to assist with bringing about the adoption of a child.
ADOPTIVE PARENT: A person who become the permanent parent through adoption, with
all of the social, legal rights and responsibilities of any parent.
AFCARS ID: The record number used in the AFCARS data submission or the value that
would be assigned.
AGE: A number representing the years that the child or perpetrator had been alive at the
time of the alleged maltreatment.
AGENCY FILE: A data le submitted by a state to NCANDS on an annual basis. The le
contains supplemental aggregated child abuse and neglect data from such agencies as medi-
cal examiners’ ofces and non-CPS services providers.
ALCOHOL ABUSE: Compulsive use of alcohol that is not of a temporary nature. This
risk factor can be applied to a caregiver or a child. If applied to a child, it can include Fetal
Alcohol Syndrome and exposure to alcohol during pregnancy.
ALLEGED PERPETRATOR: An individual who is named in a referral to have caused or
knowingly allowed the maltreatment of a child.
ALLEGED MALTREATMENT: Suspected child abuse and neglect. In NCANDS, such
suspicions are included in a referral to a CPS agency.
ALLEGED VICTIM: Child about whom a referral regarding maltreatment was made to a
CPS agency.
ALLEGED VICTIM REPORT SOURCE: A child who alleges to have been a victim of
child maltreatment and who makes a CPS referral of the allegation. Only referrals that were
screened-in (and become reports) for an investigation or assessment have report sources.
ALTERNATIVE RESPONSE: The provision of a response other than an investigation that
determines a child or family is in need of services. A determination of maltreatment is not
made and a perpetrator is not determined. States may report the disposition as alternative
response victim or alternative response nonvictim, however, in this report the categories are
combined.
Appendix B: Glossary 111
Child Maltreatment 2022

AMERICAN INDIAN or ALASKA NATIVE: A person having origins in any of the
original peoples of North and South America (including Central America), and who main-
tains tribal afliation or community attachment. Race may be self-identied or identied by
a caregiver.
ANONYMOUS REPORT SOURCE: An individual who noties a CPS agency of sus-
pected child maltreatment without identifying himself or herself.
ASIAN: A person having origins in any of the original peoples of the Far East, Southeast
Asia, or the Indian subcontinent, including, for example, Cambodia, China, India, Japan,
Korea, Malaysia, Pakistan, the Philippine Islands, Thailand, and Vietnam. Race may be
self-identied or identied by a caregiver.
ASSESSMENT: A process by which the CPS agency determines whether the child or other
persons involved in the report of alleged maltreatment is in need of services. When used as
an alternative to an investigation, it is a process designed to gain a greater understanding
about family strengths, needs, and resources.
BEHAVIOR PROBLEM, CHILD: A child’s behavior in the school or community that
adversely affects socialization, learning, growth, and moral development. This risk factor
may include adjudicated or nonadjudicated behavior problems such as running away from
home or a placement.
BIOLOGICAL PARENT: The birth mother or father of the child.
BLACK or AFRICAN-AMERICAN: A person having origins in any of the Black racial
groups of Africa. Race may be self-identied or identied by a caregiver.
BOY: A male child younger than 18 years.
CAREGIVER: A person responsible for the care and supervision of a child.
CAREGIVER RISK FACTOR: A caregiver’s characteristic, disability, problem, or environ-
ment, which could tend to decrease the ability to provide adequate care for a child.
CASE-LEVEL DATA: States submit case-level data by constructing an electronic le of
child-specic records for each report of alleged child abuse and neglect that received a CPS
response. Only completed reports that resulted in a disposition (or nding) as an outcome of
the CPS response during the reporting year, are submitted in each state’s data le. The data
submission containing these case-level data is called the Child File.
CASELOAD: The number of CPS responses (cases) handled by workers.
CASE MANAGEMENT SERVICES: Activities for the arrangement, coordination, and
monitoring of services to meet the needs of children and their families.
CHILD: A person who has not attained the lesser of (a) the age of 18 or (b) the age specied
by the child protection law of the state in which the child resides. For sex trafcking victims
only, a state may dene a child as a person who has not attained the age of 24.
Appendix B: Glossary 112
Child Maltreatment 2022

CHILD ABUSE AND NEGLECT STATE GRANT: Funding to the states for programs
serving abused and neglected children, awarded under the Child Abuse Prevention and
Treatment Act (CAPTA). May be used to assist states with intake and assessment, screening
and investigation of child abuse and neglect reports, improving risk and safety assessment
protocols, training child protective service workers and mandated reporters, and improving
services to disabled infants with life-threatening conditions.
CHILD ABUSE PREVENTION AND TREATMENT ACT (CAPTA) (42 U.S.C. 5101
et seq): The key federal legislation addressing child abuse and neglect, which was origi-
nally enacted on January 31, 1974 (P.L. 93–247). CAPTA has been reauthorized and amended
several times, most recently on December 20, 2010, by the CAPTA Reauthorization Act of
2010 (P.L. 111–320). CAPTA provides federal funding to states in support of prevention,
assessment, investigation, prosecution, and treatment activities for child abuse and neglect.
It also provides grants to public agencies and nonprot organizations, including Tribes,
for demonstration programs and projects; and the federal support for research, evaluation,
technical assistance, and data collection activities.
CHILD AND FAMILY SERVICES REVIEWS (CFSR): The 1994 Amendments to the
Social Security Act (SSA) authorized the U.S. Department of Health and Human Services
(HHS) to review state child and family service programs to ensure conformity with the
requirements in titles IV–B and IV–E of the SSA. Under a nal rule, which became effective
March 25, 2000, states are assessed for substantial conformity with certain federal require-
ments for child protective, foster care, adoption, family preservation and family support, and
independent living services.
CHILD DAYCARE PROVIDER: A person with a temporary caregiver responsibility, but
who is not related to the child, such as a daycare center staff member, family provider, or
babysitter. Does not include persons with legal custody or guardianship of the child.
CHILD DISPOSITION: A determination made by a social service agency that evidence is
or is not sufcient under state law to conclude that maltreatment occurred. A disposition is
applied to each child within a report.
CHILD DEATH REVIEW TEAM: A state or local team of professionals who review all or a
sample of cases of children who are alleged to have died due to maltreatment or other causes.
CHILD FILE: A data le submitted by a state to NCANDS. The le contains child-specic
records for each report of alleged child abuse and neglect that received a CPS response. Only
completed reports that resulted in a disposition (or nding) as an outcome of the CPS response
during the reporting year, are submitted in each state’s data le.
CHILD IDENTIFIER (Child ID): A unique identication assigned to each child. This
identication is not the state’s child identication but is an encrypted identication assigned
by the state for the purposes of the NCANDS data collection.
CHILD MALTREATMENT: The Child Abuse Prevention and Treatment Act (CAPTA) deni-
tion of child abuse and neglect is, at a minimum: Any recent act or failure to act on the part of a
parent or caretaker which results in death, serious physical or emotional harm, sexual abuse or
exploitation; or an act or failure to act, which presents an imminent risk of serious harm.
Appendix B: Glossary 113
Child Maltreatment 2022

CHILD PROTECTIVE SERVICES (CPS) AGENCY: An ofcial state agency having
the responsibility to receive and respond to allegations of suspected child abuse and neglect,
determine the validity of the allegations, and provide services to protect and serve children
and their families.
CHILD PROTECTIVE SERVICES (CPS) RESPONSE: CPS agencies conduct a
response for all reports of child maltreatment. The response may be an investigation, which
determines whether a child was maltreated or is at-risk of maltreatment and establishes
if an intervention is needed. The majority of reports receive investigations. A small, but
growing, number of reports receive an alternative response, which focuses primarily upon
the needs of the family and usually does not include a determination regarding the alleged
maltreatment(s).
CHILD PROTECTIVE SERVICES (CPS) SUPERVISOR: The manager of the case-
worker assigned to a report of child maltreatment at the time of the report disposition.
CHILD PROTECTIVE SERVICES (CPS) WORKER: The person assigned to a report of
child maltreatment at the time of the report disposition.
CHILD RECORD: A case-level record in the Child File containing the data associated with
one child.
CHILD RISK FACTOR: A child’s characteristic, disability, problem, or environment that
may affect the child’s safety.
CHILD VICTIM: A child for whom the state determined at least one maltreatment was
substantiated or indicated. This includes a child who died of child abuse and neglect. This
is a change from prior years when children with dispositions of alternative response victim
were included as victims. It is important to note that a child may be a victim in one report
and a nonvictim in another report.
CHILDREN’S BUREAU: The Children’s Bureau partners with federal, state, tribal, and
local agencies to improve the overall health and well-being of our nation’s children and
families. It is the federal agency responsible for the collection and analysis of NCANDS data.
CLOSED WITH NO FINDING: A disposition that does not conclude with a specic nding
because the CPS response could not be completed.
COMMUNITY-BASED CHILD ABUSE PREVENTION PROGRAM (CBCAP):
This program provides funding to states to develop, operate, expand, and enhance commu-
nity-based, prevention-focused programs and activities designed to strengthen and support
families to prevent child abuse and neglect. The program was reauthorized, amended, and
renamed as part of the CAPTA amendments in 2010. To receive these funds, the Governor
must designate a lead agency to receive the funds and implement the program.
COMPREHENSIVE ADDICTION AND RECOVERY ACT (CARA): Amended the Child
Abuse Prevention and Treatment Act in sections 106(b)(2)(B)(ii) and (iii) and by adding new
state reporting requirements to Section 106(d).
Appendix B: Glossary 114
Child Maltreatment 2022

COUNSELING SERVICES: Activities that apply therapeutic processes to individual,
family, situational, or occupational problems to resolve the problem or improve individual or
family functioning or circumstances.
COUNTY OF REPORT: The jurisdiction to which the report of alleged child maltreatment
was assigned for a CPS response.
COUNTY OF RESIDENCE: The jurisdiction in which the child was residing at the time of
the report of maltreatment.
COURT-APPOINTED REPRESENTATIVE: A person appointed by the court to represent
a child in an abuse and neglect proceeding and is often referred to as a guardian ad litem
(GAL). The representative makes recommendations to the court concerning the best interests
of the child.
COURT-APPOINTED SPECIAL ADVOCATE (CASA): Adult volunteers trained to
advocate for abused and neglected children who are involved in the juvenile court.
COURT ACTION: Legal action initiated by a representative of the CPS agency on behalf
of the child. This includes authorization to place the child in foster care, ling for temporary
custody, dependency, or termination of parental rights. It does not include criminal proceed-
ings against a perpetrator.
DAYCARE SERVICES: Activities provided to a child or children in a setting that meets
applicable standards of state and local law, in a center or home, for a portion of a 24-hour
day.
DISABILITY: A child is considered to have a disability if one of more of the following
risk factors has been identied or clinically diagnosed: child has a/an intellectual disability,
emotional disturbance, visual or hearing impairment, learning disability, physical disability,
behavior problem, or some other medical condition. In general, children with such conditions
are undercounted as not every child receives a clinical diagnostic assessment.
DISPOSITION: A determination made by a CPS agency that evidence is or is not sufcient
under state law to conclude that maltreatment occurred. A disposition is applied to each
alleged maltreatment in a report and to the report itself.
DOMESTIC VIOLENCE: Any abusive, violent, coercive, forceful, or threatening act or
word inicted by one member of a family or household on another. This risk factor can be
applied to a caregiver. In NCANDS, the caregiver may be the perpetrator or the victim of the
domestic violence.
DRUG ABUSE: The compulsive use of drugs that is not of a temporary nature. This risk
factor can be applied to a caregiver or a child. If applied to a child, it can include infants
exposed to drugs during pregnancy.
DUPLICATE COUNT OF CHILDREN: Counting a child each time he or she was the
subject of a report. This count also is called a report-child pair.
Appendix B: Glossary 115
Child Maltreatment 2022

DUPLICATED COUNT OF PERPETRATORS: Counting a perpetrator each time the
perpetrator is associated with maltreating a child. This also is known as a report-child-perpe-
trator triad. For example, a perpetrator would be counted twice in the following situations: (1)
one child in two separate reports, (2) two children in a single report, and (3) two children in
two separate reports.
EDUCATION AND TRAINING SERVICES: Services provided to improve knowledge or
capacity of a given skill set, in a particular subject matter, or in personal or human develop-
ment. Services may include instruction or training in, but are not limited to, such issues as
consumer education, health education, community protection and safety education, literacy
education, English as a second language, and General Educational Development (G.E.D.).
Component services or activities may include screening, assessment, and testing; individual
or group instruction; tutoring; provision of books, supplies and instructional material;
counseling; transportation; and referral to community resources.
EDUCATION PERSONNEL: Employees of a public or private educational institution or
program; includes teachers, teacher assistants, administrators, and others directly associated
with the delivery of educational services.
EMOTIONAL DISTURBANCE: A clinically diagnosed condition exhibiting one or more of
the following characteristics over a long period of time and to a marked degree: an inability to
build or maintain satisfactory interpersonal relationships; inappropriate types of behavior or
feelings under normal circumstances; a general pervasive mood of unhappiness or depression;
or a tendency to develop physical symptoms or fears associated with personal problems. The
diagnosis is based on the Diagnostic and Statistical Manual of Mental Disorders. This risk
factor includes schizophrenia and autism and can be applied to a child or a caregiver.
EMPLOYMENT SERVICES: Activities provided to assist individuals in securing employ-
ment or the acquiring of skills that promote opportunities for employment.
FA M ILY: A group of two or more persons related by birth, marriage, adoption, or emotional ties.
FAMILY PRESERVATION SERVICES: Services for children and families designed to
help families at risk or in crisis. This includes service programs designed to help children
return to families, be placed for adoption, or be placed in some other planned, permanent
living arrangement. Services also include preplacement preventive services programs, such
as intensive family preservation programs, designed to help children at risk of foster care
placement remain safely with their families; service programs designed to provide followup
care to families to whom a child has been returned after a foster care placement; respite care
of children to provide temporary relief for caregivers; services designed to improve parenting
skills; and infant safe haven programs.
FAMILY REUNIFICATION SERVICES: Services and activities that are provided to a
child that is removed from the child’s home and placed in a foster family home or a child care
institution or a child who has been returned home and to the parents or primary caregiver of
such a child, in order to facilitate the reunication of the child safely and appropriately within
a timely fashion and to ensure the strength and stability of the reunication. In the case of a
child who has been returned home, the services and activities shall only be provided during
the 15-month period that begins on the date that the child returns home. These services
Appendix B: Glossary 116
Child Maltreatment 2022

include: individual, group, and family counseling; inpatient, residential, or outpatient
substance abuse treatment services; mental health services; assistance to address domestic
violence, services designed to provide temporary child care and therapeutic services for
families, including crisis nurseries; peer-to-peer mentoring and support groups for parents
and primary caregivers; services and activities designed to facilitate access to and visitation
of children by parents and siblings; and transportation to or from any of these services and
activities.
FAMILY SUPPORT SERVICES: Community-based services designed to carry out
purposes including: promoting the safety and well-being of children and families; increasing
the strength and stability of families; supporting and retaining foster families; to increase
parents’ condence and competence in their parenting abilities; to afford children a safe,
stable, and supportive family environment; to strengthen parental relationships and promote
healthy marriages; and to enhance child development.
FATALITY: Death of a child as a result of abuse and neglect, because either an injury result-
ing from the abuse and neglect was the cause of death, or abuse and neglect were contribut-
ing factors to the cause of death.
FEDERAL FISCAL YEAR (FFY): The 12-month period from October 1 through
September 30 used by the federal government. The scal year is designated by the calendar
year in which it ends.
FEDERAL INFORMATION PROCESSING STANDARDS (FIPS): The federally
dened set of county codes for all states.
FINDING: See DISPOSITION.
FETAL ALCOHOL SPECTRUM DISORDERS: Scientists dene a broad range of effects
and symptoms caused by prenatal alcohol exposure under the umbrella term Fetal Alcohol
Spectrum Disorders (FASD). The medical disorders collectively labeled FASD include
the Institute of Medicine of the National Academies (IOM) diagnostic categories of Fetal
Alcohol Syndrome, Partial Fetal Alcohol Syndrome, Alcohol-Related Neurodevelopmental
Disorder, and Alcohol-Related Birth Defects. The Diagnostic and Statistical Manual of
Mental Disorders (DSM–5) also includes Neurobehavioral Disorder Associated with Prenatal
Alcohol Exposure. https://www.niaaa.nih.gov/publications/brochures-and-fact-sheets/
understanding-fetal-alcohol-spectrum-disorders
FINANCIAL PROBLEM: A risk factor related to the family’s inability to provide sufficient
financial resources to meet minimum needs.
FOSTER CARE: Twenty-four-hour substitute care for children placed away from their
parents or guardians and for whom the state agency has placement and care responsibility.
This includes family foster homes, group homes, emergency shelters, residential facilities,
childcare institutions, etc. The NCANDS category applies regardless of whether the facil-ity
is licensed and whether payments are made by the state or local agency for the care of the
child, or whether there is federal matching of any payments made. Foster care may be
provided by those related or not related to the child. All children in care for more than 24
hours are counted.
Appendix B: Glossary 117
Child Maltreatment 2022

FOSTER PARENT: Individual who provides a home for orphaned, abused, neglected,
delinquent, or disabled children under the placement, care, or supervision of the state. The
person may be a relative or nonrelative and need not be licensed by the state agency to be
considered a foster parent.
FRIEND: A nonrelative acquainted with the child, the parent, or caregiver.
FULL-TIME EQUIVALENT (FTE): A computed statistic representing the number of full-
time employees if the number of hours worked by part-time employees had been worked by
full-time employees.
GIRL: A female child younger than 18 years.
GROUP HOME OR RESIDENTIAL CARE: A nonfamilial 24-hour care facility that may
be supervised by the state agency or governed privately.
GROUP HOME STAFF: Employee of a nonfamilial 24-hour care facility.
GUARDIAN AD LITEM (GAL): See COURT-APPOINTED REPRESENTATIVE.
HEALTH-RELATED AND HOME HEALTH SERVICES: Activities provided to attain
and maintain a favorable condition of health.
HISPANIC ETHNICITY: A person of Cuban, Mexican, Puerto Rican, South or Central
American, or other Spanish culture or origin, regardless of race. See RACE.
HOME-BASED SERVICES: In-home activities provided to individuals or families to
assist with household or personal care that improve or maintain family well-being. Includes
homemaker, chore, home maintenance, and household management services.
HOUSING SERVICES: Activities designed to assist individuals or families to locate,
obtain, or retain suitable housing.
INADEQUATE HOUSING: A risk factor related to substandard, overcrowded, or unsafe
housing conditions, including homelessness.
INCIDENT DATE: The month, day, and year of the most recent, known incident of alleged
child maltreatment.
INDEPENDENT AND TRANSITIONAL LIVING SERVICES: Activities designed to
help older youth in foster care or homeless youth make the transition to independent living.
INDIVIDUALS WITH DISABILITIES EDUCATION IMPROVEMENT ACT: A law
ensuring services to children with disabilities throughout the nation.
INFORMATION AND REFERRAL SERVICES: Resources or activities that provide facts
about services that are available from public and private providers. The facts are provided
after an assessment (not a clinical diagnosis or evaluation) of client needs.
Appendix B: Glossary 118
Child Maltreatment 2022

INDICATED OR REASON TO SUSPECT: A disposition that concludes that maltreatment
could not be substantiated under state law or policy, but there was a reason to suspect that
a child may have been maltreated or was at-risk of maltreatment. This is applicable only to
states that distinguish between substantiated and indicated dispositions.
INFANTS WITH PRENATAL SUBSTANCE EXPOSURE (IPSE): Infants born with
and identied as being affected by substance abuse or withdrawal symptoms resulting from
prenatal drug exposure, or a Fetal Alcohol Spectrum Disorder, including a requirement that
health care providers involved in the delivery or care of such infants notify the child protec-
tive services system of the occurrence of such condition of such infants.
IN-HOME SERVICES: Any service provided to the family while the child’s residence is in
the home. Services may be provided directly in the child’s home or a professional setting.
INTAKE: The activities associated with the receipt of a referral and the decision of whether
to accept it for a CPS response.
INTELLECTUAL DISABILITY: A clinically diagnosed condition of reduced general
cognitive and motor functioning existing concurrently with decits in adaptive behavior that
adversely affect socialization and learning. This risk factor can be applied to a caregiver or a
child.
INTENTIONALLY FALSE: A disposition that indicates a conclusion that the person who
made the allegation of maltreatment knew that the allegation was not true.
INVESTIGATION: A type of CPS response that involves the gathering of objective informa-
tion to determine whether a child was maltreated or is at-risk of maltreatment and establishes
if an intervention is needed. Generally, includes face-to-face contact with the alleged victim
and results in a disposition as to whether the alleged maltreatment occurred.
INVESTIGATION START DATE: The date when CPS initially had face-to-face contact
with the alleged victim. If this face-to-face contact is not possible, the date would be when
CPS initially contacted any party who could provide information essential to the investiga-
tion or assessment.
INVESTIGATION WORKER: A CPS agency person who performs either an investigation
response or alternative response to determine whether the alleged victim(s) in the screened-in
referral (report) was maltreated or is at-risk of maltreatment.
JUSTICE FOR VICTIMS OF TRAFFICKING ACT: Amended the Child Abuse
Prevention and Treatment Act under title VIII—Better Response for Victims of Child Sex
Trafcking by adding state reporting requirements to Section 106(d).
JUVENILE COURT PETITION: A legal document requesting that the court take action
regarding the child’s status as a result of the CPS response; usually a petition requesting the
child be declared a dependent and placed in an out-of-home setting.
Appendix B: Glossary 119
Child Maltreatment 2022

LEARNING DISABILITY: A clinically diagnosed disorder in basic psychological processes
involved with understanding or using language, spoken or written, that may manifest itself
in an imperfect ability to listen, think, speak, read, write, spell or use mathematical calcula-
tions. The term includes conditions such as perceptual disability, brain injury, minimal brain
dysfunction, dyslexia, and developmental aphasia. This risk factor term can be applied to a
caregiver or a child.
LEGAL GUARDIAN: Adult person who has been given legal custody and guardianship of a
minor.
LEGAL AND LAW ENFORCEMENT PERSONNEL: People employed by a local, state,
tribal, or federal justice agency. This includes police, courts, district attorney’s ofce, attor-
neys, probation or other community corrections agency, and correctional facilities.
LEGAL SERVICES: Activities provided by a lawyer, or other person(s) under the supervi-
sion of a lawyer, to assist individuals in seeking or obtaining legal help in civil matters such
as housing, divorce, child support, guardianship, paternity, and legal separation.
LEVEL OF EVIDENCE: The type of proof required by state statute to make a specic
nding or disposition regarding an allegation of child abuse and neglect.
LIVING ARRANGEMENT: The environment in which a child was residing at the time of
the alleged incident of maltreatment.
MALTREATMENT TYPE: A particular form of child maltreatment that received a CPS
response. Types include medical neglect, neglect or deprivation of necessities, physical abuse,
psychological or emotional maltreatment, sexual abuse, sex trafcking, and other forms
included in state law. NCANDS conducts analyses on maltreatments that received a disposi-
tion of substantiated or indicated. States should not use “8-other” maltreatment type as a ag
for maltreatment death.
MATERNAL, INFANT, AND EARLY CHILDHOOD HOME VISITING PROGRAM:
The Patient Protection and Affordable Care Act of 2010 (P.L. 111–148) authorized the cre-
ation of the Maternal, Infant, and Early Childhood Home Visiting program (MIECHV). The
program facilitates collaboration and partnership at the federal, state, and community levels
to improve health and development outcomes for at-risk children through evidence-based
home visiting programs.
MEDICAL NEGLECT: A type of maltreatment caused by failure of the caregiver to provide
for the appropriate health care of the child although nancially able to do so, or offered
nancial or other resources to do so.
MEDICAL PERSONNEL: People employed by a medical facility or practice. This includes
physicians, physician assistants, nurses, emergency medical technicians, dentists, chiroprac-
tors, coroners, and dental assistants and technicians.
MENTAL HEALTH PERSONNEL: People employed by a mental health facility or prac-
tice, including psychologists, psychiatrists, clinicians, and therapists.
Appendix B: Glossary 120
Child Maltreatment 2022

MENTAL HEALTH SERVICES: Activities that aim to overcome issues involving emo-
tional disturbance or maladaptive behavior adversely affecting socialization, learning, or
development. Usually provided by public or private mental health agencies and includes both
residential and nonresidential activities.
MILITARY FAMILY MEMBER: A legal dependent of a person on active duty in the Armed
Services of the United States such as the Army, Navy, Air Force, Marine Corps, or Coast
Guard.
MILITARY MEMBER: A person on active duty in the Armed Services of the United States
such as the Army, Navy, Air Force, Marine Corps, or Coast Guard.
NATIONAL CHILD ABUSE AND NEGLECT DATA SYSTEM (NCANDS): A national
data collection system of child abuse and neglect data from CPS agencies. Contains case-
level and aggregate data.
NATIONAL YOUTH IN TRANSITION DATABASE (NYTD): Public Law 106–169 estab-
lished the John H. Chafee Foster Care Independence Program (CFCIP), which provides states
with exible funding to assist youth with transitioning from foster care to self-sufciency.
The law required a data collection system to track the independent living services states
provide to youth and outcome measures to assess states’ performance in operating their inde-
pendent living programs. The National Youth in Transition Database (NYTD) requires states
engage in two data collection activities: (1) to collect information on each youth who receives
independent living services paid for or provided by the state agency that administers the
CFCIP; and (2) to collect demographic and outcome information on certain youth in foster
care whom the state will follow over time to collect additional outcome information. States
begin collecting data for NYTD on October 1, 2010 and report data to ACF semiannually.
NATIVE HAWAIIAN OR OTHER PACIFIC ISLANDER: A person having origins in any
of the original peoples of Hawaii, Guam, Samoa, or other Pacic Islands.
NEGLECT OR DEPRIVATION OF NECESSITIES: A type of maltreatment that refers to
the failure by the caregiver to provide needed, age-appropriate care although nancially able
to do so or offered nancial or other means to do so.
NEIGHBOR: A person living in close geographical proximity to the child or family.
NO ALLEGED MALTREATMENT: A child who received a CPS response, but was not the
subject of an allegation or any nding of maltreatment. Some states have laws requiring all
children in a household receive a CPS response, if any child in the household is the subject of
a CPS response.
NONCAREGIVER: A person who is not responsible for the care and supervision of the
child, including school personnel, friends, and neighbors.
NONPARENT: A person in a caregiver role other than an adoptive parent, biological parent,
or stepparent.
Appendix B: Glossary 121
Child Maltreatment 2022

NONVICTIM: A child with a maltreatment disposition of alternative response nonvictim,
alternative response victim, unsubstantiated, closed with no nding, no alleged maltreatment,
other, and unknown.
NONPROFESSIONAL REPORT SOURCE: Persons who did not have a relationship
with the child based on their occupation, such as friends, relatives, and neighbors. State laws
vary as to whether nonprofessionals are required to report suspected abuse and neglect.
OFFICE OF MANAGEMENT AND BUDGET (OMB): The ofce assists the President
of the United States with overseeing the preparation of the federal budget and supervising
its administration in Executive Branch agencies. It evaluates the effectiveness of agency
programs, policies, and procedures, assesses competing funding demands among agencies,
and sets funding priorities.
OTHER: The state coding for this eld is not one of the codes in the NCANDS record
layout.
OTHER RELATIVE: A nonparental family member.
OTHER MEDICAL CONDITION: A type of disability other than one of those dened in
NCANDS (i.e. behavior problem, emotional disturbance, learning disability, intellectual
disability, physically disabled, and visually or hearing impaired). The not otherwise classi-
ed disability must affect functioning or development or require special medical care (e.g.
chronic illnesses). This risk factor may be applied to a caregiver or a child.
OTHER PROFESSIONAL: A perpetrator relationship where the relationship with the child
is part of the perpetrator’s occupation and is not one of the existing codes in the NCANDS
record layout. Examples include clergy member, court staff, counselor, camp employee,
doctor, EMS/EMG, teacher, sports coach, service provider, other school personnel, etc.
OUT-OF-COURT CONTACT: A meeting, which is not part of the actual judicial hearing,
between the court-appointed representative and the child victim. Such contacts enable the
court-appointed representative to obtain a rst-hand understanding of the situation and needs
of the child victim and to make recommendations to the court concerning the best interests
of the child.
PA RENT: The birth mother or father, adoptive mother or father, or stepmother or stepfather
of a child.
PART C: A section in the Individuals with Disabilities Education Improvement Act of 2004
(IDEA) for infants and toddlers younger than 3 years with disabilities.
PERPETRATOR: The person who has been determined to have caused or knowingly
allowed the maltreatment of a child.
PERPETRATOR AGE: Age of an individual determined to have caused or knowingly
allowed the maltreatment of a child. Age is calculated in years at the time of the report of
child maltreatment.
Appendix B: Glossary 122
Child Maltreatment 2022

PERPETRATOR AS CAREGIVER: Circumstances whereby the person who caused or
knowingly allowed child maltreatment to occur was also responsible for care and supervision
of the victim when the maltreatment occurred.
PERPETRATOR IDENTIFIER (Perpetrator ID): A unique, encrypted identication
assigned to each perpetrator by the state for the purposes of the NCANDS data collection.
PERPETRATOR RELATIONSHIP: Primary role of the perpetrator to a child victim.
PETITION DATE: The month, day, and year that a juvenile court petition was led.
PLAN OF SAFE CARE: A plan developed as described in CAPTA sections 106(b)(2)(B)(iii)
for infants born and identied as being affected by substance abuse or withdrawal symptoms,
or Fetal Alcohol Spectrum Disorder. The state plan section at 106(b)(2)(B)(iii) requires that a
plan of safe care addresses the health and substance use disorder treatment needs of the infant
and affected family or caregiver. The plan of safe care may be created at any point during an
investigation or assessment. This is not considered an NCANDS service eld.
PHYSICAL ABUSE: Type of maltreatment that refers to physical acts that caused or could
have caused physical injury to a child.
PHYSICAL DISABILITY: A clinically diagnosed physical condition that adversely affects
day-to-day motor functioning, such as cerebral palsy, spina bida, multiple sclerosis,
orthopedic impairments, and other physical disabilities. This risk factor can be applied to a
caregiver or a child.
POSTRESPONSE SERVICES (also known as Postinvestigation Services):
Activities provided or arranged by the child protective services agency, social services
agency, or the child welfare agency for the child or family as a result of needs discovered
during an investigation. Includes such services as family preservation, family support, and
foster care. Postresponse services are delivered within the rst 90 days after the disposition
of the report.
PREVENTION SERVICES: Activities aimed at preventing child abuse and neglect. Such
activities may be directed at specic populations identied as being at increased risk of
becoming abusive and maybe designed to increase the strength and stability of families,
to increase parents’ condence and competence in their parenting abilities, and to afford
children a stable and supportive environment. They include child abuse and neglect preven-
tive services provided through federal, state, and local funds. These prevention activities do
not include public awareness campaigns.
PRIOR CHILD VICTIM: A child victim with previous substantiated or indicated reports of
maltreatment.
PRIOR PERPETRATOR: A perpetrator with a previous determination in the state’s
information system that he or she had caused or knowingly allowed child maltreatment to
occur. “Previous” is dened as a determination that took place prior to the disposition date of
the report being included in the dataset.
Appendix B: Glossary 123
Child Maltreatment 2022

PROFESSIONAL REPORT SOURCE: Persons who encountered the child as part of their
occupation, such as child daycare providers, educators, legal law enforcement personnel, and
medical personnel. State laws require most professionals to notify CPS agencies of suspected
maltreatment.
PROMOTING SAFE AND STABLE FAMILIES: Program that provides grants to the
states under Section 430, title IV–B, subpart 2 of the Social Security Act, as amended, to
develop and expand four types of services—community-based family support services;
innovative child welfare services, including family preservation services; time-limited
reunication services; and adoption promotion and support services.
PSYCHOLOGICAL OR EMOTIONAL MALTREATMENT: Acts or omissions—other
than physical abuse or sexual abuse—that caused or could have caused—conduct, cognitive,
affective, or other behavioral or mental disorders. Frequently occurs as verbal abuse or exces-
sive demands on a child’s performance.
PUBLIC ASSISTANCE: A risk factor related the family’s participation in social services
programs, including Temporary Assistance for Needy Families; General Assistance;
Medicaid; Social Security Income; Special Supplemental Nutrition Program for Women,
Infants, and Children (WIC); etc.
RACE: The primary taxonomic category of which the individual identies himself or herself
as a member, or of which the parent identies the child as a member. See AMERICAN
INDIAN OR ALASKA NATIVE, ASIAN, BLACK OR AFRICAN-AMERICAN, NATIVE
HAWAIIAN OR OTHER PACIFIC ISLANDER, WHITE, and UNKNOWN. Also, see
HISPA N IC.
RECEIPT OF REPORT: The log-in of a referral to the agency alleging child maltreatment.
REFERRAL: Notication to the CPS agency of suspected child maltreatment. This can
include more than one child.
REFERRAL TO APPROPRIATE SERVICES: As described in CAPTA sections 106(b)(2)
(B)(iii), this eld indicates whether the infant with prenatal substance exposure has a referral
to appropriate services, including services for the affected family or caregiver. According to
Administration for Children and Families, the denition of “appropriate services” is deter-
mined by each state. This is not considered an NCANDS service eld.
RELATIVE: A person connected to the child by adoption, blood, or marriage.
REMOVAL DATE: The month, day, and year that the child was removed from his or her
normal place of residence to a substitute care setting by a CPS agency during or as a result of
the CPS response. If a child has been removed more than once, the removal date is the rst
removal resulting from the CPS response.
REMOVED FROM HOME: The removal of the child from his or her normal place of residence
to a foster care setting.
Appendix B: Glossary 124
Child Maltreatment 2022

REPORT: A screened-in referral alleging child maltreatment. A report receives a CPS
response in the form of an investigation response or an alternative response.
REPORT-CHILD PAIR: Refers to the concatenation of the Report ID and the Child ID,
which together form a new unique ID that represents a single unique record in the Child File.
REPORT DATE: The day, month, and year that the responsible agency was notied of the
suspected child maltreatment.
REPORT DISPOSITION: The point in time at the end of the investigation or assessment
when a CPS worker makes a nal determination (disposition) about whether the alleged
maltreatment occurred.
REPORT DISPOSITION DATE: The day, month, and year that the report disposition was
made.
REPORT IDENTIFIER (Report ID): A unique identication assigned to each report of
child maltreatment for the purposes of the NCANDS data collection.
REPORT SOURCE: The category or role of the person who noties a CPS agency of
alleged child maltreatment.
REPORTING PERIOD: The 12-month period for which data is submitted to the NCANDS.
RESIDENTIAL FACILITY STAFF: Employees of a public or private group residential
facility, including emergency shelters, group homes, and institutions.
RESPONSE TIME FROM REFERRAL TO INVESTIGATION OR ALTERNATIVE
RESPONSE: The response time is dened as the time between the receipt of a call to the
state or local agency alleging maltreatment and face-to-face contact with the alleged victim,
wherever this is appropriate, or with another person who can provide information on the
allegation(s).
RESPONSE TIME FROM REFERRAL TO THE PROVISION OF SERVICES: The
time from the receipt of a referral to the state or local agency alleging child maltreatment to the
provision of post response services, often requiring the opening of a case for ongoing services.
SCREENED-IN REFERRAL: An allegation of child maltreatment that met the state’s
standards for acceptance and became a report.
SCREENED-OUT REFERRAL: An allegation of child maltreatment that did not meet the
state’s standards for acceptance.
SCREENING: Agency hotline or intake units conduct the screening process to determine
whether a referral is appropriate for further action. Referrals that do not meet agency criteria
are screened-out or diverted from CPS to other community agencies. In most states, a refer-
ral may include more than one child.
Appendix B: Glossary 125
Child Maltreatment 2022

SERVICE DATE: The date activities began as a result of needs discovered during the CPS
response.
SERVICES: See POSTRESPONSE SERVICES and PREVENTION SERVICES.
SEXUAL ABUSE: A type of maltreatment that refers to the involvement of the child in
sexual activity to provide sexual gratication or nancial benet to the perpetrator, including
contacts for sexual purposes, molestation, statutory rape, prostitution, pornography, expo-
sure, incest, or other sexually exploitative activities.
SEX TRAFFICKING: A type of maltreatment that refers to the recruitment, harboring,
transportation, provision, or obtaining of a person for the purpose of a commercial sex act.
States have the option to report to NCANDS any sex trafcking victim who is younger than
24 years.
SOCIAL SERVICES BLOCK GRANT (SSBG): Funds provided by title XX of the Social
Security Act that are used for services to the states that may include child protection, child
and foster care services, and daycare.
SOCIAL SERVICES PERSONNEL: Employees of a public or private social services or
social welfare agency, or other social worker or counselor who provides similar services.
STATE: In NCANDS, the primary unit from which child maltreatment data is collected.
This includes all 50 states, the Commonwealth of Puerto Rico, and the District of Columbia.
STATE CONTACT PERSON: The state person with the responsibility to provide informa-
tion to the NCANDS.
STEPPARENT: The husband or wife, by a subsequent marriage, of the child’s mother or
father.
SUBSTANCE ABUSE SERVICES: Activities designed to deter, reduce, or eliminate
substance abuse or chemical dependency.
SUBSTANTIATED: An investigation disposition that concludes that the allegation of
maltreatment or risk of maltreatment was supported or founded by state law or policy.
SUMMARY DATA COMPONENT (SDC): The aggregate data collection form submitted
by states that do not submit the Child File. This form was discontinued for the FFY 2012 data
collection.
TEMPORARY ASSISTANCE FOR NEEDY FAMILIES (TANF): A block grant that is
administered by state, territorial, and tribal agencies. Citizens can apply for TANF at the
respective agency administering the program in their community.
UNIQUE COUNT OF CHILDREN: Counting a child once, regardless of the number of
reports concerning that child, who received a CPS response in the FFY.
Appendix B: Glossary 126
Child Maltreatment 2022

UNIQUE COUNT OF PERPETRATORS: Counting a perpetrator once, regardless of the
number of children the perpetrator is associated with maltreating or the number of records
associated with a perpetrator.
UNKNOWN: The state may collect data on this variable, but the data for this particular
report or child were not captured or are missing.
UNMARRIED PARTNER OF PARENT: Someone who has an intimate relationship with
the parent and lives in the household with the parent of the maltreated child.
UNSUBSTANTIATED: An investigation disposition that determines that there was not
sufcient evidence under state law to conclude or suspect that the child was maltreated or
was at -risk of being maltreated.
VISUAL OR HEARING IMPAIRMENT: A clinically diagnosed condition related to a
visual impairment or permanent or uctuating hearing or speech impairment that may affect
functioning or development. This term can be applied to a caregiver or a child.
VICTIM: A child for whom the state determined at least one maltreatment was substantiated
or indicated; and a disposition of substantiated or indicated was assigned for a child in a
specic report. This includes a child who died and the death was conrmed to be the result
of child abuse and neglect. A child may be a victim in one report and a nonvictim in another
report.
WHITE: A person having origins in any of the original peoples of Europe, the Middle East,
or North Africa. Race may be self-identied or identied by a caregiver.
WORKER IDENTIFIER (WORKER ID): A unique identication of the worker who is
assigned to the child at the time of the report disposition.
WORKFORCE: Total number of workers in a CPS agency.
Appendix B: Glossary 127
Child Maltreatment 2022

State Characteristics
Administrative Structure
States vary in how they administer and deliver child welfare services. Forty states (including
the District of Columbia and the Commonwealth of Puerto Rico) have a centralized system
classied as state administered. Ten states are classied as state supervised, county admin-
istered; and two states are classied as “hybrid” meaning they are partially administered
by the state and partially administered by counties. Each state’s administrative structure (as
submitted by the state as part of Appendix D, State Commentary) is provided in table C–1.
Level of Evidence
States use a certain level of evidence to determine whether maltreatment occurred or the
child is at-risk of maltreatment. Level of evidence is dened as the proof required to make
a specic nding or disposition regarding an allegation of child abuse and neglect. Each
state’s level of evidence (as submitted by each state as part of commentary in appendix D) is
provided in table C–1.
Data Submissions
States submit case-level data by constructing an electronic le of child-specic records for
each report of alleged child abuse and neglect that received a CPS response. Each state’s
submission includes only completed reports that resulted in a disposition (or nding) as an
outcome of the CPS response during the reporting year. The data submission containing these
case-level data is called the Child File.
The Child File is supplemented by agency-level aggregate statistics in a separate data submis-
sion called the Agency File. The Agency File contains data that are not reportable at the
child-specic level and often gathered from agencies external to CPS. States are asked to
submit both the Child File and the Agency File each year. For FFY 2022, 52 states submitted
both a Child File and an Agency File.
Once validated, the Child Files and Agency Files are loaded into the multiyear, multistate
NCANDS Data Warehouse. The FFY 2022 dataset is available to researchers from the
National Data Archive on Child Abuse and neglect (NDACAN).
APPENDIX C
Appendix C: State Characteristics 128
Child Maltreatment 2022

Child Population Data
The child population data for years 2018–2022 is displayed by state in table C–2. The
2022 child population data for the demographics of age, sex, and race and ethnicity is
displayed by state in table C–3. The adult population is displayed in table C–4.
Appendix C: State Characteristics 129
Child Maltreatment 2022

Table C–1 State Administrative Structure, Level of Evidence, and Data Files
Submitted, 2022
State Hybrid
State
Administered
State
Supervised,
County
Administered Credible Preponderance
Probable
Cause Reasonable
Agency File and
Child File
Alabama - 1 - - 1 - - 1
Alaska - 1 - - 1 - - 1
Arizona - 1 - - - 1 - 1
Arkansas - 1 - - 1 - - 1
California - - 1 - 1 - - 1
Colorado - - 1 - 1 - - 1
Connecticut - 1 - - - - 1 1
Delaware - 1 - - 1 - - 1
District of Columbia - 1 - 1 - - - 1
Florida - 1 - - 1 - - 1
Georgia - 1 - - 1 - - 1
Hawaii - 1 - - - - 1 1
Idaho - 1 - - 1 - -
1
Illinois - 1 - 1 - - -
1
Indiana - 1 - - 1 - - 1
Iowa - 1 - - 1 - - 1
Kansas - 1 - - 1 - - 1
Kentucky - 1 - - 1 - - 1
Louisiana - 1 - - - - 1 1
Maine - 1 - - 1 - - 1
Maryland - 1 - - 1 - - 1
Massachusetts - 1 - - - - 1 1
Michigan - 1 - - 1 - - 1
Minnesota - - 1 - 1 - - 1
Mississippi - 1 - 1 - - - 1
Missouri - 1 - - 1 - - 1
Montana - 1 - - 1 - - 1
Nebraska - 1 - - 1 -
- 1
Nevada 1 - - - 1 -
- 1
New Hampshire - 1 - - 1 - - 1
New Jersey - 1 - - 1 - - 1
New Mexico - 1 - 1 - - - 1
New York - - 1 - 1 - - 1
North Carolina - - 1 - 1 - - 1
North Dakota - - 1 - 1 - - 1
Ohio - - 1 1 - - - 1
Oklahoma - 1 - 1 - - - 1
Oregon - 1 - - - - 1 1
Pennsylvania - - 1 - 1 - - 1
Puerto Rico - 1 - - 1 - - 1
Rhode Island - 1 - - 1 - - 1
South Carolina - 1 - - 1 - - 1
South Dakota - 1 - - 1
- - 1
Tennessee - 1 - - 1
- - 1
Texas - 1 - - 1 - - 1
Utah - 1 - - - - 1 1
Vermont - 1 - - - - 1 1
Virginia - - 1 - 1 - - 1
Washington - 1 - - 1 - - 1
West Virginia - 1 - - 1 - - 1
Wisconsin 1 - - - 1 - - 1
Wyoming - - 1 - 1 - - 1
States Reporting 2 40 10 6 38 1 7 52
Note: Level of evidence is listed in alphabetical order.
Appendix C: State Characteristics 130
Child Maltreatment 2022

Table C–2 Child Population, 2018–2022
State 2018 2019 2020 2021 2022
Alabama 1,092,599 1,088,727 1,111,214 1,110,087 1,111,562
Alaska 183,189 180,442 179,073 177,739 176,523
Arizona 1,638,657 1,641,727 1,595,098 1,592,435 1,589,010
Arkansas 703,626 701,317 696,663 695,680 697,119
California 8,974,477 8,881,104 8,818,239 8,652,868 8,506,027
Colorado 1,264,226 1,256,673 1,246,974 1,232,116 1,215,575
Connecticut 736,061 727,280 743,209 735,582 731,030
Delaware 204,154 204,263 206,791 206,703 208,127
District of Columbia 126,703 127,952 125,248 123,996 124,475
Florida 4,226,134 4,233,967 4,229,720 4,234,511 4,296,354
Georgia 2,509,456 2,505,399 2,515,174 2,505,369 2,510,123
Hawaii 303,049 299,419 306,640 301,536 297,326
Idaho 445,134 448,116 453,179 460,778 463,404
Illinois 2,857,349 2,817,312 2,831,998 2,775,737 2,720,131
Indiana 1,572,404 1,569,375 1,580,111 1,573,388 1,569,923
Iowa 729,802 728,005 732,396 727,981 724,489
Kansas 706,593 701,453 702,969 695,904 690,832
Kentucky 1,008,017 1,004,268 1,011,281 1,007,420 1,004,575
Louisiana 1,098,318 1,089,906 1,086,208 1,074,840 1,061,693
Maine 250,465 249,610 251,067 249,306 247,898
Maryland 1,341,430 1,338,232 1,366,422 1,354,373 1,346,589
Massachusetts 1,365,956
1,353,615 1,372,918 1,350,968 1,337,434
Michigan 2,163,590 2,144,307 2,154,460 2,130,448 2,109,695
Minnesota 1,303,090 1,303,212 1,314,083 1,302,973 1,294,162
Mississippi 707,663 699,984 690,717 684,333 678,061
Missouri 1,379,108 1,374,703 1,375,337 1,369,735 1,364,908
Montana 229,210 228,888 231,291 232,568 233,753
Nebraska 476,581 476,033 482,095 478,986 476,677
Nevada 688,989 694,730 693,062 690,856 689,778
New Hampshire 258,045 255,785 256,250 254,597 252,924
New Jersey 1,954,045 1,943,575 2,026,114 2,006,286 1,994,109
New Mexico 482,442 477,209 476,375 467,455 459,513
New York 4,074,414 4,031,894 4,168,699 4,069,680 3,989,288
North Carolina 2,304,529 2,304,554 2,281,275 2,281,611 2,294,879
North Dakota 178,524 180,584 184,438 183,162 182,775
Ohio 2,595,584 2,581,403 2,599,462 2,580,179 2,562,550
Oklahoma 955,996 953,923 949,504 950,246 953,146
Oregon 868,879 864,815 862,084 851,011 836,988
Pennsylvania 2,653,058 2,635,819 2,672,072 2,648,608 2,624,465
Puerto Rico 591,875 572,801 566,375 544,770 518,339
Rhode Island 206,059 203,923 209,450 206,453 203,912
South Carolina 1,108,588 1,113,673 1,101,228 1,105,504 1,117,872
South Dakota 216,722 217,817 216,814 217,484 219,165
Tennessee 1,510,375 1,510,976 1,525,952
1,528,425 1,538,137
Texas 7,382,686 7,406,777 7,404,862 7,401,483 7,456,338
Utah 930,162 929,940 938,051 936,962 931,608
Vermont 115,630 114,325 117,118 115,868 114,757
Virginia 1,870,042 1,868,689 1,883,392 1,871,848 1,866,910
Washington 1,657,823 1,661,024 1,675,164 1,660,819 1,646,573
West Virginia 365,119 360,439 358,327 354,931 351,922
Wisconsin 1,276,066 1,267,935 1,273,285 1,258,867 1,245,629
Wyoming 134,683 133,577 132,639 131,341 130,114
National 73,977,376 73,661,476 73,982,567 73,356,806 72,969,166
States Reporting 52 52 52 52 52
Note: Arizona did not submit FFY 2021 NCANDS data; however, the state’s population data is presented in this appendix.
Appendix C: State Characteristics 131
Child Maltreatment 2022

Table C–3 Child Population Demographics, 2022 (continues next page)
State
<1 1 2
3 4 5 6 7 8
Alabama
57,882 57,185 57,342
58,047 59,843 60,337 61,461 61,795 61,106
Alaska
9,490 9,266 9,338
9,203 9,508 9,951 10,085 10,090 10,186
Arizona
78,579 75,953 78,226
80,157 82,091 84,356 87,197 89,225 89,233
Arkansas
35,980 35,287 35,602
36,347 37,173 37,782 38,704 38,801 38,417
California
425,149 407,106 423,040
430,701 441,768 458,025 469,417 476,874 476,454
Colorado
62,867 61,287 61,203
61,031 62,632 64,383 66,584 67,216 67,207
Connecticut
35,870 34,725 36,348
36,903 37,761 38,212 39,099 39,572 39,630
Delaware
10,785 10,421 10,725
10,794 11,041 11,165 11,454 11,524 11,464
District of Columbia
8,261 8,124 7,494
7,486 7,734 7,692 7,573 7,526 7,117
Florida
220,782 213,207 219,121
224,408 229,286 232,262 238,298 239,209 238,908
Georgia
124,954 122,903 125,429
127,431 130,828 133,350 136,735 138,395 137,873
Hawaii
15,804 15,287 15,743
16,255 16,511 16,980 17,313 17,295 17,450
Idaho
22,368 22,135 22,592
22,726 23,462 24,512 25,669 26,072 25,808
Illinois
131,093 130,551 136,510
139,036 143,151 146,312 150,336 151,512 149,730
Indiana
79,786 77,980 81,262
81,942 83,976 84,475 86,914 87,677 87,268
Iowa
36,786 36,147 37,262
37,402 38,603 39,256 40,172 40,525 40,398
Kansas
34,772 34,179 35,015
35,368 36,108 37,020 38,127 38,410 38,574
Kentucky
52,123 51,365 52,204
52,954 54,067 54,574 55,553 55,855 55,996
Louisiana
56,702 55,854 54,832
55,523 57,109 58,172 59,890 59,795 59,402
Maine
12,002 11,642 12,599
12,727 12,774 13,052 13,512 13,633 13,686
Maryland
69,158 67,332 70,272
70,858 72,224 73,063 74,661 74,849 74,531
Massachusetts
70,623 66,626 68,018
68,261 70,068 71,067 72,213 73,018 73,217
Michigan
104,605 102,891 108,177
109,024 111,728 113,892 116,449 117,437 117,389
Minnesota
64,755 63,318 66,458
67,078 68,517 70,536 72,313 72,952 72,837
Mississippi
34,735 34,572 34,545
35,011 35,655 35,589 36,300 36,573 36,526
Missouri
69,009 68,695 71,059
71,786 73,056 73,805 75,185
75,841 75,739
Montana
11,201 11,036 11,589
11,745 12,075 12,646 13,274 13,417 13,270
Nebraska
24,347 24,145 24,720
25,044 25,581 26,163 26,904 26,959 26,905
Nevada
33,611 33,672 34,944
35,787 36,230 37,107 38,574 38,774 38,435
New Hampshire
12,713 12,272 12,550
12,657 12,752 13,152 13,466 13,683 13,762
New Jersey
102,910 98,851 103,206
104,719 106,769 107,742 109,428 109,728 109,400
New Mexico
20,830 21,207 21,855
22,739 23,397 23,886 24,865 25,532 25,618
New York
214,746 201,750 211,104
214,218 217,399 218,902 221,434 222,892 220,938
North Carolina
121,554 117,878 117,750
118,542 120,766 122,446 124,831 126,027 125,460
North Dakota
10,093 9,824 9,920
9,932 10,160 10,485 10,766 10,655 10,440
Ohio
128,822 128,268 132,681
134,077 137,573 138,892 141,863 142,996 142,906
Oklahoma
47,793 47,556 48,509
49,315 50,498 51,749 53,470 53,687 53,958
Oregon
41,052 39,419 41,123
41,539 42,941 44,373 46,319 47,071 47,306
Pennsylvania
131,552 130,017 134,616
135,996 139,024 140,977 144,122 145,746 145,973
Puerto Rico
19,337
18,240 19,695
21,055 21,232 23,046 25,496 27,427 29,138
Rhode Island
10,532 9,969 10,545
10,736 10,918 11,070 11,359 11,287 11,169
South Carolina
56,849 56,543 56,731
57,129 58,631 59,217 60,948 61,819 61,686
South Dakota
11,445 11,184 11,663
11,793 12,008 12,168 12,375 12,269 12,335
Tennessee
81,460 79,643 80,447
81,111 82,760 82,754 84,802 85,017 84,524
Texas
378,682 370,760 376,841
383,360 392,996 404,723 419,724 423,784 421,340
Utah
46,679 45,123 46,928
46,864 47,480 49,183 51,203 51,874 51,994
Vermont
5,364 5,201 5,537
5,672 5,820 6,053 6,276 6,383 6,462
Virginia
96,728 94,430 96,943
98,575 100,817 101,327 104,140 104,002 103,241
Washington
84,431 82,628 85,637
85,464 87,669 90,933 93,251 93,193 92,578
West Virginia
17,376 17,331 17,590
17,616 18,084 18,308 18,959 19,471 19,816
Wisconsin
61,278 59,985 63,254
63,448 64,657 66,356 68,106 68,554 68,429
Wyoming
6,145 6,087 6,263
6,299 6,546 6,866 7,225 7,238 7,250
National
3,702,450 3,607,057 3,713,057
3,763,891 3,851,457
3,930,344 4,034,394 4,071,156 4,060,479
Reporting States
52 52 52
52 52 52 52 52 52
Appendix C: State Characteristics 132
Child Maltreatment 2022

Table C–3 Child Population Demographics, 2022 (continues next page)
State
9 10 11
12 13 14 15 16 17
Alabama 60,574 60,929 61,557 63,172 65,086 67,703 67,299 65,600 64,644
Alaska 10,192 10,068 10,137 10,016 10,039 10,027 9,844 9,549 9,534
Arizona 88,585 88,533 89,383 91,496 94,654 98,846 99,118 97,254 96,124
Arkansas 38,220 38,462 38,755 39,660 40,711 42,455 42,426 41,519 40,818
California 477,398 478,124 485,870 491,255 499,146 521,730 521,347 513,196 509,427
Colorado 66,703 67,209 68,629 70,774 71,921 74,487 74,510 73,653 73,279
Connecticut 39,824 40,256 41,334 42,279 43,709 45,883 46,483 46,292 46,850
Delaware 11,453 11,718 11,806 11,957 12,171 12,597 12,496 12,420 12,136
District of Columbia 7,151 7,014 6,717 6,197 5,994 5,889 5,740 5,461 5,305
Florida 237,283 238,004 240,410 244,105 249,272 260,073 260,758 257,383 253,585
Georgia 137,836 139,682 141,864 145,037 149,485 156,503 156,520 153,616 151,682
Hawaii 17,544 17,364 17,107 16,521 16,196 16,587 16,095 15,695 15,579
Idaho 25,931 25,873 26,301
27,435 28,027 29,107 28,987 28,336 28,063
Illinois 149,210 150,798 153,377 157,591 161,052 167,802 168,248 166,608 167,214
Indiana 87,074 87,164 87,304 89,399 91,589 94,992 94,943 93,335 92,843
Iowa 39,970 39,584 39,665 41,414 42,822 44,266 44,186 43,423 42,608
Kansas 38,733 38,804 39,256 40,292 40,841 41,994 41,855 41,007 40,477
Kentucky 55,687 55,429 55,412 56,597 58,224 60,423 60,381 59,123 58,608
Louisiana 58,259 57,960 58,168 59,459 61,342 63,802 63,537 61,519 60,368
Maine 13,682 13,612 13,737 14,390 14,792 15,377 15,588 15,477 15,616
Maryland 74,313 74,682 76,009 77,063 78,203 81,266 80,706 79,062 78,337
Massachusetts 73,423 74,086 74,962 76,486 77,791 80,937 81,849 81,732 83,057
Michigan 116,571 116,665 117,820 121,011 123,279 127,960 128,719 127,945 128,133
Minnesota 72,351 72,228 72,286 74,047 75,727 78,167 77,951 76,613 76,028
Mississippi 36,362 36,976 37,378 38,637 40,639 42,986 43,408 41,631 40,538
Missouri 75,187 75,296 76,118 77,639 79,728 82,679 82,489
81,398 80,199
Montana 13,194 13,302 13,234 13,474 13,891 14,380 14,294 14,058 13,673
Nebraska 26,551 26,269 26,438 27,107 27,776 28,429 28,205 27,660 27,474
Nevada 38,348 38,489 39,364 39,749 40,706 42,509 42,337 41,087 40,055
New Hampshire 13,995 13,987 14,400 14,624 15,006 15,760 15,943 16,079 16,123
New Jersey 109,451 110,412 112,316 114,071 115,895 120,254 120,648 119,172 119,137
New Mexico 25,910 26,069 26,588 27,464 28,169 29,210 29,122 28,601 28,451
New York 221,418 222,169 224,197 224,586 225,178 232,368 232,158 231,121 232,710
North Carolina 125,019 125,824 127,187 131,294 135,405 140,606 140,274 137,880 136,136
North Dakota 10,312 10,221 9,905 10,008 10,058 10,304 10,151 9,917 9,624
Ohio 142,627 141,702 141,689 145,132 149,198 154,506 154,665 152,944 152,009
Oklahoma 53,964 53,778 53,713 54,700 55,720 57,494 56,988 55,509 54,745
Oregon 46,972 47,349 47,851 49,047 50,088 52,173 51,667 50,671 50,027
Pennsylvania 145,651 146,052 147,307 150,293 153,629 159,245 159,090 157,601 157,574
Puerto Rico 30,590
31,905 32,804 34,407 35,236 35,733 36,840 37,871 38,287
Rhode Island 11,114 11,136 11,219 11,393 11,662 12,261 12,342 12,528 12,672
South Carolina 61,235 61,765 62,509 64,834 67,201 69,378 69,210 66,958 65,229
South Dakota 12,233 12,161 12,175 12,443 12,606 12,923 12,804 12,420 12,160
Tennessee 84,219 84,452 84,297 86,520 89,410 93,357 92,843 90,995 89,526
Texas 416,286 413,163 419,340 429,979 437,182 450,643 446,877 437,879 432,779
Utah 52,131 51,715 52,683 54,610 55,896 57,839 57,658 56,386 55,362
Vermont 6,405 6,509 6,599 6,668 6,829 7,197 7,269 7,232 7,281
Virginia 103,094 103,479 104,447 105,515 107,629 112,066 111,837 109,834 108,806
Washington 92,513 91,955 92,656 94,454 95,813 98,200 97,175 94,570 93,453
West Virginia 19,985 19,894 19,936 20,410 20,948 21,772 21,762 21,398 21,266
Wisconsin 68,471 68,934 69,750 72,743 74,505 77,357 77,513 76,411 75,878
Wyoming 7,315 7,241 7,402 7,764 8,044 8,264 8,251 8,050 7,864
National
4,048,519 4,056,452 4,101,368
4,187,218 4,276,120
4,438,766 4,433,406 4,363,679 4,329,353
Reporting States
52 52 52
52 52 52 52 52 52
Appendix C: State Characteristics 133
Child Maltreatment 2022

Table C–3 Child Population Demographics, 2022
State
Boy Girl
American
Indian
or Alaska
Native
Asian
Black or
African-
American Hispanic
Native
Hawaiian or
Other Pacic
Islander
Two or More
Races White
Alabama 567,219 544,343 3,918 16,398 321,268 97,028 630 41,970 630,350
Alaska 90,546 85,977 32,210 9,910 5,104 18,794 4,261 24,376 81,868
Arizona 811,998 777,012 71,099 48,994 85,467 713,117 3,043 70,441 596,849
Arkansas 357,251 339,868 4,896 12,882 123,423 92,500 4,981 29,314 429,123
California 4,356,524 4,149,503 30,371 1,100,745 424,411 4,412,585 30,139 460,558 2,047,218
Colorado 622,562 593,013 6,518 43,292 55,001 398,760 2,380 59,041 650,583
Connecticut 372,647 358,383 2,045 39,610 86,746 200,353 358 30,086 371,832
Delaware 105,894 102,233 464 9,296 54,234 36,873 89 12,321 94,850
District of Columbia 63,302 61,173 172 3,121 64,167 22,028 51 5,657 29,279
Florida 2,196,698 2,099,656 8,737 122,697 843,533 1,374,388 3,090 173,375 1,770,534
Georgia 1,279,930 1,230,193 4,439 112,285 853,849 384,238 2,331 105,430
1,047,551
Hawaii 153,246 144,080 412 64,516 5,044 58,381 33,374 95,091 40,508
Idaho 237,673 225,731 4,295
5,926 4,185 90,808 855 17,497 339,838
Illinois 1,390,234 1,329,897 3,766 155,327 419,638 676,284 784 102,630 1,361,702
Indiana 804,957 764,966 2,473 45,959 184,225 190,519 775 70,981 1,074,991
Iowa 370,986 353,503 2,475 19,986 42,906 80,905 2,366 31,081 544,770
Kansas 354,059 336,773 4,339 20,068 42,750 134,466 1,005 38,430 449,774
Kentucky 515,304 489,271 1,272 19,556 94,426 71,573 1,073 46,514 770,161
Louisiana 541,968 519,725 6,033 17,968 383,080 87,937 361 36,138 530,176
Maine 127,239 120,659 1,870 3,436 8,612 8,511 102 10,025 215,342
Maryland 687,670 658,919 2,616 88,368 412,016 238,427 542 74,533 530,087
Massachusetts 684,334 653,100 2,391 106,561 124,718 272,695 748 58,375 771,946
Michigan 1,081,733 1,027,962 11,407 75,022 344,539 188,107 644 108,534 1,381,442
Minnesota 662,115 632,047 17,683 85,772 143,885 122,338 1,134 69,459 853,891
Mississippi 345,018 333,043
3,908 7,026 279,192 36,926 223 19,447 331,339
Missouri 700,792 664,116 4,658 28,984 183,200 103,102 3,085
69,497 972,382
Montana 120,246 113,507 20,953 2,101 1,433 17,102 217 11,418 180,529
Nebraska 244,639 232,038 4,867 13,890 29,320 92,090 380 20,552 315,578
Nevada 353,110 336,668 4,933 44,203 78,500 287,709 5,520 51,337 217,576
New Hampshire 129,653 123,271 403 9,187 5,432 19,772 92 8,928 209,110
New Jersey 1,020,890 973,219 3,488 206,299 269,176 573,386 958 67,185 873,617
New Mexico 234,522 224,991 44,880 6,004 8,626 283,225 221 12,853 103,704
New York 2,043,317 1,945,971 12,290 358,010 588,446 1,006,380 2,070 157,452 1,864,640
North Carolina 1,171,950 1,122,929 24,440 88,422 513,645 406,491 1,901 110,338 1,149,642
North Dakota 93,400 89,375 12,676 3,282 8,746 14,018 244 8,723 135,086
Ohio 1,311,874 1,250,676 3,573 73,795 397,722 180,980 1,500 135,700 1,769,280
Oklahoma 488,022 465,124 89,212 22,283 74,831 182,695 2,895 99,663 481,567
Oregon 429,127 407,861 8,409 37,753 19,998 197,706
4,427 56,299 512,396
Pennsylvania 1,344,485 1,279,980 3,432 113,829 336,838 369,512 999 116,200 1,683,655
Puerto Rico 263,450
254,889 - - - - - - -
Rhode Island 104,270 99,642 944 7,615 15,129 59,362 156 10,069 110,637
South Carolina 569,719 548,153 3,178 21,481 319,111 120,782 832 50,191 602,297
South Dakota 112,186 106,979 25,086 3,964 7,518 18,258 273 10,964 153,102
Tennessee 786,278 751,859 2,983 31,117 285,394 170,507 1,053 65,951 981,132
Texas 3,809,464 3,646,874 17,647 368,667 937,582 3,650,284 7,016 219,065 2,256,077
Utah 479,569 452,039 7,431 18,688 11,588 180,038 11,228 37,165 665,470
Vermont 59,258 55,499 275 2,689 2,197 3,700 32 4,748 101,116
Virginia 956,943 909,967 3,789 129,028 371,635 286,896 1,213 116,093 958,256
Washington 843,855 802,718 19,756 145,920 73,460 381,199 15,122 145,899 865,217
West Virginia 180,517 171,405 478 2,770 13,067 11,025 71 16,508 308,003
Wisconsin 638,348 607,281 12,739 50,719 110,901 161,749 602 55,118 853,801
Wyoming
66,728 63,386 3,390 989 1,248 21,240 83 4,666 98,498
National 37,337,719 35,631,447 565,719 4,026,410 10,071,162
18,807,749 157,529 3,453,886 35,368,372
Reporting States 52 52 51 51 51 51 51 51 51
Appendix C: State Characteristics 134
Child Maltreatment 2022

Table C–4 Adult Population by Age Group, 2022
State 18–24 25–34 35–44 45–54 55–64 65–75 75 and Older
Alabama 492,021 657,905 621,848 617,797 658,430 540,882 373,851
Alaska 68,417 113,239 103,579 82,973 87,241 67,276 34,335
Arizona 719,560 1,018,332 926,056 851,890 871,963 780,707 601,679
Arkansas 290,231 397,098 381,818 358,703 378,312 314,714 227,642
California 3,671,979 5,747,351 5,390,648 4,870,281 4,687,309 3,560,888 2,594,859
Colorado 554,057 915,481 847,768 709,151 683,856 560,039 353,999
Connecticut 351,037 453,483 459,894 451,707 515,736 379,930 283,388
Delaware 87,585 128,230 123,537 115,577 143,496 127,275 84,569
District of Columbia 68,000 145,567 110,949 71,480 64,072 49,975 37,285
Florida 1,848,181 2,805,343 2,785,238 2,725,291 2,990,220 2,602,139 2,192,057
Georgia 1,066,375 1,511,231 1,445,295 1,397,510 1,337,315 994,257 650,770
Hawaii 120,702 190,533 191,386 168,913 176,971 162,235 132,130
Idaho 195,931 251,203 252,364 219,580 226,099 199,485 130,967
Illinois 1,169,741 1,696,752 1,667,941 1,557,864 1,606,306 1,261,263 902,034
Indiana 677,421 897,480 860,267 815,676 856,592 687,211 468,467
Iowa 328,493 398,236 402,238 359,453 401,578
337,487 248,543
Kansas 307,521 376,350 376,397 327,300 354,733 295,510 208,507
Kentucky 417,856 592,553 561,994 554,804 587,521 476,723 316,284
Louisiana 430,681 609,176 604,031 526,426 578,173 470,868 309,193
Maine 110,462 168,183 168,691 168,198 209,684 185,170 127,054
Maryland 534,403 809,165 833,654 771,708 824,932 608,281 435,928
Massachusetts 697,284 973,637 905,724 856,003 951,354 731,544 528,994
Michigan 954,220 1,318,494 1,210,540 1,202,633 1,358,196 1,123,281 757,054
Minnesota 514,740 740,688 771,968 659,534 738,560 584,717 412,815
Mississippi 291,755 376,071 363,978 351,380 371,272 302,852 204,688
Missouri 579,119 811,793 789,531 716,515 801,736 651,257 463,098
Montana 105,048 146,861 144,219 123,294 144,566 136,767 88,359
Nebraska 197,324 251,846 256,829 218,041 234,150 195,520 137,536
Nevada 264,715 459,107 438,086 397,653 391,429 322,106 214,898
New Hampshire 120,734 179,394 171,925 172,601 216,147 169,274 112,232
New Jersey 794,866 1,188,554 1,220,287 1,195,135 1,256,981 922,378 689,389
New Mexico 206,755 278,336 269,909 234,581 260,847 238,437 164,966
New York 1,803,036 2,767,531 2,533,370
2,400,391 2,619,959 2,028,832 1,534,744
North Carolina 1,038,619 1,437,479 1,351,351 1,346,958 1,367,808 1,106,578 755,301
North Dakota 89,432 109,433 100,523 78,235 88,935 74,880 55,048
Ohio 1,068,727 1,550,443 1,463,046 1,402,830 1,546,264 1,281,505 880,693
Oklahoma 406,600 541,538 524,996 457,226 475,399 388,508 272,387
Oregon 370,811 592,618 591,471 519,401 513,170 485,969 329,709
Pennsylvania 1,200,378 1,682,014 1,619,711 1,537,517 1,765,997 1,469,045 1,072,881
Puerto Rico 288,570 432,303 377,915 409,529 438,284 383,985 372,864
Rhode Island 111,927 151,442 137,963 130,073 152,007 119,463 86,947
South Carolina 494,280 680,762 651,751 633,857 696,103 604,646 403,363
South Dakota 87,029 114,295 114,374 96,313 114,831 99,880 63,937
Tennessee 644,140 976,563 892,438 872,524 906,548 729,524 491,465
Texas 3,026,333 4,337,408 4,203,606 3,676,667 3,302,167 2,438,490 1,588,563
Utah 403,891 498,913 463,662 369,405 308,121 245,876 159,324
Vermont 65,681 77,521 79,179 76,758 93,717 83,482 55,969
Virginia 823,295 1,174,486 1,167,939 1,075,904 1,110,097 858,089 606,899
Washington 677,198 1,181,605 1,109,502 930,283 932,065 784,582 523,978
West Virginia 159,635
212,994 210,862 222,858 240,786 222,956 153,143
Wisconsin 565,598 733,535 743,390 689,605 812,663 658,626 443,493
Wyoming 54,307 73,048 77,642 65,188 73,023 67,060 40,999
National 31,616,701 45,933,603 44,073,280 40,841,174 42,523,721 34,172,424 24,379,277
Reporting States 52 52 52 52 52 52 52
Appendix C: State Characteristics 135
Child Maltreatment 2022

Alabama
Contact Holly Christian Phone 334–353–4898
Title Deputy Director, Children and Family Services
Division
Email
holly.christian@dhr.alabama.gov
Address Alabama Department of Human Resources
50 Ripley Street
Montgomery, AL 36130–4000
General
Federal scal year (FFY) 2022 is the fourteenth NCANDS submission from our
Comprehensive Child Welfare Information System (CCWIS). There were no changes in poli-
cies, programs or procedures that affected the 2022 submission of NCANDS data. Variances
in data compared to previous years may occur as we have continued work to strengthen our
data collection processes in the system. Enhancements are completed each year to continue
efforts to improve reporting of services to children and families, perpetrator data and map-
ping of NCANDS elements.
Alabama has two types of screened-in responses: child abuse and neglect investigations (CA/
Ns) and prevention assessments (alternative response). For FFY 2022, the Child File included
only CA/Ns, which have allegations of abuse or neglect. Prevention Assessments are reports
that do not include allegations of abuse/neglect, but the potential risk for abuse may exist.
A Prevention Assessment may be changed to a CA/N report if an allegation is added to the
system. At that time, policy for CA/N Investigations are in effect. The FFY 2022 submission
does not include prevention assessment data in the Child File.
Reports
The state did not change its screening protocol due to the pandemic that began in 2020. The
state has maintained the same policy and requirements for in person investigations. No poli-
cies or procedures were changed related to the screening or completion of reports.
A policy change was implemented in FFY 2017 that decreased the timeframe permitted
to complete CA/N investigations from 90 days to 60 days. The state did not modify the
State Commentary
APPENDIX D
This section provides insights into policies and conditions that may affect state data. Readers
are encouraged to use this appendix as a resource for providing additional context to the
report’s text and data tables. Wherever possible, information was provided by each NCANDS
state contact and uses state terminology.
Appendix d: State Commentary 136
Child Maltreatment 2022

timeframe requirements for investigation completions due to the pandemic for FFY 2021.
Response time, as reported in the Agency File, is taken from the calculated average response
time reported in the Child File.
During FFY 2019, the mapping for caregiver and child risk factors was modied to improve
NCANDS reporting accuracy and completeness.
During FFY 2020, mapping updates were focused around improving reporting for services
for clients. Additionally, updates were created for the service date code to successfully report
service dates within the timeframe specied by NCANDS.
During FFY 2021, coding and mapping updates were completed for child and caregiver risk
factors. And more work that was initiated in FFY 2020 was completed around capturing
appropriate service referrals. Also, coding was updated to improve reporting around perpe-
trator prior abuse.
During FFY 2022, coding and mapping updates were completed for reporting deaths due to
maltreatment. Also, coding was updated to improve reporting around child risk factors.
Children
During FFY 2019 additional elds were added to the state system and NCANDS data
extraction codes were modied to further improve accuracy and completeness of CARA-
related data. Fields to document CARA-related services are available on the system. Workers
are required to document plans of safe care in the system. Reports are generated to monitor
completion of these requirements.
During FFY 2021, the state did not modify its policies related to conducting investigations
and assessments. The state has continued to conduct face-to-face assessments and investiga-
tions. The policy requirements regarding timeframes to complete investigations did not
change during FFY 2021.
Alcohol abuse and drug abuse can both be documented independently as a child risk factor
and as a caregiver risk factor in the CCWIS system.
Fatalities
Child maltreatment fatalities reported to NCANDS are those children for which the
Department has investigated the child death. The circumstances of the child fatality are
entered into our CCWIS system as a CA/N report. Coroners, LEA and Medical Examiners
are legislatively mandated reporters.
For FFY 2022 all state child fatalities are reported in the Child File. Alabama’s Child Death
Review Team continued to meet during the pandemic. The meetings had been conducted
virtually prior to the pandemic, so no interruption due to social distancing requirements
occurred.
The FFY 2022 number of child fatalities was 38, an increase of 3 from FFY 2021. The
majority of child fatality investigations which are indicated are suspended for due process
Alabama (continued)
Appendix d: State Commentary 137
Child Maltreatment 2022

or criminal prosecution. This extends the length of the investigation, which can take several
months or years to complete. For the 38 fatalities reported in FFY 2022, the actual dates of
death occurred in a ve-year range, from FFY 2017–2021.
Perpetrators
Alabama state statutes do not allow a person under the age of 14 years to be identied as
a perpetrator. These reports are addressed in an alternate response. On-going services
are provided as needed to the child victim and the child identied as the person allegedly
responsible.
Alabama reports both caregiver and non-caregiver perpetrators of sex trafcking to
NCANDS.
Services
For foster care services, Alabama CCWIS does not require the documentation of the petition
or identity of the court-appointed representative. Petitions are prepared and led according
to the procedure of each court district. All children entering foster care are appointed by the
court a guardian ad litem, who represents their interests in all court proceedings. The state’s
CCWIS does not require the tracking of out of court contacts between the court-appointed
representative and the child victims. Improvement in data quality will require staff training
in this area.
The NCANDS category of the number of children eligible for referral to agencies providing
early intervention services under Part C of the IDEA is the number of children who had
indicated dispositions during FFY 2022 and were younger than 3 years. The NCANDS
category of the number of children referred to agencies providing early intervention services
under Part C of the IDEA is the number of referrals the agency providing services reported
receiving during FFY 2022.
Many services are provided through contract providers and may not be documented through
our CCWIS system. However, enhancements were made to the system in FFYs 2019–2021
to better capture services provided, including those that may not use the system to initiate
payments.
Alabama (continued)
Appendix d: State Commentary 138
Child Maltreatment 2022

Alaska
Contact Susan Cable Phone 907–465–2203
Title Research Analyst II, Ofce of Children’s Services Email
Address Department of Health and Social Services
P.O. Box 112631
Juneau, AK
99811-2631
General
The State of Alaska utilizes a single child welfare information system, the Online Resource
for the Children of Alaska (ORCA), which was previously designated as a Statewide
Automated Child Welfare Information System (SACWIS). In 2018, Alaska declared ORCA
as a transitional Comprehensive Child Welfare Information System (CCWIS) under CCWIS
regulations. All NCANDS data is entered into and then transmitted from, ORCA.
The Child Protection Practice Model of Alaska focuses on those families where a formal
intervention by the state is necessary. This model emphasizes a strengths-based, family-
centered approach through the standardization of information gathering, enhanced assess-
ment and critical thinking skills by the Child Protection (CP) staff. Decisions regarding
needed interventions with families are based on thorough processes for initial and ongoing
assessment of safety, risk, and protective factors. The CP program serves families who are
identied as having children who are “unsafe” or at “high risk” for future maltreatment.
The state of Alaska does not utilize differential response, however, we work closely with our
tribal partners on every protective service report received that includes an Alaska Native or
American Indian Child.
Reports
The State of Alaska NCANDS submission includes all children reported to be victims of
physical injury, sexual abuse, sexual exploitation, neglect, or mental injury including those
that can later be determined to be screened out for assessment. The reporter may identify
him or herself or be anonymous and reports are accepted by phone, letter, fax, e-mail, or
in person. A Protective Services Report (PSR) may be screened in when the information
received indicates a child may be unsafe or is at high risk of harm by a primary caregiver,
parent, custodian, or guardian. There are three levels of screen in;
1) Priority 1 must be responded to as soon as possible but no later than 24 hours of the time
the report is received by OCS.
2) Priority 2 must be responded to no later than 72 hours of the time the report is received
by the OCS.
3) Priority 3 must be responded to within seven days of the time the report is received by
the OCS.
NCANDS data from the past ve years shows a continual decrease in reports screened
in. Although Alaska continues to research the reason behind this trend, two factors which
contribute to the decline is the reduction in children enrolled in public school and a policy
change in the screening of Priority 3 level reports, more clearly dening high risk screening,
so some reports which would previously have been screened in for 7-day response are now
being screened out.
Appendix d: State Commentary 139
Child Maltreatment 2022

Although it did not affect the number of reports received, it is noted that an unprecedented
worker turnover rate of 60 percent for front-line, case-carrying staff, was seen in FFY 2022.
In Alaska, workforce data is calculated using full-time equivalents (FTE).
Children
Alaska completes a safety assessment on all child victims, their siblings, and any other chil-
dren in the home, regardless of if they were noted as victim or not. In FFY 2022, there was a
decrease in the number of children reported as possible abuse or neglect victims as compared
to the previous year. Similarly, the number of substantiated victims decreased as well.
In alignment with federal guidance, in 2020, specic data indicators on sex trafcking were
added to both the initial Protective Service Report and the Initial Assessment. Reports are
made to law enforcement if any sex trafcking is suspected and all youth who go on runaway
status are then assessed for potential trafcking once found. Furthermore, the State of
Alaska has a process for reporting to the National Center for Missing and Exploited Children
(NCMEC) and the National Crime Information Center (NCIC).
Fatalities
In the State of Alaska, the authority for child fatality determinations resides with the Medical
Examiner’s Ofce, not the child welfare agency. The Medical Examiner’s Ofce assists the
state’s Child Fatality Review Team in determining if a child’s death was due to maltreatment.
A child fatality is reported only if the Medical Examiner’s Ofce concludes that the fatal-
ity was due to maltreatment. For NCANDS reporting, fatality counts are obtained from a
member of the Child Fatality Review Team and reported in the NCANDS Agency File.
Perpetrators
Alaska does not have a limitation on how young a perpetrator can be; however, the
state is currently looking into ways to better document child-on-child abuse.
The NCANDS category “other” perpetrator relationship includes perpetrators who are
not primary or secondary caregivers to the child (i.e., non-caregivers) such as a stranger
or adult who does not live in the home and does not normally have access to the child.
Services
The State of Alaska does not document services provided to families in the CCWIS,
however, we partner with our tribal entities to provide preventative and ongoing services
to the families we serve. In 2017, the State of Alaska and eighteen Tribal Co-signers,
representing a total of sixteen tribes, signed the Tribal Welfare Compact. Services provided
via the Compact include Initial Diligent Relative Searches, Ongoing placement searches,
Licensing Assistance, Safety Evaluation of an Unlicensed Relative Home, Family Contact,
Primary and Secondary Prevention.
A pilot program for Plans of Safe Care with the Department of Public Health is currently
underway. Once an evaluation of effectiveness of the program has been completed, the Ofce
of Children’s Service will work to implement a mechanism to track Plans of Safe Care within
the CCWIS.
Alaska (continued)
Appendix d: State Commentary 140
Child Maltreatment 2022

Arizona
Contact Andrew Egge Phone 602-255-2744
Title Information Technology Manager, Reports and
Statistics
Email
andrew[email protected]
Address Arizona Department of Child Safety
AZ Department of Child Safety
P.O. Box 6030
Site Code C010-14
Phoenix, AZ 85003–6030
General
The le for 2021 reporting period had both code and replicated data issues, several of which
have been resolved in the 2022 le. The change from 2021 le is due primarily to improve-
ments to the 2022 le. Specic improvements include: 1. modied code logic to include all
children in Intakes within an investigation closed in the reporting period (given the depen-
dency that an investigation may not be closed until all ndings are entered, and which yields
the earliest date all ndings are entered); 2. included children with missing birthdates, and; 3.
resolved missing Intake ID, Assessment ID, and Removal Details replicated data issues.
Reports
The Hotline continued to answer calls as normal, with no changes to hours or stafng levels.
The department’s call center and child safety specialists are all full- time employees. These
services are not contracted out. DCS has a set of criteria to determine if a communication
(intake) qualies as a report of abuse or neglect according to the denitions in Arizona
statute. If an intake meets the criteria to be a report of abuse or neglect, the staff determines
if the report is in the Jurisdiction of DCS. If not, the information is sent to the correct
Jurisdiction, such as an American Indian tribe. If the report falls under DCS jurisdiction, it is
nalized and sent to the Field to begin the assessment (investigation).
Children
DCS received over 8,000 more reports in 2022 when compared to 2021. On the over 8,000
reports there was an increase of approximately 9,000 more children. This trend aligns with
the re-opening of schools and other mandatory reporting sources impacted by COVID. The
2022 counts also align with 2019 (pre-Covid) counts.
All children in the home are assessed if the intake meets the criteria for a report, includ-
ing children who are not the subject of the current allegations. We are able to distinguish
between alcohol and drug risk factors.
The Guardian system has made IPSE (also referred to as substance exposed newborns) an
allegation type. We did not report Safe Care Plan information this reporting period. Our
business team will review this element to determine if a change is needed for the next report-
ing period.
Perpetrators
DCS maps 2 values to this element for reporting “Other”. “NON-RELATIVE” (available in
the CHILDS System) and “Other Adult” (available in the Guardian System). When this is
the relationship indicated, we map the value to “other”. DCS does not report non-caregiver
perpetrators to NCANDS.
Appendix d: State Commentary 141
Child Maltreatment 2022

Services
In July 2021 DCS offered a new service array. Parent Aide and Family Preservation Services
were no longer offered as part of contracted services after July 2021. DCS now provides
Family Connections, and Nurturing Parenting Program which are available to all families
whether the children are In-Home or Out of Home care. In SFY 2022, MIECHV was reduced
from $3.8M to $2.4M.
DCS has both outsourced services and services provided by the Department as well as
services provided by other child serving state agencies. As of April 2021, DCS integrated
health care for youth in Out Of Home care providing physical, dental and behavioral health
services through Arizona’s Medicaid health plan specically for youth in foster care.
Arizona (continued)
Appendix d: State Commentary 142
Child Maltreatment 2022

Arkansas
Contact Nellena Garrison Phone 501–320–6503
Title DCFS Information Systems Manager
Department of Human Services
Email
nellena.garrison@dhs.arkansas.gov
Address Ofce of Information Technology
108 E. 7th Street, Donaghey Plaza North, 3rd Floor
Little Rock, AR 72201
General
The following options are available when accepting a referral:
■ Refer to DCFS for Fetal Alcohol Spectrum Disorder Assessment (R/A-FASD): The
following change was made to Arkansas legislation effective July 2011—Act 1143 requires
health care providers involved in the delivery or care of infants to report infants born and
affected by Fetal Alcohol Spectrum Disorder. The Department of Human Services shall
accept referrals, calls, and other communication from health care providers involved in
the delivery or care of infants born and affected with FASD. The Department of Human
Services shall develop a plan of safe care of infants born with FASD. The Arkansas State
Police Hotline staff used the Request for DCFS assessment for FASD. These were auto-
matically assigned to the DCFS Central Ofce FASD Project Unit to complete the assess-
ment and closure. The R/A-FASD Assessment was updated and integrated with a new
Refer to DCFS for N. I. Substance Exposure (R/A-SE) Assessment type during FFY 2020.
■ Refer to DCFS for N. I. Substance Exposure Assessment (R/A-SE): Arkansas legisla-
tion effective July 2019—Act 598 requires healthcare providers involved in delivery or
care of infants reporting an infant born and affected by Fetal Alcohol Spectrum Disorder
(FASD) (the previous requirement), and adds infants born and affected by maternal
substance abuse resulting in prenatal drug exposure to an illegal or a legal substance,
or withdrawal symptoms resulting from prenatal drug exposure to an illegal or a legal
substance to that list. Refer to DCFS Newborn Infant Substance Exposure Assessments do
not have allegations of maltreatment at the time of the Referral.
■ Referrals regarding substance exposed infants would be screened out for the follow-
ing circumstances:
• If reported by persons other than medical personnel,
• If the referral is a duplicate and an investigation already is opened,
• If the mother tests positive during her pregnancy but not at birth, or
• If the Health Care Provider can conrm the mother’s prescription for the drug causing
the positive screening.
For FFY 2021 the Request for Assessment Refer to DCFS for N.I. Substance Exposure
(R/A-SE) was included in the data. The R/A-SE Assessment Type was added to the
NCANDS logic as an Alternative Response Referral for FFY 2021. The R/A-SE
Assessments are mapped to the NCANDS category of alternative response nonvictim.
Clients under 1 year old who meet the other dened criteria are counted for any RA-SE
Assessment Type:
• FASD
• Substance Use Resulting in Prenatal Exposure
• Withdrawal Symptoms Resulting From Prenatal Exposure
■ Refer to CACD for Death Assessment (R/A-DA): Arkansas FFY 2015 legislation man-
dated per Act 1211, the Department of Human Services and Arkansas State Police Crimes
Against Children Division (CACD) will conduct an investigation or death assessment
upon receiving initial notication of suspected child maltreatment or notication of a child
Appendix d: State Commentary 143
Child Maltreatment 2022

death. This was effective in Children’s Reporting Information System (CHRIS) August
2, 2015. The Child Abuse Hotline will accept a report for a child death if a child has died
suddenly and unexpectedly not caused by a known disease or illness for which the child
was under a physician’s care at the time of death, including without limitation child deaths
as a result of the following:
• Sudden infant death syndrome;
• Sudden unexplained infant death;
• An accident;
• A suicide;
• A homicide; or
• Other undetermined circumstance
All sudden and unexpected child deaths will be reported to the Child Abuse Hotline.
Death Assessment (DA) reports are accepted by the Hotline and do not have allegations of
maltreatment at the time of the Referral. The data for R/A-DA reports are not submitted
to NCANDS. If the incident does rise to the level of a child maltreatment investigation,
then the Referral will be elevated to be investigated. Child Death Investigation reports are
accepted by the Hotline and will have maltreatment allegations at the time of the referral.
■ Accept for Investigation: Reports of child maltreatment allegations will be assigned
for child maltreatment investigation pursuant to Arkansas Code Annotated 12-18-601.
Arkansas uses an established protocol when a DCFS family service worker or the
Arkansas State Police Crimes Against Children Division investigator conducts a child
maltreatment assessment. The protocol was developed under the authority of the state
legislator, (ACA 12-18-15). It identies various types of child maltreatment a DCFS family
service worker or an Arkansas State Police Crimes Against Children Division investigator
may encounter during an assessment. The protocol also identies when and from whom an
allegation of child maltreatment may be taken. The worker or investigator must show that
a preponderance of the evidence supports the allegation of child maltreatment. The data
for these reports are submitted to NCANDS.
■ Accept for Differential Response: Differential response (DR) is another way of respond-
ing to allegations of child neglect. DR is different from DCFS’ traditional investigation
process. It allows allegations that meet the criteria of neglect or physical abuse that
occurred at least one year from the Referral Date to be diverted from the investigative
pathway and serviced through the DR track. DR is designed to engage low- to moderate-
risk families in the services needed to keep children from becoming involved with the
child welfare system. Counties have a differential response team to assess for safety,
identify service needs, and arrange for the services to be put in place. FFY 2013 was the
rst year the state submitted differential response data to NCANDS. Differential Response
Referrals are mapped to Mapped to the NCANDS category of alternative response
nonvictim.
Reports
On September 6, 2022, the Arkansas Mandated Reporter Portal (MRP) went live. This is
a new public-facing website that mandated reporters can create an account and submit a
child maltreatment report using a new secure online portal. The new website is designed to
be user-friendly and easy to learn. If there are any questions, the portal includes a step-by-
step video to walk the user through the process of submitting online. This new portal has
been created in addition to the hotline for reporting suspected child abuse and neglect. The
Arkansas (continued)
Appendix d: State Commentary 144
Child Maltreatment 2022

Arkansas Child Abuse Hotline remains accessible. Once a referral is submitted through the
MRP, the information transfers directly into the current case management system CHRIS for
the ASP Hotline staff to complete the Referral determination. For the period September 6,
2022 through September 30, 2022 (end of FFY 2022), there were 2,244 Referrals submitted
through the MRP.
Children
All children in the home are assessed during the investigation process.
Fatalities
The Arkansas Division of Children and Family Services receives notice of child fatalities
through the Arkansas Child Abuse hotline. The reports include referrals from mandated
reporters such as, physicians, medical examiners, law enforcement ofcers, therapists, and
teachers, etc. A report alleging a child fatality can also be accepted from a non-mandated
reporter. Non-mandated reporters include neighbors, family members, friends, or members
of the community. The guidelines for reporting are mandated and non-mandated persons are
asked to contact the child abuse hotline if they have reasonable cause to believe that a child
has died as a result of child maltreatment.
All sudden and unexpected child deaths will be reported to the Child Abuse Hotline. Death
Assessment (R/A-DA) reports are accepted by the Hotline and do not have allegations of
maltreatment at the time of the Referral. The data for R/A-DA reports are not submitted to
NCANDS. If the incident does rise to the level of a child maltreatment investigation, then the
Referral will be elevated to be investigated. Child Death Investigation reports are accepted
by the Hotline and will have maltreatment allegations at the time of the referral. All Child
Death Investigation reports are included in the Child File data submission.
Perpetrators
An alleged offender must be fourteen years of age or older. For sexual abuse allegations by
an alleged offender under fourteen years old, a role in referral is selected of “Alleged Juvenile
Offender-Under Age Fourteen” and Findings of “Exempted (Underage Juvenile Offender
at Time of Incident)” for the applicable sexual abuse allegations that were found to have a
preponderance of evidence to support a True Finding.
The following values are mapped to NCANDS code ‘other’ perpetrator relationship: Client,
Life Connection, Live-In, No Relation, Peer, Signicant Other, and Student.
Arkansas accepts reports of Sex Trafcking by adult non-caregiver offenders 18 years of age
or older. This data is reported to NCANDS in the Child File.
Services
Arkansas continued to use the additional funding provided through the Relief Bill
promoting Safe and Stable Families. The Intensive In-Home Services funding source will
no longer be utilized for Safe and Stable Families for FFY 2023. The state outsources
some contracted services such as Parenting Training and Substance Abuse Treatment.
Arkansas (continued)
Appendix d: State Commentary 145
Child Maltreatment 2022

California
Contact Christina Hoerl Phone 916–651–0229
Title Section Chief, Data Analytics Bureau Email
Address California Department of Social Services
744 P Street, MS 8–05–656
Sacramento, CA 95814
General
California made a number of coding changes for the Child File to account for updates to
our statewide child welfare information system and to ensure alignment with the NCANDS
mapping instructions. Data reported in the services section of the Child File has changed the
most from last year as a result. More specically, we:
■ Adjusted our coding to only count services if they continued past the client disposition. This
resulted in a lower number of children being reported with services compared to Federal
Fiscal Year (FFY) 2021. This also resulted in a decrease in the percent of children reported
with Case Management services and an increase in the percent of children reported with this
service as unknown or missing.
■ Updated our coding to account for updates to our statewide system that capture Family
Preservation Services, as well as include children already in a case with a service compo-
nent of Family Maintenance, resulting in an increase in the percent of children reported
with those services and a decrease in the percent of children reported with this service as
unknown or missing.
■ Updated our coding to account for updates to our statewide system that capture Family
Planning Services, resulting in this item being changed from Not collected/Not applicable
to reportable and a large increase in the percent of children with this service as unknown or
missing.
■ Updated our coding to account for updates to our statewide system that capture Health-
Related and Home Health Services, resulting in an increase in the percent of children
reported with this service and a decrease in the percent of children with this service as
unknown or missing.
■ Re-coded services in our system that used to map to Employment Services and to Home-
Based Services to other NCANDS categories, resulting in no services being mapped to
Employment Services or Home-Based Services (now reported as Not collected/Not appli-
cable) and a decrease in the percent of children with those services as unknown or missing.
■ We also developed methodologies and began reporting on Agency File items #3.1, 4.3, and 5.2.
California’s differential response approach is comprised of three pathways:
■ Path 1 community response—family problems as indicated by the referral to the child
welfare system do not meet statutory denitions of abuse and neglect, and the referral is
evaluated out by child welfare with no investigation. But based on the information given at
the hotline, the family may be referred by child welfare to community services.
■ Path 2 child welfare services with community response—family problems meet statutory
denitions of abuse and neglect, but the child is safe, and the family has strengths that can
meet challenges. The referral of suspected abuse and neglect is accepted for investigation by
the child welfare agency, and a community partner goes with the investigator to help engage
the family in services. A case may or may not be opened by child welfare, depending on the
results of the investigation.
■ Path 3 child welfare services response—the child is not safe and at moderate to high risk
for continuing abuse or neglect. This referral appears to have some rather serious allegations
Appendix d: State Commentary 146
Child Maltreatment 2022

at the hotline, and it is investigated, and a child welfare services case is opened. Once an
assessment is completed, these families may still be referred to an outside agency for some
services, depending on their needs.
Reports
As a result of COVID-19 restrictions easing and children returning to in-person learning,
the number of calls to the child welfare hotline have increased, but not yet returned to pre-
pandemic levels. There was an increase of about 7 percent. For FFY 2022 compared to 2021,
The greatest gain was seen in reports made by education personnel.
The report count includes both the number of child abuse and neglect reports that require,
and then receive, an in-person investigation within the time frame specied by the report
response type. Reports are classied as either immediate response or 10-day response. For
a report that was coded as requiring an immediate response to be counted in the immediate
response measure, the actual visit (or attempted visit) must have occurred within 24 hours
of the report receipt date. For a report that was coded as requiring a 10-day response to
be counted in the 10-day response measure, the actual visit (or attempted visit) must have
occurred within 10-days of the report receipt date. For the quarter ending September 2022,
the immediate response compliance rate was 94.7 percent, and the 10-day response compli-
ance rate was 86.1 percent.
Children
The California Department of Social Services (CDSS) has policies to investigate/assess all
children in a household if any child in the household has a maltreatment allegation. First, the
investigating social worker performing the initial investigation must determine the potential
risks to the child, or any child in the family or household, and have in-person contact with all
the children alleged to be abused, neglected, or exploited. If the social worker nds that the
referral is not unfounded, they must conduct an in-person investigation with all children present
at the time of the initial in-person investigation. It is then at the discretion of the county to
decide whether to conduct an in-person investigation with any additional children who were not
present at the initial in-person investigation. In our statewide child welfare information system,
we have an allegation type of “At Risk, Sibling Abused.” This allegation type is reported to
NCANDS as “No alleged maltreatment.”
System changes to capture the Comprehensive Addiction and Recovery Act of 2016 (CARA)
related elds (substance exposed infants, creation of plans of safe care, and referral to appropri-
ate services) were completed in July 2020 and data entry guidance was released to counties in
November 2020. Our analyses have found that there are a high number of plans of safe care
and referrals to services entered into our system which originate from reports not provided by
medical professionals, and many of these are notated as “other” reporters. While we do not
expect that 100 percent of our plans of safe care and referrals to services will originate from
reports made by medical professionals, it is likely at least some of the reports made by “other”
sources could be more accurately entered as medical professionals. We will continue to work
with counties to accurately enter report sources.
While the system changes to capture CARA related data improved NCANDS reporting of alco-
hol and drug abuse child risk factors for infants, there are instances where we cannot separate
California (continued)
Appendix d: State Commentary 147
Child Maltreatment 2022

alcohol abuse from drug abuse. When our data indicates that an infant has a substance expo-
sure type of “Substance Abuse,” “Withdrawal Symptoms,” or “Other,” the child is reported as
having both alcohol abuse and drug abuse, as instructed in the Child File Codebook. We hope
to address this limitation and other opportunities for data improvement in the coming years.
While California’s system has existing elds to capture caregiver drug and alcohol abuse, as
well as drug and alcohol abuse for children who are not infants, these elds are seldom used,
resulting in very low counts of caregiver risk factors especially. California will be implement-
ing a system change in March of 2023 to collect drug and alcohol abuse data for all clients and
caregivers in all investigated referrals to improve reporting to NCANDS. These elds will
need to be completed for every client in a referral before the referral can be closed. While it’s
expected that the addition of these elds, and the requirement that they be completed before
closing a referral, will improve the completeness of data on client risk factors, it is likely a
number of responses will be reported as “Unable to Determine,” which is being added to allow
users exibility when they do not know for certain whether a risk factor is present or not.
CDSS has a policy to track commercially sexually exploited (CSE) youth referrals with an
allegation of “Exploitation.” CSE allegations are entered in one of two ways: rst, by choosing
“Exploitation” and, to differentiate this from other exploitation referrals, with the sub-category
of “Commercial Sexual Exploitation;” second, by choosing “General Neglect” with a sub-
category of “Fail/Unable to Protect from CSE.” There is a limitation with these data, however.
Only when the allegation is substantiated can the sub-categories be entered. Thus, inconclusive
CSE allegations are not reported as CSE.
Fatalities
Fatality data submitted to NCANDS is derived from notications (SOC 826 forms) submitted
to the CDSS from County Child Welfare Services (CWS) agencies when it has been deter-
mined that a child has died as the result of abuse and neglect, as required by SB 39, Chapter
468, Statutes of 2007. The abuse and neglect determinations reported by CWS agencies are
made by local coroner/medical examiner ofces, law enforcement agencies, and/ or county
CWS/probation agencies. As such, the data collected and reported via SB 39 and used for
NCANDS reporting purposes reects child death information derived from multiple sources. It
does not, however, represent information directly received from either the state’s vital statistics
agency or local child death review teams.
The data is used to meet the reporting mandates of the federal Child Abuse Prevention and
Treatment Act (CAPTA) and for the Title IV-B, Annual Progress and Services Report (APSR).
Calendar Year (CY) 2021 is the most recent validated annual data and is therefore reported for
FFY 2022. It is recognized that counties will continue to determine causes of fatalities to be
the result of abuse and/or neglect that occurred in prior years. Therefore, the number reected
in this report is a point in time number for CY 2021 as of December 2022 and may change if
additional fatalities that occurred in CY 2021 are later determined to be the result of abuse and/
or neglect. For fatalities that occurred while the child was in foster care, the perpetrator infor-
mation is unavailable until full case reviews of CY 2022 critical incidents are concluded. Any
changes to this number will be reected in NCANDS trends analyses, through resubmissions,
as well as subsequent year’s APSR reports.
California (continued)
Appendix d: State Commentary 148
Child Maltreatment 2022

With the enactment of SB 39, the CDSS determined that the data provided through the SB 39
reporting process would provide not only more current information regarding child maltreat-
ment deaths in California than the reconciliation audit conducted by CDPH, but would also
provide data from multiple agency sources providing more reliable data for NCANDS. As a
result, beginning with the FFY 2010 NCANDS data submission in CY 2011, the CDSS changed
the data source to the SB 39 data. It is important to note that while SB 39 data were used in the
FFY 2022 NCANDS submission, the data were derived from CY 2021. Additionally, beginning
in CY 2012 CDSS began to receive reports of fatalities determined to be the result of abuse and
neglect and caused by an unknown third party where a parent or caretaker did not contribute
to the child’s death. NCANDS submissions of FFY 2013 (CY 2012) forward includes such
fatalities.
Perpetrators
California does not have a limit on how young a perpetrator can be. The following is an
excerpt from guidance released by the California Department of Social Services in All
County Letter 17-85:
Circumstances may arise where the abuse or neglect occurs within the home, but the perpe-
trator is a non-parent under the age of 18. The county hotline screener must still assess any
referral indicating a possible failure or inability to protect involving the parent that places
the child at risk. The county, in consultation with county counsel and at its discretion, may
choose to investigate and substantiate an allegation involving a minor perpetrator. When
doing so, best practice indicates that the county considers several factors including, but not
limited to, the following:
■ The relationship between the perpetrator and the victim.
■ The ages and developmental levels of the perpetrator and victim.
■ Whether the action constitutes developmentally normal behavior (i.e., sexual exploration
between two pre-school aged children, or physical aggression between siblings, if the
behavior was not extreme and the parents responded appropriately).
■ If the perpetrator has the developmental ability and capacity to understand the gravity of
his or her actions or acted with willful disregard to the danger, pain or fear of the other
child.
■ The severity and frequency of the alleged abuse.
■ If the action negatively affects the long-term safety and well-being of either child.
Relationship types of “Indian Custodian” (where the child is an Indian Child), “Live In,” and
“No Relation” are included in “other” perpetrator relationship.
Services
Prevention services in California are implemented through a state-supervised, county
administered system. This system has the advantage of allowing the 58 counties in California
exibility to address child abuse prevention efforts through a community based local lens.
This approach, however, results in 58 sets of challenges in program implementation, evalu-
ation, data collection, and reporting. Federal funding is allocated to each county to support
a variety of prevention services. Federal funding streams targeted for prevention services
include Community-Based Child Abuse Prevention (CBCAP), Promoting Safe and Stable
Families (PSSF), Child Abuse Prevention and Treatment Act (CAPTA), and Child Abuse
California (continued)
Appendix d: State Commentary 149
Child Maltreatment 2022

Prevention, Intervention and Treatment (CAPIT). The Ofce of Child Abuse Prevention
(OCAP) is responsible for monitoring federal expenditures as well as ensuring counties are
evaluating the quality of programs consistently. Since the State Fiscal Year (SFY) and the
FFY are not aligned, information for SFY 2021–22 is representative of FFY 2022.
On January 25, 2021, the Regional Stay at Home Order was lifted by the California
Department of Public Health for all regions within California. These organizations have been
able to resume in-person service delivery or provide a hybrid option which includes virtual
or in-person services. As providers and families adjusted to a virtual platform for service
delivery, there was a recognition that virtual services offered a level of convenience which
encouraged participation by families that traditionally were unable to engage in services.
Although the virtual platform allows for exibility, one of the on-going challenges providers
continue to face is staff shortages and high turnover rates.
On January 8, 2021, Governor Gavin Newsom announced a state budget proposal that
included critical supports for Family Resource Centers (FRCs) to respond to the COVID-19
pandemic. Specically, the measure proposed $7 million in General Funds in SFY 2020-21
and $6 million in General Fund for SFY 2021–22 for COVID-19 related supports for child
welfare services. Throughout SFY 2021–22, 95 lead agencies, and a total of 375 FRCs,
received supports from the relief funds. FRCs reported most funds went towards concrete
supports for families. Many of the funds went towards stafng for FRCs to provide continued
direct services for families. FRCs continue to report an increased need in concrete supports,
hiring staff to meet service and business needs, and staff training.
Governor Newsom provided General Funds for the creation of a parent, caregiver, and
youth remote helpline to support families with stressors arising from the pandemic. The
OCAP contracted with Parents Anonymous to provide remote support to families through
text support, live chats, resource coordination, and virtual support groups across the state
of California. In SFY 2021–22, Parents Anonymous continued to provide such services,
responding to 17,019 calls. Parents Anonymous has consistently seen a rise in the need of
connections to concrete supports and additional assistance for families and individuals in
remote locations.
In 2021, the American Rescue Plan Act (ARPA) under CBCAP provided $29,667,177 in fund-
ing, of which $25,000,000 was provided to counties to provide direct services to families.
CBCAP ARPA funding was released in the form of grants through the OCAP in the amount
of $4,667,177. The ARPA under CAPTA provided $12,063,503 in funding that was provided
in the form of grants through the OCAP. Request for Applications (RFAs) were developed
in SFY 2021-22 for 3 grant series: Father Engagement, Strong Communities, and Planting
Prosperity. The Father Engagement grant will provide father-specic case management and
evidence-informed/-based services through eight grants. The Strong Communities grant
will award eight grantees to expand FRCs. Lastly, the Planting Prosperity grant will provide
funds to 10 agencies to develop innovative primary and secondary prevention services
throughout California.
Each year the CDSS also allocates prevention funding directly to counties for disbursement.
This information is gathered in a data collection system funded by the OCAP.
California (continued)
Appendix d: State Commentary 150
Child Maltreatment 2022

In 2022, the OCAP transitioned from utilizing Efforts to Outcomes (ETO) software system
for data collection and reporting to Apricot Social Solutions. Over the past four years, the
OCAP requested counties select one unit of measure (children, parents/caregivers, or fami-
lies) for service counts instead of multiple units of measure for one service activity to reduce
duplicative service counts. This request has led to some improvements in the way informa-
tion is captured, however, in some instances counties are changing the unit of measure
collected from year to year so it is difcult to compare service counts. Discrepancies between
service counts from year to year may be attributed to changes in vendor contracts, evaluation
methodologies, and/or the transition from in-person services to a virtual platform. To the
best of OCAP’s knowledge, the data collected for children, parents, and families is mutually
exclusive.
For SFY 2021–2022, the OCAP included a question about completion rates. This informa-
tion provides insight as to the relative success of a program or intervention’s engagement
strategy. The OCAP recognizes that completion rates alone are not indicative of improved
long-term outcomes, however, this information provides a baseline understanding of the level
of engagement and participation in the program or intervention which is one step towards a
successful outcome.
For SFY 2021–22, counties reported 5,101 parents/caregivers served by CAPIT funding,
5,707 parents/caregivers served by CBCAP funds, and 18,082 parents/caregivers served by
PSSF funding. The data indicates that counties served more children using PSSF funding in
SFY 2021-22, than in previous scal years. There are several potential factors that may have
contributed to the increase in the number of children served in SFY 2021-22, these include:
■ Improved data collection methodology.
■ In-person services and activities have resumed since COVID-19 restrictions have been
lifted.
■ Flexibility of the virtual platform which eliminates the barriers associated with transporta-
tion and childcare.
■ Changes to the unit measured (counties may have selected to measure parent service
counts in the previous reporting period, and in SFY 2021–22 chose to collect data based
on the child for the same intervention).
■ Increases in the number of contracted staff in some counties.
■ Increased technical assistance support early in the reporting period by OCAP Consultants.
There are several factors that may be associated with a decrease in the number of children
served using CAPIT and CBCAP funding and these include:
■ Counties corrected inaccuracies in reporting from the prior scal year
■ Lower rates of referrals to children and family support services
■ Changes in way service counts were measured (children, parents/caregivers, families)
■ Changes to service provider contracts (termination of contracts) or new programs started
during the middle of the scal year therefore not capturing total numbers served for the
entirety of the scal year
■ Signicant number of resignations across agencies and it has been difcult hiring qualied
staff which has led to the inability of providers to serve as many or more children, parents,
and families
■ Other challenges, such as concerns with resurgence in COVID-19 cases
California (continued)
Appendix d: State Commentary 151
Child Maltreatment 2022

In SFY 2021–22, twelve counties reported a decrease in the number of children served with
CAPIT dollars compared to SFY 2020–21.
The Celebrating Families! (CF!) grant funded with $51,769 in CAPTA funds allowed
Prevention Partnership International (PPI) to provide train-the-trainer training and technical
assistance to agencies who will be administered the Celebrating Families! program. The
trained agencies planned to each reach at least 10-15 families in their respective sites in the
third year of the grant. The families served are at risk for experiencing child abuse/neglect,
or family violence due to substance use disorders and other adverse childhood experiences.
A Year Two evaluation was completed for CF! and it was reported that though training and
technical assistance to agencies was not largely affected by COVID-19, having the CF! pro-
gram implemented virtually and in-person depending on the changing restrictions affected
the number of families served. Stafng shortages and turnovers also affected program
implementation.
The OCAP continued the Economic Empowerment with three organizations and awarded 10
new organizations committed to support the nancial empowerment of parents and alleviate
the stress of poverty in their communities. This program involves providing supports to
parents using the “Your Money, Your Goals” nancial empowerment toolkit developed by the
Consumer Financial Protection Bureau. A total of $440,410 in CAPTA funds and $376,770
in CBCAP funds was allocated to support the program in SFY 2021-22. In SFY 2021-22,
agencies began transitioning back to an in-person service delivery model while still provid-
ing services virtually, as needed. Special populations that have been served and prioritized
through outreach include:
■ Unhoused or at-risk of homelessness
■ English as a second language caregivers (Main languages include Spanish, Chinese, Farsi,
Russian, etc.)
■ Previously incarcerated caregivers
■ Migrant farmworkers and dayworkers
■ Parents with children ages 0–5
The Road to Resilience grant funding is supported with $7,011,462.30 in Child Abuse
Prevention and Treatment Act (CAPTA) funds. The 12 grantees are composed of collabora-
tive partnerships between community-based and county government agencies. The objective
of the program is to serve pregnant women with known histories of substance use, pregnant
women with current substance use, and mothers of substance-exposed infants, linking them
to services and supports. In SFY 2021-22 Road to Resilience grantees had a total of 778
mothers served.
California (continued)
Appendix d: State Commentary 152
Child Maltreatment 2022

Colorado
Contact Detre Godinez Phone 303–866–5359
Title Federal Analyst and Liaison Email
detre.godinez@state.co.us
Address Colorado Department of Human Services,
Ofce of Children, Youth and Families
1575 Sherman Street
Denver, CO 80203
General
Colorado implemented the new Adoption and Foster Care Analysis and Reporting System
(AFCARS) requirements in the fall of 2022. Implementation of Family First Prevention
Services Act is also underway with adaptation to these new processes. Improvement to
NCANDS data mappings of service and risk factor data were put on hold as improvements
were focused on these changes. NCANDS data will better reect services in Colorado as
CCWIS is modernized and mapping of services and risk factors are improved.
Colorado counties have the option to use Differential Response, which has a dual track
system for screened-in referrals. The referral options are traditional High-Risk Assessments
or a Family Assessment Response for low and moderate-risk referrals. Counties who are not
yet utilizing Differential Response only use High Risk Assessments. Safety and risk assess-
ments are completed for all screened-in referrals. Both tracks are reported to NCANDS.
Reports
There were no changes to policy or interpretation of statute around screening referrals
due to the pandemic. Face-to-face initial contacts and ongoing monthly contacts resumed
with additional measures to standard procedure for safety. Colorado has a hotline system
(1-844-CO-4-KIDS) that remained operational during the pandemic. Difculties in hiring
new staff continues to be an issue in Colorado.
Children
Colorado county agencies conduct face-to-face investigations and assessments as required to
accurately determine safety and risk of children. County workers continue to minimize possible
risks or exposure to COVID by taking additional precautions and maintaining public health
recommendations for protocols including washing hands, self-monitoring health, and minimiz-
ing social interactions and wearing a mask as needed.
Improvements to NCANDS data mappings of child and caregiver risk factor data were put on
hold due to data system modernization and AFCARS changes. Colorado’s child welfare system
does not allow for assessment of prenatal exposure and only for assessment at the time of birth.
Fatalities
Colorado’s Child Fatality Review Team (CFRT) were able to perform reviews.
Perpetrators
Colorado does not make ndings on third party perpetrators of sex trafcking; instead,
the caretakers are evaluated to see if their behaviors are providing access to the third-party
perpetrators.
Child Maltreatment 2022
Appendix d: State Commentary 153

The “other” perpetrator relationships include live-in partners, no relation, signicant other,
signicant other, foster son, foster daughter, teacher, school counselor, spouse (ex), restitu-
tion recipient, child under guardianship, signicant other (ex), neighbor, self, and host home
provider.
Services
In 2021, the Division of Child Welfare began implementing the Family First Prevention
Services Act, which is shifting services toward prevention and creating new avenues for
services. Colorado aims to better reect services in Colorado through CCWIS modernization
and mapping renements of services and risk factors.
Colorado does not outsource any direct child welfare protection services. Some services that
help to support families may be community-based.
Colorado (continued)
Child Maltreatment 2022
Appendix d: State Commentary 154

Connecticut
Contact Fred North Phone 860–817–7462
Title Program Director
Strategic Planning, Data Reporting and Evaluation
Email
Address Department of Children & Families
505 Hudson Street
Hartford, CT 06106
General
The State of Connecticut (CT) Department of Children and Families (DCF) continues to
operate a Differential Response System (DRS). DRS is comprised of two tracks: Child
Protective Services (CPS) Investigations for moderate to high-risk cases, and Family
Assessment Responses (FAR) for low to moderate risk cases (exceptions apply). Currently,
CT does not report data concerning reports handled through a FAR response to NCANDS.
This means that the total number of abuse/neglect reports observed in the NCANDS data is
far lower than the total that we actually receive, accept and respond to each year. We have
also been increasingly utilizing the FAR response, to the point where during FFY 2022 we
used FAR to respond to about 60 percent of all accepted reports, although only 55.5 percent
remained solely a FAR response and did not change tracks to Investigation.
DCF policy did not change with regards to commencement within the designated response
time determined at time of acceptance, or for completion of DRS response within 33 business
days. Inconsistencies with that expectation were documented accordingly.
Reports
During the reporting period 88 Social Worker Trainees began their pre-service training.
DCF’s Academy for Workforce Development certied 114 new child protective services
hires as completing their pre-service training during FFY 2022. The CT DCF Careline is
the agency’s 24/7 centralized point of contact for reporting concerns of child abuse and
neglect. The Careline has maintained continuous operations 24/7/365 throughout the course
of the year. During FFY 2022, Careline continued utilizing a modern cloud-based call center
system (Five9) that allows for social worker screeners to work remotely up to 80 percent
of their schedules, consistent with the statewide labor agreement regarding telework. This
system helps to ensure the health and safety of staff, while maintaining continuous opera-
tions, as pandemic conditions continue. Careline social work screening staff are comprised of
50 full-time staff, and 13 part-time staff (at either 34, 32 or 20 hours per week).
Appropriately, screening calls is a top priority of the DCF Careline and was an area of
quality focus during FFY 2022. Through partnering with the DCF Bureau of Strategic
Planning, an in-depth qualitative review of non-accepted reports was completed. During
the review period more than 4,000 non-accepted reports were reviewed, with only 60 (1.3
percent) returned to Careline management for further review. Careline used this information
to improve performance and provide guidance regarding effective documentation of rationale
for not accepting a report. This review will continue semi-annually to maintain the high
standards established. Another noteworthy Careline accomplishment in FFY 2022 was the
completion of a Careline Continuous Quality Improvement (CQI) Plan and the development
of CQI Teams. The CQI Plan contains key performance indicators that span all Careline
functions, and there are CQI Teams with areas of focus that include screening/response,
training/development and special investigations.
Child Maltreatment 2022
Appendix d: State Commentary 155

CT DCF has also continued to modernize our systems through ongoing enhancements to
our automated reporting portals. Enhancements were made to both the Child Protective
Services (CPS) Background Check and CAPTA Notication portals this year. The CAPTA
Notication portal allows birthing hospitals the ability to le online reports of abuse or
neglect to DCF OR to create a CAPTA Notication for those newborns identied as sub-
stance exposed and consistent with the criteria associated with a notication.
The Careline also implemented a new public facing mandated reporter portal in June 2022.
This portal allows all mandated reporters the ability to le non-emergent reports of abuse/
neglect online, and a training video explaining its use was posted online to help reporters
understand the system. DCF received 7,335 reports through the portal during FFY 2022,
receiving an average of 611 per month, ranging from a high of 812 in March to a low of 375
in August.
There was an 11 percent increase in overall CPS reports received during FFY 2022 compared
to FFY 2021. Every month saw increases when compared to the same month the previous
year, though months that see typical seasonal spikes saw the most increase as well. The
volume of reports received in March, June and December 2022 exceeded that of the pre-
pandemic, and formerly highest volume observed yet, months in 2019. Report volume in
September and November also came close to meeting the same volume for those months in
2019. The types of reporters making calls to the Careline have continued to evolve beyond
pre-pandemic proportions during FFY 2022, particularly with respect to those calling from
schools. In fact, the proportion of calls received from schools continued to rise during FFY
2022. All other groups showed a commensurate decrease in proportion from FFY 2021 to
FFY 2022 during almost all months.
Children
During FFY 2022, there was a 16 percent increase in the number of unique children who were
alleged victims, compared to FFY 2021. This correlates with the almost 20 percent increase in
the number of reports accepted for Investigation observed during this year as reporting contin-
ues to rebound from the pandemic. CT continued to conduct differential responses throughout
the course of this year and had returned to almost entirely in-person responses, with virtual
visitation only utilized when indicated.
Policies and procedures concerning the conducting of all differential responses did not change
during the course of the year. DCF continues to operate a CAPTA portal, which is a web-based
portal for notications of such children by birthing hospitals, which includes the ability to make
online reports of abuse/neglect when indicated. DCF received 1,880 notications through the
CAPTA portal during FFY 2022, of which 42.3 percent resulted in an actual abuse/neglect
report. Further, 71 percent indicated that a Plan of Safe Care had been developed for the child,
and 71 percent referred to appropriate services, as of the time of the notication. Data collected
by the portal is de-identied but does include required elements regarding development of a
Plan of Safe Care and Referral to Appropriate Services. These elds have not been incorporated
into our legacy SACWIS system, as they are planned to be developed in our upcoming CCWIS
system within the next one to two years.
Connecticut (continued)
Child Maltreatment 2022
Appendix d: State Commentary 156

DCF continues to strengthen its response to child victims of human trafcking as we learn
more in CT and across the country. During FFY 2022, DCF saw its largest increase in new
referrals, validating the increased activity by trafckers and demonstrating that the training
continues to improve the state’s identication of child victims. The number of new referrals
last year increased. Each of the six DCF Regions has a Human Antitrafcking Response Team
(HART) team consisting of a HART Lead and Liaison(s) that partner with law enforcement,
service providers and the identied Multidisciplinary Team(s) (MDT). These partnerships
ensure a collaborative response and coordinate services for child victims and their families.
Cases that do not meet the statutory denition of abuse and neglect are coordinated by the
Department’s HART Director in partnership with the relevant MDT(s). The Department’s
Human Trafcking Policy and Practice Guide allows for all cases of suspected child trafcking
be sent directly to the MDT Coordinators.
Fatalities
CT DCF continues to have appointed representatives that are members of, and regularly attend,
the CT Statewide Child Fatality Review Panel meetings. Other members include representa-
tives from the Ofce of the Chief State’s Attorney, Chief Medical Examiner, Child Advocate,
and more. The Child Fatality Review Panel has remained operational during the pandemic,
and no changes were made to policy regarding its operation. We have maintained our monthly
meeting, review data, those specic circumstances related to fatalities and systematic issues.
From these meetings, recommendations are generated for communications, dissemination of
information and other actions as a result. The receipt of child fatality data by the Panel has
also continued from the Ofce of the Chief State’s Attorney, Chief Medical Examiner, Child
Advocate, CT Department of Public Health and other law enforcement or medical entities
without interruption.
Perpetrators
CT Statute denes abuse and neglect as having been committed by a parent/guardian or
entrusted caretaker (see CT CGS 17a-101g). Most of Connecticut’s child trafcking cases are
the result of non-caregiver perpetrators, therefore, are not accepted by DCF Careline. The new
DCF Human Trafcking Policy and Practice Guide that went into effect in August 2021 created
a new pathway for non-accept cases. All calls of suspected child trafcking that are called into
the DCF Careline are reviewed by the HART director and are automatically sent to the state’s
seventeen Multidisciplinary Teams (MDTs) and Human Trafcking Task Force. This process
ensures that every case of suspected child trafcking receives the same access to support,
resources, and legal response despite the limits of state statute. The MDTs have access to the
states specialized providers for this population as well as a wealth of other supports and ser-
vices that can be benecial to the child victims and their families. All child trafcking cases are
documented in the Provider Information Exchange (PIE) data base. PIE data is used for federal
reporting, grant writing, service development, and statewide awareness.
The perpetrator relationship eld is used to capture the relationship between specic alleged
perpetrators and alleged victims. Types of relationships not specied in already dened
values are to be captured using the “Other” perpetrator relationship. Examples of such
relationships often include parents of other children in the family that are not step/adoptive
parents to the alleged victim, parents or relatives of a friend of the alleged victim, and school/
educational setting staff (i.e. janitors).
Connecticut (continued)
Child Maltreatment 2022
Appendix d: State Commentary 157

Services
CT DCF directly provides all Differential Response Services, as well as ongoing Child
Protective and Foster Care/Adoption services. DCF also funds a wide array of contracted
services to meet the ongoing needs of children, youth and families, and are aimed at both
prevention of abuse/neglect, and treatment of behavioral health, parenting skills, independent
living skills and many more. With very few exceptions, DCF modied our service system at
the onset of COVID to minimize non-emergency, in-home or in-person services. Our entire
service array transitioned very quickly to tele-health solutions and maintained a virtual
presence in home and with clients through COVID. With a brief exception during January
and early February 2022, the system has continued to utilize in-person services. Our current
status is that we are fully open to in-person services at this point while utilizing virtual
services when deemed appropriate.
The State of Connecticut has continued to plan for implementation of our Family First
Prevention Plan, developed in partnership with over 400 individuals from state agencies,
community-based providers, advocates, youth and families with lived experiences. What
makes this prevention plan unique is that CT has taken a bold approach to expand access to
prevention services to children and their caregivers “upstream” who present with particular
needs or characteristics that ultimately may result in DCF involvement, as identied through
a community pathway. Family First is being utilized as a tool, as part of Connecticut’s
overall prevention strategy, to assist in building upon an existing infrastructure and its
already diverse array of services and evidence-based programs (EBPs), with the goal to
prevent maltreatment and children entering foster care. DCF has already been funding
two of the services on the approved plan (Multi-Systemic Therapy and Functional Family
Therapy), and our partner agency the Ofce of Early Childhood (OEC) has been funding
three others (Healthy Families America, Nurse Family Partnership and Parents as Teachers).
Connecticut’s vision is to expand upon its collaborative child well-being system through
enhanced focus on prevention and early intervention. We have continued ongoing preparation
for full implementation throughout FFY 2022.
Connecticut (continued)
Child Maltreatment 2022
Appendix d: State Commentary 158

Delaware
Contact Christine Weaver Phone 302–892–6489
Title Data and Quality Assurance Manager
Division of Family Services
Email
Address Delaware Department of Services for Children,
Youth and their Families
1825 Faulkland Road
Wilmington, DE 19805
General
Delaware’s Division of Family Services (DFS) has received an increase in reports of child
abuse, neglect and dependency. In FFY 2022, Delaware received an increase in reports.
Delaware continues to use Structured Decision Making® (SDM) at the report line, in
Investigation, and in Family Assessment Intervention Response (FAIR). By the use of this
evidence- and research-based tool, Delaware is better able to distinguish between cases that
require a full investigation and those that require an assessment or referrals for services
unrelated to child abuse and neglect, to consistently determine safety threats, and to make
decisions using the same set of standards. Delaware has continued our internal FAIR pro-
gramming and maintained our external FAIR contracts. For the current NCANDS reporting
period, Delaware has added internal FAIR data in the Child File. In the near future, we hope
to be able to include external FAIR data as we are building a provider portal to allow our
contracted FAIR services to enter information into our data system. This portal has been
built but is in the testing phase at this time. Delaware has updated juvenile trafcking deni-
tions to assist our intake staff on screening reports and has introduced a Commercial Sexual
Exploitation Identication Tool (CSE-IT).
On February 6, 2018, our new SACWIS system called FOCUS (For Our Children’s Ultimate
Success) went live. This integrated cloud-based system is implemented but remains under
construction. Change requests continue to be built and testing is ongoing. Delaware also
now has added a FOCUS mobile app that allows workers to have access to our data system
and enter specic events more readily from the eld. As we continue to improve FOCUS,
we have tasked ourselves with improving data quality including information used for the
NCANDS report. NCANDS validations are used as a data quality tool to determine areas
of need and improvement. We have added validations to our system to improve data quality
and more accurate reporting. We are in the process of building additional validations to
ensure updated demographics are completed on all investigation case participants. We have
improved our ability to validate case participants more accurately. Delaware has an estab-
lished Continuous Quality Improvement Data Quality Committee that continues to focus on
data quality improvement efforts.
Reports
In FFY 2022, Delaware received 23,537 family and 595 institutional abuse (IA) reports. Of
the reports received, 35 percent, were screened in for an assessment or investigation, a 2 per-
cent decrease as compared to the 37 percent in FFY 2021. Of reports screened in, 53 percent
were diverted through various differential response programs, as compared to 37 percent
in FFY 2021, a 16 percent increase. During the COVID-19 pandemic, the Delaware hotline
remained at full capacity, and we did not alter our screening practice or policy. Delaware did
obtain Dialpad, a cloud-based communication platform to be used for intakes. This allows
hotline staff to have remote capability and ensure that all calls will be answered by a live
hotline worker, eliminating Delaware’s need for an answering service.
Child Maltreatment 2022
Appendix d: State Commentary 159

While 53 percent screened in reports were diverted through various differential response
programs, more than three thousand were screened in for a new investigation and more
than six hundred were linked to an already active investigation. In FFY 2022, Delaware has
overall completed less investigations than FFY 2021. This decrease in investigation comple-
tion numbers is contributed to the increase in referrals to contracted FAIR, and expansion
to our internal FAIR program. Because of the increase of cases diverted through differential
response, there is also an increase in unsubstantiated cases, victims, and perpetrators.
Previously some of these cases may have received a lower-level substantiation.
Since 2012, the State’s intake unit has used the Structured Decision Making® (SDM) tool
to collect sufcient information to access and determine the urgency to investigate child
maltreatment reports. Currently, all screened-in reports are assessed in a three-tiered priority
process to determine the urgency of the workers rst contact; Priority 1 - Within 24 hours,
Priority 2 - Within 3 days, and Priority 3 - Within 10 days. In FFY 2022, accepted referrals
for family abuse cases were identied as 68 percent routine/Priority 3, 18 percent Priority 2,
and 14 percent urgent/Priority 1 in response.
The calculation of our average response time for FFY 2022 was an increase of 15 percent
from FFY 2021, but still improved from FFY 2020. Delaware has made great efforts to
improve our timeliness response to investigations. We are using data informed practice
and have established initial interview due date reports and initial interview completion rate
reports that are shared with all staff. Despite our efforts to improve timeliness of response,
our vacancy rate is the highest it has been which has led to increase caseloads and an
increase in response time, particularly on our priority 3 reports.
Children
The State uses 50 statutory types of child abuse, neglect and dependency to substantiate an
investigation. The State code denes the following terms: “Abuse” is any physical injury to a
child by those responsible for the care, custody and control of the child, through unjustied
force as dened in the Delaware Code Title 11 §468, including emotional abuse, torture,
sexual abuse, exploitation, and maltreatment or mistreatment. “Neglect” is dened as the
failure to provide, by those responsible for the care, custody, and control of the child, the
proper or necessary: education as required by law; nutrition; supervision; or medical, surgi-
cal, or any other care necessary for the child’s safety and general well-being. “Dependent
Child” is dened as a child under the age of 18 who does not have parental care because of
the death, hospitalization, incarceration, residential treatment of the parent or because of the
parent’s inability to care for the child through no fault of the parent. It is Delaware’s policy to
assess all children that are part of the household where the alleged maltreatment occurred.
In FFY 2022, substantiated victims of child maltreatment is 7 percent of the children in the
Child File. In FFY 21, 9 percent of the children in the Child File were substantiated victims
of child maltreatment. Delaware is able to capture specic information related to caregiver
and child risk factors. Delaware implemented sex trafcking as an allegation type in January
2020. Reports regarding noncaregiver perpetrators of sex trafcking are accepted and
included in NCANDS report. Delaware has been reporting infants with prenatal substance
exposure for a number of years.
Delaware (continued)
Child Maltreatment 2022
Appendix d: State Commentary 160

Fatalities
House Bill 181 requires the agency to investigate all child deaths of children aged 3 and
under that are sudden, unexplained, or unexpected. Delaware also has a Maternal and Child
Death Review Commission that reviews every child death in the state. There is also a Child
Abuse and Neglect (CAN) panel that conducts retrospective reviews on all child death and
child near death cases where abuse or neglect is suspected. The state does not report any
child fatalities in the Agency File that are not reported in the Child File. For FFY 2022, the
state reported 6 fatalities.
Perpetrators
Delaware maintains a condential Child Protection Registry for individuals who have been
substantiated for incidents of abuse and neglect since August 1, 1994. The primary purpose
of the Child Protection Registry is to protect children and to ensure the safety of children
in childcare, health care, and public educational facilities. The Child Protection Registry in
Delaware does not include the names of individuals, who were substantiated for dependency;
parent and child conict, adolescent problems, or cases opened for risk of child abuse and
neglect. An adult Delaware intends to substantiate will receive a written notice of intent to
substantiate at the conclusion of the investigation. The notication includes a hearing request
form that must be returned within thirty days of the postmarked date of the notication. The
hearing request form enables the individual to receive a substantiation hearing in Family
Court. When the hearing request form is not returned within the specied timeframe, the
individual will automatically be entered on the Child Protection Registry. A minor will
receive a substantiation hearing without submitting a hearing request form. This registry is
not available through the internet and is not the same as the Sex Offender Registry main-
tained by the Delaware State Police State Bureau of Identication.
For FFY 2022, parent as a perpetrator ranks the highest in the perpetrator relationship to the
child. The Other relationship would include individuals such as a babysitter or nonrelated
household member.
Services
During FFY 2021, Delaware’s Children’s Department saw an increase in the number of
children and families served in agency le elements 1.1.C-C and 1.1 E-F. This was due to the
reopening of many programs following the slowdown of the COVID pandemic.
One of our programs is Team Decision Making, which engages the family, informal sup-
ports and formal supports in planning for children who are at risk of coming into care. This
process has remained steady in diverting youth into kinship placements instead of Foster
Care. Family Team Meetings is a growing component of our casework practice. Delaware
continues it partnerships with community organizations to provide community-based pres-
ervation and reunication services including family interventionists and kinship navigators.
Delaware has expanded our contracts with post adoptive services. Delaware has collaborated
with numerous community partners to provide better services and plans of safe care for
infants with prenatal substance exposure. We have partnerships with domestic violence
and substance abuse agencies that provide intervention services in conjunction with agency
case management. Delaware plans to continue to build on our service array for prevention
services in the upcoming years.
Delaware (continued)
Child Maltreatment 2022
Appendix d: State Commentary 161

Delaware has added additional elds to capture information on services provided in our
FOCUS system. These service elds were newly built into our data system as of February
2018. They were intended to be mandatory elds, however there was a defect allowing work-
ers to complete the event without adding any services. A validation was added and improve-
ments on data entry have been seen. Although improvements have been made, there remains
a data entry and completion delay that is being addressed by operations.
Delaware Division of Family Services provides case management and some foster care ser-
vices. Delaware outsources with community agencies to support additional foster care homes
and group care, FAIR intervention, post-adopt support, and a number of other services.
Delaware (continued)
Child Maltreatment 2022
Appendix d: State Commentary 162

District of Columbia
Contact Lori Peterson Phone 202–434–0055
Title IT Manager (User Support)
Child Information System Administration
Email
Address Child and Family Services Agency
200 I St, SE
Washington, DC 20003
General
There have been no policy/practice changes that affect our FFY 2022 data. During FFY
2022, the Child and Family Services Agency (CFSA) has begun a new information technol-
ogy development process to replace its current SACWIS (known as “FACES”) with the new
CCWIS (known as Stronger Together Against Abuse and Neglect in DC (STAAND)). It is
anticipated that it will be complete in FFY 2024.
Reports
The data shows a slight increase in referrals. There has been an increase in vacancies in
CPS that have impacted our caseloads. The social work vacancies we are experiencing are
nationwide issue and our Human Resource department has hired a recruitment specialist to
help recruit to ll these vacancies.
Children
The District’s CFSA does not accept calls on alleged victims of sex trafcking aged above 18
years old. These occurrences are solely handled by the Metropolitan Police Department.
Fatalities
CFSA participates on the District-wide Child Fatality Review committee and uses informa-
tion from the Metropolitan Police Department and the District Ofce of the Chief Medical
Examiner (CME) when reporting child maltreatment fatalities to NCANDS.
The District reports fatalities in the Child File when neglect and abuse was a contributing factor
that led to the death of the child. The District denes Suspicious Child Death as a report of
child death is either unexplained, or concern exists that abuse or neglect by caregiver contrib-
uted to or caused the child’s death.
Child Maltreatment 2022
Appendix d: State Commentary 163

Florida
Contact Hans Soder Phone 850–717–4686
Title Director of Data & Information Services
Ofce of Child & Family Well-Being
Email
hans.soder@myfamilies.com
Address Florida Department of Children and Families
2415 N Monroe St, Ste. 400
Tallahassee, FL 32303
General
In seven Florida Counties (Walton, Seminole, Broward, Manatee, Pinellas, Pasco,
Hillsborough), Child Protective Investigations are handled by the County Sheriff’s Ofces
through grant agreements. There have been no recent changes to our policies affecting
NCANDS data for FFY 2022 (maltreatments and determination of ndings).
Florida uses one pathway for intakes screened in for investigation. All screened-in intakes
alleging abuse, abandonment, and/or neglect are responded to through an investigative
response by a Child Protective Investigator. A separate type of referral (Special Conditions
Referral) is generated when certain conditions are reported to the Hotline and do not meet
the criteria for an investigation (do not contain allegations of child abuse, abandonment,
or neglect), but warrant a response by the department, investigating sheriff’s ofce or
community-based-care child welfare professional. These special conditions referrals include
caregiver unavailable, child on child sexual abuse, parent needs assistance, and foster care
referral.
Reports
The criteria to accept a report are that an alleged victim:
■ Is younger than 18 years.
■ Is a resident of Florida or can be located in the state at the time of the report.
■ Has not been emancipated by marriage or other order of a competent court.
■ Is a victim of known or suspected maltreatment by a parent, legal custodian, caregiver, or
other person responsible for the child’s welfare (including a babysitter or teacher).
■ Is in need of supervision and care and has no parent, legal custodian, or responsible adult
relative immediately known and available to provide supervision and care.
■ Is suspected to be a victim of human trafcking by either a caregiver or non-caregiver.
The response commences when the assigned child protective investigator attempts the initial
face-to-face contact with the alleged victim. The system calculates the number of minutes
from the received date and time of the report to the commencement date and time. The min-
utes for all cases are averaged and converted to hours. An initial onsite response is conducted
immediately in situations in which any one of the following allegations are is made: (1) a
child’s immediate safety or well-being is endangered; (2) the family may ee or the child will
be unavailable within 24 hours; (3) institutional abuse or neglect is alleged; (4) an employee
of the department has allegedly committed an act of child abuse or neglect directly related to
the job duties of the employee; (5) a special condition referral (e.g., no maltreatment is alleged
but the child’s circumstances require an immediate response such as emergency hospitaliza-
tion of a parent, etc.); for services; or (6) the facts of the report otherwise so warrant. All
other initial responses must be conducted with an attempted onsite visit with the child victim
within 24 hours.
Child Maltreatment 2022
Appendix d: State Commentary 164

Several maltreatments map to “8 - Other” in Florida, including Threatened Harm, Intimate
Partner Violence Threatens Child, Household Threatens Child, and Family Violence
Threatens Child, this will inevitably increase the number of reported in the NCANDS
category of Other maltreatment values.
Children
The NCANDS Child File includes both children alleged to be victims and other children in
the household. The Adoption and Foster Care Analysis and Reporting System (AFCARS)
identication number eld is populated with the number that would be created for the child
regardless of whether that child has actually been removed and/or reported to AFCARS.
Although the Florida Hotline uses the maltreatment “Threatened Harm” only for narrowly
dened situations, investigators may add this maltreatment to any investigation when they
are unable to document existing harm specic to any maltreatment type, but the information
gathered, and documentation reviewed, yields a preponderance of evidence that the plausible
threat of harm to the child is real and signicant. Threatened Harm is dened as behavior
which is not accidental, and which is likely to result in harm to the child, which leads a pru-
dent person to have reasonable cause to suspect abuse or neglect has occurred or may occur
in the immediate future if no intervention is provided. However, Florida does not typically
add Threatened Harm if actual harm has already occurred due to abuse (willful action) or
neglect (omission which is a serious disregard of parental responsibilities).
Most data captured for child and caregiver risk factors will only be available if there is an
ongoing services case already open at the time the report is received or opened due to the
report.
A reduction in the child intake screen in rate within in the Florida Abuse Hotline resulted in
a decline in the total number of intakes accepted for investigation compared to the previous
year. This reduction has impacted the unique child counts, duplicate victim counts, and
unique perpetrator counts.
Fatalities
Fatality counts include any report closed during the year, even those victims whose dates of
death may have been in a prior year. Only veried abuse or neglect deaths are counted. The
nding was veried when a preponderance of the credible evidence resulted in a determina-
tion that death was the result of abuse or neglect. All suspected child maltreatment fatalities
must be reported for investigation and are included in the Child File. Beginning with the
2021 submission, the maltreatment of “Other” was removed from fatality records leaving
only the other maltreatment(s) in the investigation.
Perpetrators
By Florida statute, perpetrators are only identied as responsible for maltreatment in cases
with veried ndings. Licensed foster parents and non-nalized adoptive parents are mapped
to nonrelative foster parents, although some may be related to the child. Approved relative
caregivers (license not issued) are mapped to the NCANDS category of relative foster parent.
Florida (continued)
Child Maltreatment 2022
Appendix d: State Commentary 165

Florida reviews all children veried as abused with a perpetrator relationship of relative
foster parent, nonrelative foster parent, or group home or residential facility staff during the
investigation against actual placement data to validate the child was in one of these place-
ments when the report was received. If it is determined that the child was not in one of these
placements on the report received date, then the perpetrator relationship is mapped to the
NCANDS category of “other.”
Services
Due to the IV-E waiver and a cost pool structure that is based on common activities per-
formed that are funded from various federal and state awards, Florida uses client eligibility
statistics to allocate costs among federal and state funding sources. As such, Florida does not
link individuals receiving specic services to specic funding sources (such as prevention).
Florida (continued)
Child Maltreatment 2022
Appendix d: State Commentary 166

Georgia
Contact Michael Fost Phone 404-463-0845
Title Operations Analyst
Division of Family and Children Services
Email
michael.fost@dhs.ga.gov
Address Georgia Department of Human Services
47 Trinity Avenue SW
Atlanta, GA 30334
General
Screened-in maltreatment referrals that are not considered “Special” call types, are directed
to an Initial Safety Assessment, where case managers conduct a preliminary assessment to
determine if there is present or impending danger safety threats. The system determines the
track assignments based on safety threats recorded by the Case Manager. The track assign-
ment can be Investigation or Family Support Services (alternative response), depending on
safety threats recorded.
Special Investigation (Maltreatment in Care and Child Death, Near Fatality and Serious
Injury) cases are immediately assigned to the Investigation stage. Special Circumstances
— No Maltreatment Alleged Intakes are also assigned to the Investigation track, but with
a ve-day response time instead of immediate or one-day. Cases with allegations that are
considered dangerous (sexual abuse, physical abuse, maltreatment in care) are directed
immediately to the investigation pathway. Cases with other allegations undergo an “Initial
Safety Assessment” (ISA). A case worker interviews in person the alleged victim(s) and the
alleged perpetrator(s) at the home. Risk is assessed, and the case is then directed either to an
investigation or, if risk appears low, to the Family Support pathway. Investigations conclude
with a disposition of either substantiated or unsubstantiated, indicating whether a preponder-
ance of evidence supports the allegation(s) or not. Family Support Services cases can be track
assigned to Investigation if safety threats are observed or closed if no threats exist. Both
investigations and Family Support are included in the NCANDS Child File.
A decision to remove children into state custody does not depend on the investigation dis-
position, but on present or impending danger safety threats that indicate the child is unsafe.
Case Managers are required to explore Kinship Arrangements when an Out of Home Safety
Plan is necessary.
Reports
Georgia made changes to intake interviews over the past two years. More information is
gathered through a structured interview process. There were about 10,000 more referrals of
maltreatment in 2022 compared to 2021 and a greater proportion have been screened out.
The components of a CPS report are: (1) a child younger than 18 years; (2) a referral of
conditions indicating child maltreatment; and (3) a known or unknown individual alleged
to be a perpetrator. Referrals that do not contain all three components of a CPS report are
screened out. Screen-outs may include historical incidents, custody issues, poverty issues,
truancy issues, situations involving an unborn child, and/or juvenile delinquency issues. For
many of these, referrals are made to other resources, such as early intervention or prevention
programs.
Child Maltreatment 2022
Appendix d: State Commentary 167

Children
The number of unique child victims increased 9.1 percent from 2021 to 2022.
Fatalities
Georgia receives information from partners in the medical eld, law enforcement, Ofce
of the Child Advocate, other agencies, and the general public to identify and evaluate child
fatalities.
Approximately 20 more children died due to maltreatment in the 2022 report than in the 2021
report.
Perpetrators
Prior to July 1, 2016, a ruling of the Georgia Supreme Court prohibited the Division of
Family and Children Services from reporting perpetrator data. Changes in state law allowed
the formation of a Child Abuse Registry in July 2016, and Georgia began to report perpetra-
tor data. The change was accompanied by a decrease in substantiated investigations, perhaps
because of different evidence requirements. In 2020, the state discontinued the Child Abuse
Registry. Perpetrator data is still collected in the SACWIS system, and Georgia continues to
report perpetrator data in NCANDS. The effect, if any, on substantiation rates is not obvious.
Services
The agency does not provide Educational and Training, Family Planning, Daycare,
Information and Referral, or Pregnancy Planning Services for clients. These services would
be provided by referrals to other agencies or community resources. Our SACWIS system
would only track those services paid for by agency funds. However, most services are
provided through referrals to other agencies or community resources.
Georgia (continued)
Child Maltreatment 2022
Appendix d: State Commentary 168

Hawaii
Contact Rosaline Tupou Phone 808–586–5711
Title Administrator Hawaii Child Welfare Program
Development
Email
Address Princess Victoria Kamamalu Bldg
1010 Richards Street, Suite 216
Honolulu, HI 96813
The state did not submit commentary for the Child Maltreatment 2022 report.
Child Maltreatment 2022
Appendix d: State Commentary 169

Idaho
Contact Robbin Thomas Phone 208–334–5700
Title Research Analyst, Principal
Family and Community Services
Email
robbin.thomas@dhw.idaho.gov
Address Idaho Department of Health and Welfare
450 West State Street, 5th Floor
Boise, ID 83703
General
Idaho does not have an alternative response to screened-in referrals.
Reports
The number of accepted reports of maltreatment declined in the past year. However, there
has not been any practice or policy changes that would account for this change. Idaho has
stafng challenges and the intake unit is doing their best to ensure that if the priority guide-
lines do not clearly apply to the given circumstances, they are screening out where in the past
they may have screened something in.
Idaho has a centralized intake unit which includes a 24-hour telephone line for child welfare
referrals. The intake unit maintains a specially trained staff to answer, document, and pri-
oritize calls, and documentation systems that enable a quicker response and effective quality
assurance. Allegations are screened out and
not assessed when:
■ The alleged perpetrator is not a parent or caregiver for a child, the alleged perpetrator no
longer has access to the child, the child’s parent or caregiver is able to be protective of the
child to prevent the child from further maltreatment, and all allegations that a criminal act
may have taken place have been forwarded to law enforcement.
■ The alleged victim is under 18 years of age and is married.
■ The alleged victim is unborn.
■ The alleged victim is 18 years of age or older at the time of the report, even if the alleged
abuse occurred when the individual was under 18 years of age. If the individual is over 18
years of age, but is vulnerable (physically or mentally disabled), all pertinent information
should be forwarded to Adult Protective Services and law enforcement.
■ There is no current evidence of physical abuse or neglect and/or the alleged abuse, neglect,
or abandonment occurred in the past and there is no evidence to support the allegations.
■ Although Child and Family Services (CFS) recognizes the emotional impact of domestic
violence on children, due to capacity of intake, we only can respond to referrals of
domestic violence that involve a child’s safety. Please see the priority response guidelines
for more information regarding child safety in domestic violence situations. Referrals
alleging that a child is witnessing their parent/caregiver being hurt will be forwarded to
law enforcement for their consideration. Additionally, referents will be given referrals to
community resources.
■ Allegations are that the child’s parents or caregiver use drugs, but there is no reported
connection between drug usage and specic maltreatment of the child. All allegations that
a criminal act may have taken place must be forwarded to law enforcement.
■ Parental lifestyle concerns exist, but don’t result in specic maltreatment of the child.
■ Allegations are that children are neglected as the result of poverty. These referrals should
be assessed as potential service need cases.
■ Allegations are that children have untreated head lice without other medical concerns.
Child Maltreatment 2022
Appendix d: State Commentary 170

■ Child custody issues exist, but don’t allege abuse or neglect or don’t meet agency deni-
tions of abuse or neglect.
■ More than one referral describes the identical issues or concerns as described in a previous
referral. Multiple duplicate referrals made by the same referent should be staffed with the
local county multi-disciplinary team for recommendations in planning a response.
More information regarding intake, screening, and priority guideline standards can be found
on the Idaho Health and Welfare website.
The investigation start date is dened as the date and time the child is seen by a Child
Protective Services (CPS) social worker. The date and time are compared against the report
date and time when CPS was notied about the alleged abuse. Idaho reports substantiated,
unsubstantiated: insufcient evidence, and unsubstantiated: erroneous report dispositions.
Children
Idaho has incorporated modications related to policies or procedures in conducting investi-
gations during the past year. These changes enable staff to expedite the formal safety assess-
ment process in cases in which the allegations are determined erroneous. Idaho struggled
with stafng levels this year which impacted staff’s ability to conduct timely investigations.
Idaho’s current practice standard for Expedited Safety Assessment, Comprehensive Safety,
Ongoing, and Re-Assessment requires the social worker to interview all children of con-
cern, all child participants on a report, and any child who falls under the Temporary Child
Resident Standard. The practice standard denes child(ren) participants on a presenting issue
as, “all other children who are not identied as victim(s) of abuse or abandonment which
reside in or visit the home.”
Idaho collected data on sex trafcking victims on all children assessed for neglect, abuse, or
abandonment. In addition, Idaho assesses children in foster care for human trafcking during
child contact visits and when a youth returns from runaway status.
Idaho implemented data collection for prenatal substance exposure in April 2019. When our
centralized intake unit receives a report regarding concerns of a substance affected infant
information is collected regarding the plan of care and services provided. There were no
changes in policies or procedures regarding sex trafcking or referral of infants with prenatal
substance exposure during the pandemic.
All children ages birth to three years old who are involved in cases substantiated for abuse,
neglect and/or abandonment are referred to early intervention services through the Idaho
Infant and Toddler Program. More information regarding Idaho’s standards specic to safety
assessment, mandatory referrals for children birth to three, and human trafcking standards
can be found on the Idaho Health and Welfare website.
Fatalities
There were no changes in policies or procedures regarding child death reviews during the
pandemic. Idaho has a state child fatality review team who was able to make a slight sched-
ule adjustment and continue to meet to ensure reviews were completed as planned during
Idaho (continued)
Child Maltreatment 2022
Appendix d: State Commentary 171

the pandemic. Idaho compares fatality data from the Division of Family and Community
Services with the Division of Vital Statistics for all children younger than 18. The Division
of Vital Statistics conrms all fatalities reported by child welfare via the state’s SACWIS and
provides the number of fatalities for all children for whom the cause of death is homicide.
When a report is made to the Centralized Intake Unit, the Priority Response Guidelines
establish requirements for evaluating safety issues within Child and Family Services (CFS)
mandates and are utilized to determine the immediacy of the response timeframes. When
the death of a child is alleged to be due to physical abuse or neglect by the child’s parents,
guardian, or caregiver and reported information indicates there may be safety threats to any
minor siblings remaining in the home, CFS will assess the safety of the other children in the
home with an immediate response.
Perpetrators
Idaho Administrative Code for the purpose of substantiating an individual for abuse,
neglect or abandonment does not dene the age of a suspect or perpetrator. However, for the
purpose of Idaho’s Child Protection Central Registry levels of risk, for an individual to be
to be placed on the Central Registry at the highest level for sexual abuse they must meet the
denition of sexual abuse as dened in Idaho Statute. Idaho Statute 18-1506 includes in the
denition of sexual abuse of a child under the age of sixteen year that it is a felony for any
person eighteen (18) year of age or older. Idaho’s practice is to substantiate suspects who are
over the age of eighteen (18) or are the parent of the victim.
Idaho does report noncaregiver preparators of substantiated cases related to sex trafcking.
Idaho’s other perpetrator relationship is for other relative. We have dened categories for
stepparents, grandparents, and great grandparents therefore other relative is typically used for
aunt, uncle, or cousin or other relative relationships.
Services
Currently, Idaho is unable to report public assistance data due to constraints between Idaho’s
Welfare Information System and CCWIS. Idaho has had no changes in preventive funding.
Federal initiatives through CAA and ARPA provide additional funding to support youth who
may have aged of foster care to remain in foster care and/or receive additional services to
help them successful transition to adulthood. Idaho utilized contractors service providers and
community service providers and/or agencies to provide services to families and children.
Idaho (continued)
Child Maltreatment 2022
Appendix d: State Commentary 172

Illinois
Contact Jennifer Eblen-Manning Phone 708–338–6618
Title Deputy Director
Quality Assurance
Email
jennifer[email protected]
Address Department of Children and Family Services
1701 S. First Ave, 10th Floor Rm 1060
Maywood, IL 60153
General
Currently Illinois does not have a Differential Response pathway. The Illinois NCANDS
Child File contains reports of child abuse/neglect that resulted from a hotline call meeting
the standards of abuse/neglect as dened in department procedure 300.30(a)(1) Criteria for a
Report of Abuse or Neglect.
Illinois DCFS launched a Streamlined Online System for Reporting of Non-Emergency
Child Abuse and Neglect in October 2020. This system makes it easier for everyone to le a
report of suspected abuse or neglect.
Reports
The following criteria must be met for a report of abuse or neglect to be taken:
■ The alleged child victim must be under 18 years of age or be between the ages of 18–22
while living in a DCFS licensed facility.
■ There must be an incident of harm or a set of circumstances that would lead a reasonable
person to suspect that a child was abused or neglected as interpreted in the allegation
denitions contained in Procedures 300, Appendix B; and
■ The person committing the action or failure to act must be an eligible perpetrator:
• For a report of suspected abuse, the alleged perpetrator must be the child’s parent,
immediate family member, any individual who resides in the same home as the child,
any person who is responsible for the child’s welfare at the time of the incident, a
paramour of the child’s parent, or any person who came to know the child through an
ofcial capacity or is in a position of trust.
• For a report of suspected neglect, the alleged perpetrator must be the child’s parent or
any other person who was responsible for care of the child at the time of the alleged
neglect.
The Illinois DCFS procedures allow taking multiple reports on the same child abuse and
neglect incident when there are multiple perpetrators that either do not reside in the same
residence or reside in the same residence as a child victim but are part of separate and inde-
pendent families. In these situations, there are separate reports taken for each perpetrator.
The number of reports for FFY 2022 show an increase compared to FFY 2021, which
appears to be related to the school districts returning to in class learning during the reporting
period. With the resumption of in class learning, Illinois data reects the number of reports
made by education personnel increased which accounts for 85 percent of increase in the
unique reports.
Since the start of the pandemic, the Child Abuse/Neglect Hotline has never shutdown, staff
transitioned to working from home after the Governor issued the stay home order. There
were no changes to criteria for screening calls of abuse/neglect. COVID-19 screening
Child Maltreatment 2022
Appendix d: State Commentary 173

questions were added, consistent with CDC and IDPH (Illinois Department of Public Health)
guidance for worker safety in responding to reports of abuse/neglect.
Illinois reports “nonmandated reporters” to the NCANDS report source category of “other”.
The state does not collect any subtype information. The state’s online system is a self-
reported report source.
Children
Illinois uses the allegation of Substance Misuse to report on infants with prenatal substance
exposure among other types of substance misuse for children and youth.
Illinois has an allegation of Human Trafcking, which, according to the federal law, is
dened as twofold:
“sex trafcking in which a commercial sex act is induced by force, fraud, or coercion, or
in which the person induced to perform such act has not attained 18 years of age; or the
recruitment, harboring, transportation, provision, obtaining, patronizing or soliciting of
a person for labor or services, through the use of force, fraud, or coercion for the purpose
of subjection to involuntary servitude, peonage, debt bondage or slavery.” [22 U.S.C.
§7102(8)]
For the purpose of a child abuse/neglect investigation, force, fraud, or coercion need not be
present. Incidents of Maltreatment:
■ Labor exploitation (ABUSE).
■ Commercial sexual exploitation (i.e., prostitution, the production of pornography or sexu-
ally explicit performance) (ABUSE).
■ Blatant disregard of a caregiver’s responsibilities that resulted in a child being trafcked
(NEGLECT).
Since Illinois’s denition of sex trafcking is a part of a broader denition of Human
Trafcking that also includes labor exploitation and blatant disregard of a caregiver’s respon-
sibilities, it is mapped to the NCANDS maltreatment type 8 — Other. Illinois procedure
related to Human Trafcking was updated on 9/16/2022 to collect data specic to Human
Labor Trafcking Abuse allegation, Human Sex Trafcking Abuse allegation, Blatant
disregard of a caregiver’s responsibilities that result in Human Labor Trafcking Neglect
allegation, and Blatant disregard of a caregiver’s responsibilities that result in Human Sex
Trafcking Neglect allegation. Illinois is working to ensure it can collect and produce data on
these new elements out of SACWIS.
Currently, Illinois reports child risk factors for youth with prior or current foster care
involvement only.
Fatalities
Illinois DCFS procedures allow for multiple reports on the same child abuse and neglect
incident (fatal incidents included) to be taken when there are multiple perpetrators that either
do not reside in the same residence or reside in the same residence as the child victim, but
are of separate and independent families. In these situations, there are separate reports taken
for each perpetrator. This policy has the potential to report the same child fatality in multiple
Illinois (continued)
Child Maltreatment 2022
Appendix d: State Commentary 174

reporting cycles if the disposition (nal nding) dates occur in different reporting cycles. No
other data system or agencies are used to compile and report child fatalities due to suspected
abuse or neglect.
In Illinois, mandated reporters are required to report suspected child abuse or neglect imme-
diately (fatal incidents included) when they have “reasonable cause to believe” that a child
known to them in their professional or ofcial capacity may be an abused or neglected child”.
(325 ILCS 5/4) Reports are made by calling the DCFS Child Abuse Hotline. Mandated
reporters include, but are not limited to, medical personnel, law enforcement personnel,
coroners, medical examiners, and funeral home directors.
Perpetrators
The state makes a dispositional allegation-based determination for perpetrators for alleged
victim. The Illinois Abused and Neglected Child Reporting Act (ANCRA) [325 ILCS 5/5] and
Rule 300, Reports of Child Abuse and Neglect, does not set a minimum age for a perpetra-
tor, except for Allegation #10 – Substantial Risk pf Physical Injury (minimum age of 16),
therefore any case involving a young perpetrator must be assessed on an individual basis
according to the dynamics of the case.
The state is currently unable to report caregiver risk factors.
Services
Illinois case-management services include intact family and foster care services. The state
contracts 70 percent–80 percent of its casework to community-based provider agencies.
The Intact Family Services program is designed to work with families voluntarily who have
come to the attention of the Department of Children and Family Services: 1) as a result of
an indicated nding from a child abuse/neglect investigation, 2) as a result of an unfounded
investigation if approved by the Ofce of Intact Family Services, or 3) involuntarily when
ordered by the court to provide services as dened in Procedures 302.388. There are 5 target
populations served by Family First Prevention Services and intact family services is the
largest group.
Illinois (continued)
Child Maltreatment 2022
Appendix d: State Commentary 175

Indiana
Contact Kara Riley Phone 765–431–0851
Title Data Analyst–Federal Reporting Project Manager Email
kara.riley@dcs.in.gov
Address Indiana Department of Child Services
Ofce of Data Management
302 W. Washington St, Room E306–MS47
Indianapolis, IN 46204–2739
General
Indiana has engaged in continuous improvement efforts to rene the data collection and
mapping process through system modications and overall enhancement. The Management
Gateway for Indiana’s Kids (MaGIK) is an ever-evolving, umbrella system which has further
incorporated services, billing, case management, and the overall data management, organiza-
tion, and extraction components.
Reports
The Indiana Department of Child Services (DCS) does not assign for assessment a referral of
alleged child abuse or neglect that does not:
■ Meet the statutory denition of child abuse and neglect; and/or
■ Contain sufcient information to either identify or locate the child and/or family and
initiate an assessment (Indiana Policy Manual 3.6).
As of January 1, 2018, the Hotline ceased automatically recommending assessment of all
reports with alleged victims under the age of three years old.
As of July 1, 2019, a change in legislation increased the 1-hour response time to 2-hours.
Effective June 1, 2021, DCS Hotline modied its standardized worker safety questions. DCS
also partnered with the Capacity Building Center for States as well as ran internal events
targeted at reducing our screen-in rate. DCS made decision modications on types of reports
to screen out that include, but are not limited to:
■ “Sexting” concerns among adolescents, effective October 1, 2020.
■ Pre-adolescent children exhibiting potentially sexually maladaptive behaviors, effective
January 1, 2021.
■ Marijuana use only reports with children 3 and older, effective April 1, 2021.
■ Educational neglect, effective August 16, 2021.
Effective June 1, 2021, every screen-out report (including child fatalities and near fatalities)
will be reviewed by one hotline supervisor, then sent to the local DCS ofces, where one
member of management will be designated to make the nal determination within 24 hours.
DCS Hotline also ceased doing the additional screen out review for children under 3.
Effective February 28, 2022, a practice change was implemented where DCS Hotline would
no longer document certain reports that provide no value. Examples include wrong numbers,
immediate disconnects, internal DCS conversations, or simply transferring a call to another
worker within the Hotline.
Child Maltreatment 2022
Appendix d: State Commentary 176

Children
Indiana continues to work with its eld staff responsible for entering reports and completing
assessments and emphasizing the importance of entering all applicable data, including child
risk factors. Indiana completes daily Assessment Stafngs between eld workers and super-
visors, which emphasizes ensuring the safety of children as quickly as possible.
In FFY 2021, Indiana streamlined their assessment completion processes for SafeACT
assessments (where all children in the assessment are deemed clearly safe) and Professional
Service Requests. Streamlining these processes should allow workers to initiate and complete
all assessments more timely.
Fatalities
All data regarding child fatalities are submitted exclusively in the Child File. Fatality counts
for the FFY are based on the date of an approved, substantiated, fatality assessment. DCS
completes a review of all child fatalities that t the following circumstances:
■ Children under the age of 3: the child’s death is sudden, unexpected or unexplained, or
there are allegations of abuse or neglect;
■ Children age 3 or older: the child’s death involves allegations of abuse or neglect.
Reports for fatalities can be made from multiple sources, including DCS, law enforcement,
re investigator, emergency medical personnel, coroners, the health department, or hospitals.
Reports can be made from these sources related to drownings, poisonings/overdoses, asphyx-
iation, etc., which may include accidents. It is the intention for these reporting standards not
only to be used to determine if abuse or neglect was involved but also as an evaluation tool to
inform practice.
Perpetrators
Indiana launched a new intake system in February 2016 that better aligns with the system
used for completing assessments and case management cases. This has allowed for more
accurate perpetrator data entry.
Services
Improvements in data collection allowed Indiana to report prevention data by child.
Therefore, to not duplicate counts, Indiana does not provide prevention data on a family level.
In FFY 2021, a CBCAP COVID grant was added as a separate federal funding source,
which allowed Indiana to serve more children. On June 1, 2020, Indiana Family Preservation
Service was launched. This service is required to be referred on all new in-home child/chil-
dren in need of services (CHINS) and informal adjustments (IA). This service is a per diem
that encompasses all services that the family needs to remain safely in the home with their
caregivers.
Indiana (continued)
Child Maltreatment 2022
Appendix d: State Commentary 177

Iowa
Contact Lynda Miller Phone 515-377-0390
T
itle
Management Analyst 3
Bureau of Quality Assurance & Improvement
Email
Address Iowa Department of Health and Human Services
PO Box 4826, Des Moines, IA 50305
General
Iowa has two types of responses to screened-in referrals/reports of suspected abuse. Our
traditional pathway is called a child abuse assessment and the alternative response pathway
is called a family assessment. The child abuse assessment pathway requires a determination
of abuse and a determination of whether criteria for placement on the Registry are met. The
family assessment pathway identies family strengths and needs, connects the family to the
appropriate services needed, and does not include a determination of abuse or a determina-
tion of whether criteria for placement on the Registry are met. Data from both pathways are
reported to NCANDS.
A signicant number of Iowa laws impacted state policies and procedures that in turn may
have affected FFY 2022 data to NCANDS, including the following which were effective July
1, 2022:
■ Safe haven laws were extended from a newborn infant who is or appears to be thirty
days of age or younger to a newborn infant who is or appears to be ninety days of age or
younger.
■ Massage therapists were added to the list of mandatory reporters of both child and depen-
dent adult abuse.
■ A requirement that an allegation of Denial of Critical Care or an allegation of Dangerous
Substance to be reported within ve years to qualify as child abuse.
■ The removal of a requirement for a written report of suspected abuse to be submitted
within 48 hours of the oral report and maintains that only an oral report is required.
■ Amendments to CINA proceeding, including:
• A requirement that the GAL must be an attorney and not a CASA,
• An addition of “objective criteria” to be used in GAL recommendations,
• A presumption it is in the best interest of children 10 years and older to attend court,
• Allows for removal of “domestic abusers” from the residence pursuant to a court order,
• An underscoring of the harm caused by removal of a child and that it must be weighed
against the potential harm in allowing a child to remain with the child’s family,
• A prioritization of relatives and ctive kin as preferred placements,
• Providing notice to adult relatives, even if the custody is not transferred to the Iowa
Department of Health and Human Services (HHS),
• Permission for HHS to share information necessary to explore potential relative
placement,
• A focus on family interaction even when parents fail to comply with court require-
ments, so long as it’s not detrimental to the child, and
• Reasonable efforts to place siblings together.
Child Maltreatment 2022
Appendix d: State Commentary 178

Reports
The number of suspected reports of abuse decreased slightly in FFY 2022. This decrease was
small and not a difference of 10 percent or more. The law change which requires an allega-
tion of Denial of Critical Care or an allegation of Dangerous Substance to be reported within
ve years to qualify as child abuse took effect on July 1, 2022, and may have been a factor in
this slight decrease. However, the law change was implemented toward the end of FFY 2022
and it would have only impacted the last three months of data.
Additionally, new staff were hired and trained with an expansion in the hours of operation for
Iowa’s Centralized Service Intake Unit (CSIU)/abuse hotline. CSIU transitioned to a 24-hour
unit in January 2021, so by the start of FFY 2022, there were an addition of 21 staff who
had been in their positions for less than 10 months. This increase in new intake staff is not
believed to have impacted the number of screened in referrals.
Children
The number of victims of abuse decreased slightly in FFY 2022. This decrease was small.
While it’s unknown what contributed to the slight decrease, barriers to collecting and reporting
data for infants with prenatal substance exposure remains a topic of discussion. A lack of com-
mon understanding and application of what constitutes “infant affected” has led to confusion
around what medical providers feel they should be reporting and how child welfare staff should
be responding. Policies and procedures have not changed regarding the referral of infants with
prenatal substance exposure, but conversations with medical provider partners have increased
and trainings with child welfare staff have increased in attempt to assure these infants are being
identied and Safe Plans of Care are created for them and their caregivers.
Fatalities
While Iowa’s Child Death Review Team does review all fatalities of children that were
sudden, unexpected, or nonnatural deaths, Iowa Agency File fatalities are collected from data
maintained internally by the Iowa Department of Health and Human Services (HHS). Infant/
child deaths are only assessed by HHS when there is an allegation of abuse.
The number of child maltreatment fatalities increased signicantly in FFY 2022. While the
total number was not more than 10, this difference was more than a 50 percent increase,
jumping from twelve child maltreatment fatalities in FFY 2021 to nineteen in FFY 2022.
Fatalities related to unsafe sleep made up the majority of this increase. With the awareness of
safe sleep recommendations on the rise and the number of those cases which include sub-
stance use by the parent/caretaker, it is no surprise that we are seeing an increase in fatalities
resulting from unsafe sleep.
Looking at this data in total, nineteen child fatalities were the result of abuse or abuse as
a contributing factor. A state review of the maltreatment death data indicated unsafe sleep
made up over one-third (seven) of all child maltreatment deaths, involving infants between 10
days and 6 months of age. In ve of these instances, a parent or older sibling was co-sleeping
with the infant on an adult bed or couch/recliner. The other two instances involved unregu-
lated in-home childcare providers, one who placed an infant on an adult bed to sleep and
another who placed an infant on their stomach in a pack and play to sleep.
Iowa (continued)
Child Maltreatment 2022
Appendix d: State Commentary 179

Physical Abuse attributed to nearly one-quarter (four) of all child maltreatment deaths.
Strikingly, all four of these physical abuse incidents were caused by a parent (one, which also
included a paramour of the child’s mother). The physical abuse incidents involved children
between 19 days and 2 years of age.
Drownings accounted for three of all child maltreatment deaths, involving children between
9 months and 2 years of age, with one occurring in a residential pool and the other two in a
bathtub. The persons responsible in all three of the drowning incidents were parents.
The ve remaining child maltreatments deaths were single cases of inadequate medical
care, motor vehicle accident, suicide, accidental gunshot, and asphyxiation. These incidents
involved ve children between 1 year and 13 years of age. In these incidents, three of the
persons responsible were parents, one was a foster parent, and one was an unregulated in-
home childcare provider. When considering whether any child maltreatment deaths included
a history of HHS assessment or services, it was determined that eight of the nineteen child
maltreatment deaths had both assessment and service history, six of the nineteen had assess-
ment history only (no service history), and ve of the nineteen had no assessment or service
histor y.
Perpetrators
Perpetrators in Iowa include individuals of any age who have caregiver responsibilities at the
time of the alleged abuse, or a person 14 years of age or older who sexually abuses a child
they reside with, or a person who engages in or allows child sex trafcking. This denition,
in accordance with federal regulation, denes any perpetrator of child sex trafcking as a
perpetrator of child abuse and therefore, includes data in NCANDS reporting for persons
who may otherwise be considered noncaregivers.
In FFY 2022, the incidents of abuse perpetrated by a childcare provider increased by more
than 200 percent. The logic for perpetrator information did not change and there is no clear
explanation for this dramatic increase. Factors may include an increase in children’s mental
health issues that result in increased behaviors, under trained staff, increased substantia-
tions of abuse due to non-compliance with regulatory rules, and seeing a rise in numbers of
children returning to childcare since the height of the COVID-19 pandemic.
Services
Iowa has both preventative and post-response services. Preventative services, referred to as
Non-Agency Voluntary Services, are available on a voluntary basis to families following an
assessment where abuse is not substantiated or abuse is conrmed (substantiated, but not
placed on the central abuse registry) and there is low or moderate risk. These services are
provided through contracts with external partners to strive to keep children safe from abuse,
keep families intact, prevent the need for future involvement from the child welfare system,
and to build ongoing connection to community-based resources.
Postresponse services, referred to as Family Centered Services, are required for families
where abuse is conrmed (substantiated, but not placed on the central abuse registry) and
there is high risk or for families where abuse is founded (substantiated, and placed on the
central abuse registry) and the risk is low, moderate, or high. These services are provided
Iowa (continued)
Child Maltreatment 2022
Appendix d: State Commentary 180

through contracts with external partners and managed by the Iowa’s child welfare agency
to offer a exible array of culturally sensitive interventions and supports (including Family
Preservation Services, Solution Based Casework, and SafeCare), to achieve safety and
permanency for children and their families.
Iowa (continued)
Child Maltreatment 2022
Appendix d: State Commentary 181

Kansas
Contact Ashley Johnson Phone 785–380–6445
Title Deputy Director of Performance Improvement Email
ashleyr[email protected]
Address Prevention & Protection Services
Department for Children & Families
555 S Kansas Avenue
Topeka, KS 66603
General
In the event there is no concern of maltreatment, but an assessment and referral from DCF
may be necessary, Kansas does have a non-abuse/non-neglect category of case assignment
called Family in Need of Assessment (FINA). FINA cases are not counted as screened-out
reports. They are screened in, but as FINA as opposed to Abuse/Neglect (maltreatment).
Reports
Reasons for screening out allegations of child abuse and neglect include:
■ Initial assessment of reported information does not meet the statutory denition: Report
does not contain information that indicates abuse and neglect allegations according to
Kansas law or agency policy.
■ Report fails to provide the information necessary to locate child: Report doesn’t provide
an address, adequate identifying information to search for a family, a school where a child
might be attending, or any other available means to locate a child.
■ The Department of Children and Families (DCF) does not have authority to proceed or
has a conict of interest if: Incidents occur on a Native American reservation or military
installation; alleged perpetrator is a DCF employee; alleged incident took place in an
institution operated by DCF or Kansas Department of Corrections – Juvenile Services
(KDOC-JS); or alleged victim is age 18 or older.
■ Incident has been or is being assessed by DCF or law enforcement: Previous report with
the same allegations, same victims, and same perpetrators has been assessed or is cur-
rently being assessed by DCF or law enforcement.
Children
The decrease in the number of child victims compared to last year may be partially attrib-
uted to updating the Kansas Protection Reporting Center (KPRC) processes including
Structured Decision Making (SDM) denitions as well as education and training to KPRC
staff. KPRC staff have received updated training on how SDM is applied, Risk Intelligence,
and Questions that Make a Difference. KPRC leadership and staff have received additional
coaching throughout the year on SDM and how to utilize the updated SDM denitions.
Kansas has also implemented the Kansas Practice Model statewide and focused on the issue
of poverty vs. neglect (for example, a child who may have been an alleged victim of Physical
Neglect may instead be an identied child on a Family in Need of Assessment case and
receive an assessment and referral for services if warranted).
Kansas is also working diligently to provide education and resources to communities includ-
ing educators and other mandated reporters on ways to best support children and families
when DCF interventions may not be necessary, which includes connecting families to
community-based services. In the event there is no concern of maltreatment, but an assess-
ment and referral from DCF may be necessary, Kansas does have a non-abuse/non-neglect
category of case assignment called Family in Need of Assessment (FINA). FINA cases are
Child Maltreatment 2022
Appendix d: State Commentary 182

not counted as screened out reports. They are screened in, but as FINA as opposed to Abuse/
Neglect (maltreatment). Case assignments have decreased as a whole, which is also likely
why we are seeing a decrease in the total number of unique child victims.
Fatalities
Kansas uses data from the Family and Child Tracking System (FACTS) to report fatalities to
NCANDS. Maltreatment ndings recorded in FACTS on child fatalities are made from joint
investigations with law enforcement. The investigation from law enforcement and any report
from medical examiner’s ofce would be used to determine if the child’s fatality was caused
by maltreatment. The Kansas Child Death Review Board reviews all child deaths in the state
of Kansas. Child fatalities reported to NCANDS are child deaths because of maltreatment.
Reviews completed by the state child death review are completed after all the investigations,
medical examiner’s results, and any other information related to the death is made available.
The review by this board does not take place at the time of death or during the investigation
of death. The state’s vital statistics reports on aggregate data are not information specic to
an individual child’s death.
Perpetrators
Kansas does report noncaregiver perpetrators of sex trafcking. Kansas has a minimum
age of 10 years for a child to be considered an alleged perpetrator of maltreatment. The
NCANDS category of “other” perpetrator relationship includes the state category of not
related.
Services
Kansas does not capture information on court-appointed representatives. However, Kansas
statute (K.S.A. 38-2205) requires the child to have a court-appointed attorney (GAL).
Kansas has placed an emphasis on child and family well-being and prevention services in
recent years. This has included implementation of the Kansas Practice Model, Family First
Prevention Services, Family Resource Centers, a mobile crisis service for children and youth
experiencing a mental health crisis, and advisory councils that partner with the voices of
those directly impacted by services. Kansas DCF provides many of these prevention services
as well as foster care case management through contracts or grants awarded to other organi-
zations who provide direct services to children and families.
Kansas (continued)
Child Maltreatment 2022
Appendix d: State Commentary 183

Kentucky
Contact Melanie Day Phone 502-564-7635
Title Quality Assurance Branch Manager
Protection and Permanency
Email
melanie.day@ky.gov
Address Department of Community Based Services
275 East Main Street 3E-A Frankfort KY 40621
General
Kentucky does not currently have a true alternative or differential response. assessment
worker (investigation worker) makes an (investigation response (IR) or family in need of
services response determination at the completion of the assessment (investigation).
Kentucky has the following dispositional ndings for investigations/assessments: fatality/
near fatality substantiated, found/substantiated, substantiated, unsubstantiated, and services
needed. For the purposes of NCANDS reporting, services needed is mapped to the NCANDS
disposition of “other.” Kentucky currently does not map a dispositional nding to alternative
response. Kentucky has begun the tasks associated with implementation of a true alternative
response system. With full implementation of an alternative response statewide, the depart-
ment anticipates a decrease in the number of past due investigations/assessments. Alternative
response is anticipated to be implemented by 2024.
Kentucky’s business practice does allow multiple maltreatment levels to be present in a
single report. For example, one report could have a disposition/nding of unsubstantiated and
services needed if it was determined that maltreatment did not occur, but the family needed
services from the agency.
Reports
Each of the nine service regions in Kentucky houses a central intake (CI) team which oper-
ates the statewide abuse and neglect reporting system. Due to the high volume of reports and
population size, Jefferson County has two CI teams. All ten CI teams are housed under one
statewide branch focused on serving their respective service region.
The CI phone system allows teams to “share” call volume by serving consumers across
regional boundaries. The statewide hotline number rst directs calls based on area codes to
the corresponding service region. If all lines for that service region are busy, the call then
bounces over to the next available CI team member statewide. This has improved customer
experience via shorter wait times, increased service efciency, and expanded coverage to
meet business needs.
The statewide call platform was implemented in July 2019 with all teams online by March
2020. A partnership with Seven Counties Services, Kentucky’s after-hours hotline operator,
began in 2022 and was implemented January 2023. This expanded the number of employees
and ensured more calls were answered in a timely manner. The PureCloud phone system
used by DCBS’s CI staff became available for Seven Counties Services hotline employees
as of February 2023. All staff using the same platform allows DCBS staff to easily reference
and pull detailed data on the number of calls, wait times, staff averages, and performance.
The PureCloud system also allows Kentucky to track metrics such as call volume, wait times,
call times, call recording for coaching and mentoring opportunities, etc. Additional stored
information may be revisited for delity matters or staff training.
Child Maltreatment 2022
Appendix d: State Commentary 184

To slow down the intake process and gather the information needed to make better decisions for
assessing reports for acceptance, the Department took steps to enhance the skills of intake staff
through the implementation of the Structured Decision Making® (SDM®) Intake Assessment
Tool. The intake assessment is consensus-based, meaning it is designed to operationalize
Kentucky’s standards of practice (SOP) and statute in a decision support tool. Through training
and practice guidance, intake staff will be able to slow down the intake process to thoroughly
review each intake to ensure each adequately meets acceptance criteria and have the supportive
guidance to go through each section of intake criteria with specic denitions while evaluating
the report. This will assist in decreasing the number of false positive acceptances (referrals that
are incorrectly accepted for investigation), consequently reducing staff burden.
The SDM® Intake Assessment Tool was released for staff use on April 2, 2022. The DCBS
Training Branch received a training of trainer’s session in February 2022. This allowed
DCBS Training Branch staff time to create and implement trainings for frontline staff of
the intake assessment. The SDM® vendor, Evident Change, trained central intake staff on
the SDM® Intake Assessment Tool March 8-18, 2022. The DCBS Training Branch provided
29 training sessions around the SDM® Intake Assessment Tool throughout the month of
April to all Kentucky frontline staff and supervisors to ensure all staff understand the intake
assessment and updated policies.
Efforts to address staff turnover and decrease caseloads to stabilize the workforce have
continued. Regional retention committees are operational in all regions. Alternative work
schedules have been operationalized in several pilot areas throughout the state and discus-
sions are occurring regarding expansion. Current plans are underway to allow for more staff
the option to telecommute or work a hybrid schedule that would allow partial telecommuting
and partial time in the ofce. Along with pay raises in December 2021, May 2022, and July
2022, several long overdue pay grade changes were enacted as part of a larger plan to address
the Department’s pay equity issues. This issue will not be solved short term but rather over
the process of several years. Kentucky is only in the initial stages of addressing its pay equity
issues that it has attributed to its staff turnover.
The Child Protection Branch completed revisions of Standards of Practice (SOP) Online
Manual Chapter 2- Child Protective Services (CPS) Intake and Investigation to align with
changes resulting from the new intake tool release and to better align with current regula-
tions. CPS workforce data for Kentucky only includes full-time equivalents (FTEs).
The state does not collect in-depth information regarding the number of children who are
screened out for referrals that do not meet criteria for abuse or neglect. In January 2018, the
state implemented new response times based upon the safety threats and risk factors identi-
ed by the reporting source. For example, two reports both alleging sexual abuse may cur-
rently have different response times based upon the perpetrator’s current location and access
to the victim. Prior to this change, each maltreatment type had a single response time, e.g.,
all reports alleging sexual abuse had a response time of one hour. The response times were
overall increased with this change, as reports identied as low or no risk were previously
assigned a response time of 48 hours, but now may have up to 72 hours, which likely is the
cause of the continued increase to average response time in this submission. In addition, the
Kentucky (continued)
Child Maltreatment 2022
Appendix d: State Commentary 185

responsibility of determining response times during normal business hours was transferred
from eld staff supervisors to centralized intake supervisors.
Children
An overall decrease for child victims was observed between FFY 2021 and FFY 2022.
Kentucky has worked diligently over the past several years to implement a safety model
which includes the implementation of SDM® Intake Assessment Tool and a thorough review
and modication of the state’s acceptance criteria to ensure a focus upon children and fami-
lies with true safety threats versus risk factors. This shift in the approach to the work may
have contributed to the decrease in child victims this year. Kentucky’s SOP 2.11-Investigation
Protocol indicates unannounced face-to-face interviews should be completed with all house-
hold members including all other children in the home.
In 2022, Kentucky revised program areas specically related to human trafcking allega-
tions to ensure non-caretaker reports were accepted appropriately. This change was made
to fulll federal reporting requirements to differentiate between sex trafcking and labor
trafcking, and to ensure proper identication of caretaker vs. non-caretaker perpetrators.
The revised program/subprograms are now Human Trafcking-Sexual-Caretaker, Human
Trafcking-Labor-Caretaker, Human Trafcking-Sexual-Non-caretaker, and Human
Trafcking-Labor-Non-caretaker.
Findings of Human Trafcking Conrmed or Human Trafcking Not Conrmed are associ-
ated with non-caretaker reports of human trafcking. Non-caretaker reports of human
trafcking cannot receive a substantiated nding, therefore, alleged perpetrators will not
receive a Notication of Findings Letter. Non-caretaker perpetrators do not have due process
to le an appeal as outlined in 922 KAR 1:300 Child protective services.
The Department updated its CCWIS screens in 2022 to indicate whether an individual is a
victim of human trafcking, as well as to distinguish between labor and sex trafcking. The
Department publishes an annual human trafcking report to the LRC, which includes data
on demographics, trends, and case ndings regarding human trafcking reports. Across the
state, community partners utilize the report to guide practice for service delivery to victims
of human trafcking. The report is posted online annually and can be found on the division’s
public facing website.
Kentucky began capturing safe care plan data and referral to appropriate services in FFY
2019. FFY 2022 is Kentucky’s third full year of reporting for infants with prenatal substance
exposure. Kentucky’s Plan Of Safe Care SOP can be found at SOP 1.15-Working with
Families Affected by Substance Misuse.
Fatalities
Kentucky has a Systems Safety Review (SSR) team which reviews all cases involving a
child fatality in an active CPS case and/or accepted as an investigation with the fatality/
near fatality designation. An initial review is completed by a system safety analyst and is
then presented to the multi-disciplinary team (MDT) for consideration of a comprehensive
analysis. The state investigates only child fatalities that are a result of maltreatment.
Kentucky (continued)
Child Maltreatment 2022
Appendix d: State Commentary 186

The state uses CCWIS to capture information on child fatalities related to maltreatment.
For every fatality investigated as a possible death caused by maltreatment, the investiga-
tor obtains a copy of the ofcial death certicate and autopsy conducted by the medical
examiner from the Department of Public Health (DPH). The investigator incorporates this
information into decision making around the investigative ndings, as well as case disposi-
tion. A discussion of the contents of these documents is included in the assessment entered
into CCWIS. These documents, as well as any additional documents such as those produced
by law enforcement, are maintained in the case le.
Perpetrators
The number of perpetrators in Kentucky decreased by 16.9 percent in FFY 2022. Kentucky
has worked diligently over the past several years to implement a safety model which includes
the implementation of SDM® Intake Assessment Tool and a thorough review and modica-
tion of the state’s acceptance criteria to ensure a focus upon children and families with true
safety threats versus risk factors. This shift in the approach to the work may have contributed
to the decrease in perpetrators this year.
Kentucky’s SOP 2.3-Acceptance Criteria states: A report that meets child abuse, neglect, or
dependency criteria which involves an alleged perpetrator between the age of twelve (12)
and seventeen (17) years old who is in a caretaking role will be accepted. If substantiated,
the child aged twelve (12) to seventeen (17) will be identied as the perpetrator.
Kentucky reports Perp REL as 88-other for non-caregivers. DCBS will only accept reports
involving a non-caretaker as a perpetrator if the report involves allegations of human traf-
cking and/or female genital mutilation. SOP 2.3-Acceptance Criteria also states: Child sex
trafcking when a non-caretaker is the alleged perpetrator involves any sex act involving
a minor in exchange for anything of value. This includes but is not limited to cash, drugs,
jewelry, clothing, food, shelter, protection, or transportation. This could also include the
offer or intent to exchange something of value for sexual favors.
Services
Kentucky had the opportunity to expand Family Preservation Program (FPP) services further
to serve more families and train further in Family First Prevention Services Act (FFPSA)
evidence-based practices (EBPs), through use of state general funds in calendar year (CY)
2022. FPP expanded in calendar year 2022 to serve additional families through an open
solicitation, allowing for providers to submit proposals including budgetary needs to address
barriers to stafng capacity. Additionally, the agency’s budget biennium request included an
ask for an additional $11,491,000 in funding for state scal year (SFY) 2023, and an addi-
tional $16,323,000 in funding for SFY 2024.
As a result of advocacy efforts for greater focus on prevention, DCBS received an additional
$20 million appropriation of state general funds to be utilized for prevention services in SFY
2022, allowing expansion of the Kentucky Strengthening Ties and Empowering Parents
(KSTEP) program.
Parent engagement meetings (PEMs) were implemented in 11 rural areas in calendar year
2022 thanks to additional prevention state general funds and Community-Based Child Abuse
Kentucky (continued)
Child Maltreatment 2022
Appendix d: State Commentary 187

Prevention (CBCAP) funding through the American Rescue Plan Act (ARPA). Discussions
among DCBS leadership continue regarding the prioritization of funding for all prevention
services, including PEMs.
Kentucky received a grant award in the amount of $7.9M to support FFPSA implementation.
The department originally intended to use these funds for FPP expansion. The Consolidated
Appropriations Act granted 100 percent federal reimbursement to states for FFPSA EBPs
through 9/30/2021. Twenty million dollars ($20M) was also appropriated from state general
funds to the department for FFPSA through SFY 2022. Therefore, grant funds were no
longer needed. A portion of these funds was used to support Qualied Residential Treatment
Program (QRTP) implementation in the form of stipends to QRTP providers struggling
nancially due to pandemic related challenges, including stafng. The remaining balance of
$5,768,487 in Family First Transition Act (FFTA) funds must be used by 9/30/2025. This is
100 percent federally funded and cannot be used for services for which a title IV-E claim will
also be submitted.
Activities for title IV-E EBP identication were successful but require ongoing assessment
of the needs of Kentucky families and plan amendment to make changes as needed. A Title
IV-E State Prevention Plan amendment was approved in CY 2021, to include expanded use
of motivational interviewing (MI) and High-Fidelity Wraparound. Another amendment was
submitted to the Children’s Bureau in March 2022 to add Intercept as an EBP, with approval
pending.
The Department is using supplemental funding to provide additional services and supports
to families across the state. Supplemental CBCAP funding has been used to expand services
under Community Collaboration for Children (CCC), which is available in all parts of the
state but especially critical in rural areas where other services may be sparse. The goal is
to decrease CCC in-home services waitlists, provide concrete supports for families, expand
PEMs, and enhance primary prevention efforts through the local regional networks.
Kentucky is one of the jurisdictions selected for the Thriving Families, Safer Children
initiative. These supplemental CBCAP funds will support this initiative. CBCAP aligns
with Thriving Families, Safer Children for primary and secondary prevention. The goal in
Kentucky will be to increase the availability of supports, services, and resources within local
communities to assist families in becoming successful in raising safe and healthy children,
while enhancing the well-being of families. The funds must be obligated by September 30,
2025 and liquidated by December 30, 2025.
Kentucky invested $9.5 million in tertiary prevention services from SFY 2019 to present,
along with leveraging partnerships with other agencies to serve target populations. Sobriety
Treatment and Recovery Teams (START) and KSTEP both expanded through partnership
with the Kentucky Opioid Response Effort (KORE) through funding from the Department
for Behavioral Health, Developmental and Intellectual Disabilities (DBHDID) Substance
Abuse and Mental Health Services Administration (SAMHSA) grant to serve geographic
areas of need and additional families. Both programs were sustained beyond the title IV-E
waiver demonstration project to assist Kentucky families affected by substance use disorder;
cases often resulting in removal absent these services. KSTEP expanded from four counties
Kentucky (continued)
Child Maltreatment 2022
Appendix d: State Commentary 188

to eight counties, from eight to 15, and an entire service region, since SFY 2019, with plans to
expand to two additional service regions. Kentucky also expanded in CY 2021 to include an
additional prevention pilot to deliver Multisystemic Therapy (MST) in two service regions,
with plans for two additional providers in two additional service areas.
Many of Kentucky’s prevention services are provided by contracted service providers. As
identied in the ve-year FFPSA Prevention Plan, children meeting Kentucky’s foster care
candidacy denition total over 27,000, with Kentucky having the capacity to meet 1/5 of the
need with contracted prevention services. Kentucky continues to pursue diligent efforts to
expand child welfare contracted prevention services, including stakeholder partnership and
advocacy for additional funding from the legislature.
Kentucky (continued)
Child Maltreatment 2022
Appendix d: State Commentary 189

Louisiana
Contact Steven Lane Phone 318–676–7800
Title Business Analytics Specialist Email
steven.lane.dcfs@la.gov
Address Department of Children and Family Services
1525 Faireld Avenue, Room 874
Shreveport, LA 71101–4388
General
The Louisiana Department of Children and Family Services (DCFS) continues to review and
revise the methodology used to extract the Child File. These changes often reect system
enhancements that have been completed since the previous submission, requiring updates to
how DCFS data is mapped. Further, the Department revises the extraction process to address
identied gaps in reporting as well possible corrections to errors identied during the extrac-
tion process to improve overall data quality.
Louisiana employs only one type of screened-in response, Child Protection Assessment and
Services (CPS). The CPS program uses the same safety and risk assessment instruments and
documentation protocols for all screened-in reports.
In August of 2018, the Department implemented a new case management system to capture
data related to intake reports and investigations. As with all system implementation, a num-
ber of issues were identied. For example, the Department continues to nd issues related to
the report date and time as well as the date and time initiation of the investigation. This was
noted because of military time discrepancies discovered during the error clean-up process.
Most of these discrepancies were able to be handled for the FFY 2022 submission; however
this remains an area requiring review each submission.
The Department is currently in the planning phase of implementing a new CCWIS system to
capture all NCANDS requirements in an effective and efcient manner.
Reports
In Louisiana, referrals of child abuse and neglect are received through a centralized intake
center that operates on a 24-hour basis. The centralized intake worker and supervisor review
the information using a structured, safety model tool to determine whether the case meets the
legal criteria for intervention. Referrals are screened in if they meet three primary criteria for
case acceptance:
■ A child victim younger than 18 years
■ An allegation of child abuse or neglect as dened by the Louisiana Children’s Code
■ The alleged perpetrator meets the legal denition of a caretaker of the alleged victim
The primary reason for screened-out referrals is that either the allegation or the alleged
perpetrator does not meet the legal criteria. Newborns affected by the mother’s use of a
controlled dangerous substance taken in a lawfully prescribed manner are also screened out,
and reported in the Agency File. Some intake reports are neither screened-out nor accepted.
These additional information reports are often related to active investigations, in-home
services cases, or out-of-home services cases. Generally, if a second report is received and is
still under investigation, the second report is classied as an additional information report.
Child Maltreatment 2022
Appendix d: State Commentary 190

The Department uses a 4-pronged Response Priority system; the four separate priorities are
Priority 1 (contact within 24 hours), Priority 2 (contact within 48 hours), Priority 3 (contact
within calendar 3 days), and Priority 4 (contact within 5 calendar days). Louisiana no longer
employs the Alternative Response model.
The NCANDS disposition of substantiated investigation case is coded in the state as having
a disposition of valid. When determining a nal nding of valid child abuse or neglect, the
worker and supervisor review the information gathered during the investigation and if any of
the following answers are “yes,” then the allegation is valid:
■ An act or a physical or mental injury which seriously endangered a child’s physical, mental
or emotional health and safety; or
■ A refusal or unreasonable failure to provide necessary food, clothing, shelter, care, treat-
ment or counseling which substantially threatened or impaired a child’s physical, mental,
or emotional health and safety; or a newborn identied as exposed to chronic or severe use
of alcohol; or, the unlawful use of any controlled dangerous substance or in a manner not
lawfully prescribed; and,
■ The direct or indirect cause of the alleged or other injury, harm or extreme threat of
harm is a parent; a caretaker as dened in the Louisiana Children’s Code; a person who
maintains an interpersonal dating or engagement relationship with the parent/caretaker/
legal custodian; or a person living in the same residence with the parent/caretaker/legal
custodian as a spouse, whether married or not.
The NCANDS disposition of unsubstantiated investigation case is coded in the state as
having a disposition of invalid. This disposition is dened as a case with no injury or harm,
no extreme risk of harm, insufcient evidence to meet validity standard, or a non-caretaker
perpetrator. If there is insufcient evidence to meet the agencies standard of abuse or neglect
by a parent, caretaker, adult household occupant, or person who is dating or engaged to a
parent or caregiver, the allegation shall be found invalid. If there is evidence that any person
other than the parent, caretaker, or adult household occupant has injured a child with no
culpability by a parent, caregiver, adult household occupant, or a person dating/ engaged to
one of the aforementioned, the case will be determined invalid.
It is expected that the worker and supervisor will determine a nding of invalid or valid
whenever possible. For cases in which the investigation ndings do not meet the standard for
invalid or valid, additional contacts or investigative activities should be conducted to deter-
mine a nding. When a nding cannot be determined following such efforts, an inconclusive
nding is considered. It is appropriate when there is some evidence to support a nding that
abuse or neglect occurred but there is not enough credible evidence to meet the standard
for a valid nding. The inconclusive nding is only appropriate for cases in which there
are particular facts or dynamics that give the worker or supervisor a reason to suspect child
abuse or neglect occurred.
In addition to the ndings noted above, Louisiana also employs the use of an Unable to
Locate nding and a Client Non-Cooperation nding. The Unable to Locate nding is used
when the Department has made extensive efforts to locate the alleged victim and their family.
For example, attempted in-person contact at the address supplied by the reporter and other
Louisiana (continued)
Child Maltreatment 2022
Appendix d: State Commentary 191

addresses found via a global record search (SNAP, FITAP, Medicaid, etc.) and Consolidated
Lead Evaluation and Reporting search (CLEAR); attempted contact via phone; or a neighbor
or relative is unable to provide information on the client’s whereabouts. If the Department is
unable to locate the family after these efforts, this nding may be used.
A nding of Client Non-Cooperation shall be used only in instances in which the
Department is completely thwarted in attempts to complete the investigation by the parents’
refusal to participate in the investigation. Several conditions need to be met to use this nd-
ing: (1) the worker has made reasonable effort to interview the client; (2) Law enforcement
has not been able to assist or refused to assist with efforts to interview the client; and, (3) the
district attorney has chosen not to pursue further action; or, (4) the court has refused to order
the client to cooperate.
Children
During 2022 there were no changes to Child Protective Services policies related to conduct-
ing investigations due to the continued pandemic. However, there might have been some
instances where response time was affected due to COVID-19 exposure of families and
face-to-face contact needing to be delayed.
The Department implemented a new case management system in 2018. During that time,
the ability to identify victims of juvenile sex trafcking was made possible through the
implementation of a new category of child abuse and neglect. Louisiana reports information
on victims with parent/caretaker perpetrators; those victims are substantiated for the respec-
tive Human Trafcking allegation when the parent or caretaker is found to be culpable in the
alleged sexual trafcking incident.
Increased focus has gone to drug and alcohol affected newborns. Identication of drug and
alcohol use by the parents has been identied as a risk factor. However, reporting in this area
has been difcult due to some issues leading back to one distinct problem: Identication of
the reporter as medical personnel. Very often, the hospital social worker calls as opposed to
a doctor or nurse. Centralized Intake Staff have been given additional training in this area
to correctly identify the reporter type as medical personnel, rather than social services. A
number of Plan of Safe Care and Referral cases have been dropped as a result of this issue.
Further, staff will be given additional guidance regarding when to identify a plan of safe care
as being in place.
The agency has provided more guidance on public awareness on Human Trafcking due to
Act 622 that was passed during the 2022 Regular Legislative Session which could result in
more Human Trafcking reports. The law will go into effect January 1, 2023, and requires
that mandatory reporters shall report all alleged child sex trafcking to DCFS regardless of
whether there is alleged parental or caretaker culpability.
Fatalities
Louisiana saw a 26 percent increase in the number of fatalities from FFY 2021 to FFY 2022.
Louisiana reported 29 fatalities during FFY 2022. Policies around child fatality reviews were
not changed in 2022 and the Child Death Review Panel meetings were able to continue to
conduct operations during the pandemic.
Louisiana (continued)
Child Maltreatment 2022
Appendix d: State Commentary 192

The State Child Death Review panel consists of the state health ofcer or his designee,
the secretary of the Louisiana Department of Health or his designee, the secretary of the
Department of Children and Family Services or his designee, the superintendent of the ofce
of state police or his designee, the state registrar of vital records in the ofce of public health
or his designee, the attorney general or his designee, a member of the Senate appointed by
the president of the Senate, a member of the House of Representatives appointed by the
speaker of the House of Representatives, the commissioner of insurance or his designee,
the executive director of the Highway Safety Commission of the Department of Public
Safety and Corrections or his designee, the state re marshal or his designee, the Assistant
Secretary of the Ofce of Behavioral Health of the Louisiana Department of Health or his
designee, a representative of the Louisiana Partnership for Children and Families, a district
attorney appointed by the Louisiana District Attorneys Association, a sheriff appointed by
the Louisiana Sheriff’s Association, a police chief appointed by the Louisiana Association
of Chiefs of Police, a forensic pathologist certied by the American Board of Pathology and
licensed to practice medicine in the state appointed by the chairman of the Louisiana State
Child Death Review Panel subject to Senate conrmation, a pathologist experienced in pedi-
atrics appointed by the Louisiana Pathology Society, a coroner appointed by the president of
the Louisiana Coroner’s Association, the state superintendent of education or his designee,
the director of the bureau of emergency medical services of the Louisiana Department of
Health or his designee, and six persons appointed by the governor, subject to Senate conr-
mation, for a term of three years as follows:
■ A health professional with expertise in Sudden Infant Death Syndrome appointed from a
list of three names submitted by the Louisiana State Medical Society.
■ A pediatrician with experience in diagnosing and treating child abuse and neglect
appointed from a list of three names submitted by the state chapter of the American
Academy of Pediatrics.
■ Four citizens from the state at large who represent different geographic areas of the state.
Perpetrators
The current method of extracting NCANDS data captures perpetrator involvement in family
investigation cases, but does not capture perpetrator relationship to child victims. Therefore,
perpetrator relationship is reported as unknown for the majority of cases.
Services
The Child Welfare agency provides post-investigation services such as foster care, adoption,
in-home family services, and protective daycare. Many services are provided through con-
tracted providers and are not reportable in the Child File. To the extent possible, the number
of families and children receiving services through Title IV–B funded activities are reported
in the Agency File.
Louisiana (continued)
Child Maltreatment 2022
Appendix d: State Commentary 193

Maine
Contact Leigh-Anne Bordas Phone 207– 624 –7911
Title Information Services Manager Email
leigh-anne.bordas@maine.gov
Address Ofce of Child and Family Services
Maine Department of Health and Human Services
2 Anthony Avenue, 11 State House Station
Augusta, ME 04333–0011
General
Maine continues to utilize the Structured Decision Making (SDM) Intake Screening and
Response Priority Tool. It ensures that all reports received are investigated for meeting the
statutory threshold for an in-person Ofce of Child and Family Services (OCFS) response. It
identies how quickly to respond, and the path of response.
Reports
All reports, including reports that are not appropriate, and are referred to as screened out,
are documented in the Comprehensive Child Welfare Information System (CCWIS). The
screening decision is performed at the Intake Unit using the SDM Tool. Reports that do not
meet the statutory denition of child abuse and/or neglect and which the criteria for appropri-
ateness of child abuse /neglect report for response is not met, are preliminarily screened out.
The Maine statutory denition of child abuse and/or neglect is a threat to a child’s health or
welfare by physical, mental or emotional injury or impairment, sexual abuse or exploitation,
deprivation of essential needs or lack of protection from these or failure to ensure compliance
with school attendance requirements under Title 20–A, section 3272, subsection 2, paragraph
B or section 5051–A, subsection 1, paragraph C, by a person responsible for the child.
Maine’s report investigation start date is dened as the date and time (in hours and minutes)
of the rst face-to-face contact with an alleged victim. The SDM tool provides the appro-
priate response time required by child protective services, either 24 or 72 hours from the
approval of a report as appropriate for child protective services.
Children
The state documents all household members and other individuals involved in a report. Some
children in the household do not have specic allegations associated with them, and so are
not designated as alleged victims. These children are now included in the NCANDS Child
File for Maine.
For Maine, the NCANDS Child File category of victims includes children with the state
dispositions of both indicated and substantiated. The term indicated is used when the
maltreatment found is low to moderate severity. The term substantiated is used when the
maltreatment found is high severity.
Fatalities
In FFY 2019 Maine began the collection and ability to track child deaths at time of report,
during investigation or while in care. This information is now available in the NCANDS
Child File for deaths that occurred after June 2019. Various state ofces, along with the
multi-disciplinary child death and serious injury review board continue to share and compile
child fatality data.
Child Maltreatment 2022
Appendix d: State Commentary 194

Perpetrators
Relationships of perpetrators to victims are designated in the CCWIS system. Perpetrators
receive notice of their rights to appeal any maltreatment nding. Low- to moderate-severity
ndings (indicated) that are appealed result in only a desk review. High-severity ndings
(substantiated) that are appealed can result in an administrative hearing with due process.
Services
Only services through a Child Welfare approved service authorization are included in the
NCANDS Child File. Maine continues to work with our contracted agencies for the future
reporting of child/family prevention services in an NCANDS Child File.
Maine (continued)
Child Maltreatment 2022
Appendix d: State Commentary 195

Maryland
Contact Hilary Laskey Phone 410–767–7788
Title Deputy Executive Director of Operations Email
hilary.laskey@maryland.gov
Address Division Department of Human Services
Social Services Administration
311 West Saratoga Street
Baltimore, MD 21201
General
Maryland’s Department of Human Services Social Services Administration fully transitioned
from SACWIS to CCWIS in FFY 2020. This has allowed for changes in data collection
and mapping which have improved the state’s NCANDS submission. In preparing for other
federal reporting changes, modications have been made in required data elds that have
and will continue to improve future NCANDS submissions. Additionally, Maryland has
been working closely with local jurisdictions to ensure that initial face-to-face contacts are
documented timely as this was also part of Maryland’s program improvement plan which has
also improved the current NCANDS submission process.
In an effort to ensure better NCANDS outcomes, Maryland has an extensive CFSR local
review process, in which Maryland partners with the University of Maryland School of
Social Work, to conduct case reviews and local site reviews including interviews with fami-
lies and local partners. The state coordinates this effort in partnership with the Children’s
Bureau and as necessary develops program improvement plans with local jurisdictions that
helps align all the jurisdictions with critical federal and state expectations for child safety,
permanence, and well-being.
Maryland’s current CPS response follows the same rules for Alternative or Investigative
Response:
■ Alleged perpetrators and alleged victims are noted in the record;
■ Alleged child victims must be seen within 24 hours when abuse is alleged, and within 5
days when neglect is alleged;
■ Child safety and risk of maltreatment must be assessed;
■ The CPS response must be completed within 60 days; and
■ Additional services may be offered including in-home or out-of-home services.
Alternative Response targets low risk reports of child neglect and abuse, and although the
alleged victims and alleged perpetrators are noted in the record, the case does not establish
ndings concerning maltreatment, nor are the children receiving Alternative Response
coded as victims. Instead, alternative response allows local departments of social services
to help Maryland families to access services, supports and other assistance that will address
their concerns. Families screened in for CPS who are eligible but refuse to participate in
Alternative Response are reassigned to Investigative Response.
Investigative Response targets moderate to high-risk reports of child neglect and abuse which
results in a nding concerning maltreatment. This is Maryland’s traditional CPS investiga-
tion. Maryland has improved NCANDS data mapping for its CPS functionality in CJAMS.
Child Maltreatment 2022
Appendix d: State Commentary 196

Reports
Maryland’s number of referrals increased in FFY 2022 from FFY 2021 which is thought to
be due to resumption of in person education. Children with increased access to education
personnel in condential settings allowed for children to disclose alleged abuse or neglect,
which led to an increase in the reports. There were also resumption of in person mental
health and physical health appointments which allowed for increase in reports from those
mandated reporters.
Due to the enactment of a legislative bill , Maryland implemented a centralized reporting
hotline for Child Protective Services in 2021. This centralized hotline has provided a single
number for Marylanders to report suspected abuse or neglect with the ability to then route
the calls to the appropriate local jurisdiction based on the location of the allegation. The
local jurisdiction’s previous child protection numbers remained in service, allowing those to
continue to be used by those who were already familiar with them, thus providing options for
reporting suspected child abuse or neglect.
Children
Maryland regulations require that all children in a household are interviewed/assessed during
an investigation or alternative response. The time frame for these interviews/assessments of
children not initially identied as victims vary depending on the type of response.
Maryland does have a check box in place in the SDM tool to count sex trafcking: when
a caseworker chooses sexual abuse, the case worker is able to choose “yes” or “no” as to
whether it was sex trafcking. Prior mapping from Maryland’s SACWIS had not been able
to separate out the sex trafcked maltreatment. Maryland will make changes with regards to
mapping so that identication of these children can be reported in future submissions.
Several years ago, Maryland made the decision to not investigate infants where prenatal
substance abuse exposure was the only concern. These children receive a risk of harm
assessment and are reported as part of the agency le. Only in situations where additional
factors that meet abuse or neglect criteria will infants with perinatal substance abuse be
reported in the child level le. This makes it appear as if Maryland does not have many
infants with perinatal substance abuse. The plan of safe care for these infants continues
to undergo development in the state’s CCWIS and it is hoped that this will be able to be
reported in subsequent years.
Fatalities
Maryland requires that child fatalities where child maltreatment is a factor are reported by
the local departments of social services. In addition, the state and local departments also
get information about these fatalities from local agency fatality review teams, the Maryland
Department of Health’s Child Fatality Review team, and the ofce of the Chief Medical
Examiner. Any suspicious death is investigated while any sleep related death is assessed or
investigated if suspicious. Maryland is continuing to work on a centralized review for fatali-
ties where maltreatment was a factor.
Maryland (continued)
Child Maltreatment 2022
Appendix d: State Commentary 197

Over the past year, there has been a focus on ensuring that documentation of child death
is recorded in the CCWIS which has improved the state’s ability to report these deaths in
the child level le instead of having to report them in the agency le. This has improved
NCANDS reporting for FFY 2022.
Perpetrators
Maryland currently does not have a minimum age for a perpetrator, however the age differ-
ence and difference in ability would be taken into consideration and often in the nding, the
perpetrator would be unnamed and indicated more often than naming the youth offender.
On the other hand, when a perpetrator’s age is unknown, Maryland has used a default date of
birth, which is not always updated by the end of the investigation. This has led to the appear-
ance that Maryland has a large number of perpetrators who are over the age of 75. Maryland
will be working to ensure that a better approximation of a perpetrator’s age is documented
prior to the nalization of investigations for next year’s data submission.
Services
When CPS reports are screened out, they are evaluated to determine if the concerns raised in
the report meet criteria for a risk of harm assessment. These criteria include:
■ substance exposed newborns,
■ domestic violence (when a child has not been injured),
■ substantial risk of sexual abuse by a registered sex offender,
■ caregiver impairment,
■ previous death or serious injury of a child due to child abuse or neglect,
■ previous report to CPS and there is currently a child age 5 or under in the home,
■ suspicion of sex trafcking, and
■ adult survivor of maltreatment (where maltreator has children in care and supervision).
These assessments are able to be changed to a CPS case if the assessment indicates that the
information meets CPS criteria. Risk of Harm cases can also be referred to on-going services
to provide support to prevent potential maltreatment in the future.
As our population of children in foster care has been decreasing in the past several years,
Maryland continues to utilized family team decision meetings as well as increase the use
of evidence-based practices (EBP), such as Functional Family Therapy (FFT), Parent Child
Interactive Therapy (PCIT), Multisystemic Therapy (MST), and Healthy Families America
(HFA), which were identied in Maryland’s Family First Prevention Services Act (FFPSA)
Prevention Plan to address a holistic approach to family needs. These EBPs were rolled out
throughout the state in stages, utilizing those that were already in place following the Title
IV-E Waiver and then implementing services in other jurisdictions across the state.
Maryland (continued)
Child Maltreatment 2022
Appendix d: State Commentary 198

Massachusetts
Contact Nicholas Campolettano Phone 508–929–2013
Title Management Analyst
Ofce of Management, Planning, and Analysis
Email
Address Massachusetts Department of Children and Families
600 Washington Street
Boston, MA 02211
Reports
The Department’s Protective Intake Policy requires non-emergency reports of abuse and
neglect to be reviewed and screened in or out in one business day. Emergency reports require
an immediate screening decision and an investigatory response within 2 to 4 hours.
Massachusetts uses a single child protection response, with all screened in reports of
suspected child abuse and neglect (51A reports) assigned to investigation-trained response
workers. This places the decision making regarding the appropriate level of departmental
intervention after the response—the point at which the Department has interviewed the
child and caregiver involved, contacted collaterals, and substantially investigated the report
of abuse or neglect. Emergency responses must be completed in 5 working days; non-
emergency responses must be completed in 15 workings days. To complete an investigation,
the policy mandates the use of the Department’s Risk Assessment Tool to assess potential
future safety risks to the child. In October 2019, the Department updated its Risk Assessment
Tool to incorporate the latest validated research to assess child safety risk more effectively
and reliably.
The number of screening and initial assessment/investigation workers listed is the estimated
full-time equivalents (FTE) based on the number of screenings and initial assessments/inves-
tigations completed during the federal scal year (FFY), divided by the monthly workload
standard for the activity, divided by 12. The workload standards are 55 screenings per month
and 10 investigations per month. The number includes both state staff and staff working
for the Judge Baker Children’s Center, Massachusetts’ Child-At-Risk Hotline contractor.
The hotline handles child protective service functions whenever state ofces are closed.
The number of workers completing assessments was not reported because assessments are
case-management activities rather than screening, intake, and investigation activities. In FFY
2022, social workers also performed screening and investigation functions in addition to
ongoing casework.
Children
In Massachusetts, intake screening and response decisions require the lowest legal threshold,
or level of proof, of “reasonable cause”, as required by Massachusetts state law. This allows
for the capture of a broader view of children potentially in need of protective services.
Response outcomes are mapped to NCANDS outcomes as follows:
■ Supported is mapped to Substantiated
■ Substantiated Concern is mapped to Other
■ Unsupported is mapped to Unsubstantiated at the report level and to Unsubstantiated at
the allegation level if the report decision is either Supported or Unsupported. If the report
decision is Substantiated Concern, an allegation decision of Unsupported is mapped to
Other.
Child Maltreatment 2022
Appendix d: State Commentary 199

The NCANDS category of neglect includes medical neglect; Massachusetts does not have a
separate allegation type for medical neglect. Living arrangement data are not collected dur-
ing investigations with enough specicity to report, except for children who are in placement.
Data on child health and behavior are collected, but these data need not be entered during an
investigation. Data on caregiver health and behavior conditions are not usually collected dur-
ing an investigation. For both the alcohol and drug abuse elements, the indicator is marked
as a “yes” for any information found in the health and behavior sections of the case record
and for any infant with a reported allegation of Substance Exposed Newborn or Substance
Exposed Newborn-Neonatal Abstinence Syndrome.
Since 2014, Massachusetts has engaged in a comprehensive approach to address Human
Trafcking and Sexual Exploitation of children and youth that has included:
■ Updating multiple policies to integrate understanding, identifying and responding to child
trafcking.
• Accepting reports of allegations against non-caretaker alleged perpetrators.
• Since the implementation of the new protective intake policy in 2016, the identied
perpetrators have mostly been non-relatives—the relationships are identied in the
Department’s system as “unknown” or “other person.”
■ Training of child welfare staff and community partners.
■ Maintaining an internal intranet page (available to all child welfare staff) that provides tip
and fact sheets related to Human Trafcking and Sexual Exploitation of children.
■ Implementing a Multi-Disciplinary Team model that primarily consists of Child Advocacy
Centers, the Department, and law enforcement representatives, and includes numerous
community partners.
• Child Advocacy Centers cover the entire state and there is a Human Trafcking
Coordinator within each Center.
Changes to iFamilyNet, Massachusetts’ electronic case record system were implemented in
FFY 2020 to allow for the documentation of the presence of Plans of Safe Care and Referrals
to Appropriate Services (for families of Substance Exposed Infants) during the report or
investigation. Additionally, this information can also be captured and detailed during the
Family Assessment and Action Plan that occurs on cases open for services.
Fatalities
Massachusetts reports child fatalities attributed to maltreatment only after information is
received from the state’s Registry of Vital Records and Statistics (RVRS). RVRS records
for cases where child maltreatment is a suspected factor are not available until the medical
examiner’s ofce determines that child abuse or neglect was a contributing factor in a child’s
death or certies that it is unable to determine the manner of death. Information used to
determine if the fatality was due to abuse or neglect may also include data compiled by the
Department’s’ Case Investigation Unit, reports of alleged child abuse and neglect led by the
state and regional child fatality review teams convened pursuant to Massachusetts law, and
law enforcement.
As these data are not available until after the NCANDS Child File must be transmitted, the
state reports a count of child fatalities due to maltreatment in the NCANDS Agency File.
Massachusetts (continued)
Child Maltreatment 2022
Appendix d: State Commentary 200

Massachusetts only reports fatalities due to abuse or neglect if an allegation related to the
child’s death is supported.
Services
Data are collected only for those services provided by the Department. The Department may
be granted custody of a child who is never removed from home and placed in substitute care.
In most cases when the Department is granted custody of a child, the child has an appointed
representative. Representative data are not always recorded in iFamilyNet.
Massachusetts (continued)
Child Maltreatment 2022
Appendix d: State Commentary 201

Michigan
Contact Theresa Keyes Phone 517–574–2257
Title State Administrative Manager Email
keyest@michigan.gov
Address Division of Continuous Quality Improvement
Michigan Department of Health and Human Services
Children’s Services Agency
235 South Grand Ave Suite 505
Lansing, MI 48933
Contact Cynthia Eberhard Phone 517–896–6213
Title Child Welfare Data Manager Email
eberhardc@michigan.gov
Address Michigan Department of Health and Human Services
Michigan Statewide Automated Child Welfare Information System
222 North Washington Square, 1st Floor
Lansing, MI 48933
General
The Michigan Department of Health and Human Services (MDHHS) does not have a dif-
ferential response or alternate response program. MDHHS is responsible for the investigation
of complaints of child abuse and neglect allegedly committed by a person responsible for the
child’s health and welfare.
Michigan has begun to implement the commitments outlined in the Families First Prevention
Services Act instituting in three pilot communities a transfer of abuse or neglect complaints
to the United Way 211 when the complaints do not rise to the level for concern of child abuse
or neglect per state law, but indicate that the family may need prevention services.
Reports
Michigan has implemented a Structured Decision-Making protocol at the statewide
Centralized Intake Division, the twenty-four-hour hotline responsible for taking all child and
adult abuse or neglect concerns.
The decision tool routes families to prevention services to keep children and youth safe in
their own communities by establishing a system rooted in family well-being, prevention, and
equity. This initiative, MiFamily, Stronger Together, will require a signicant culture shift,
moving away from a reactive child protection system and toward a prevention-oriented, fam-
ily well-being system. Michigan has observed a slight increase, 12 percent, of referrals being
screened out since implementing a prevention-oriented system of care within Centralized
Intake.
Children
Michigan has been able to report victims of sex trafcking since scal year 2018, dened
as an individual subject to the recruitment, harboring, transportation, provision, obtaining,
patronizing, or soliciting of a person for the purposes of a commercial sex act or who is a
victim of a severe form of trafcking in persons in which a commercial sex act is induced by
force, fraud, or coercion, or in which the person induces to perform the act is under 18 years
old. In addition, Michigan denes labor trafcking as the recruitment, harboring, transporta-
tion, provision, or obtaining of a person for labor or services, using force, fraud, or coercion
for the purpose of subjection to involuntary servitude, peonage, debt bondage, or slavery.
Child Maltreatment 2022
Appendix d: State Commentary 202

Michigan has reported data for infants with prenatal substance exposure since scal year
2018. The state policy indicates that Child Protective Services will investigate complaints
alleging that an infant was born exposed to substances not attributed to medical treatment
and subsequent requirements for conrming abuse/neglect must nd that a parent’s substance
use/abuse impacts child safety/well-being. Michigan continues to collaborate with the
medical community, staff and Governor’s appointed task force to review and update policy,
process, and reporting requirements to ensure families impacted are offered a Plan of Safe
Care through either a public health or child welfare contact.
Fatalities
Michigan has observed an increase in the total number of child fatalities in scal year 2022 at
61 compared to 35 in scal year 2021 and 43 in scal year 2020. Some observations include:
■ 11 youth died in federal scal year 2021 while the investigation disposition took place in
federal scal year 2022 and therefore was included in FY 2022 report.
• 7 of the 11 fatalities occurred near the end of the reporting period.
■ 3 sets of siblings totaling 7 youth are included in the total count of child fatalities.
■ Concurrent criminal investigations impact nal determination on causality of a child
fatality.
Michigan reports child fatalities within the Child File where there is a nding of preponder-
ance outlined by category dispositions or ndings noted as a Category 1, 2, or 3. In 2022, a
total of 57 children were reported within the Child File. Michigan does not conrm persons
not responsible as dened by statute or deceased persons as perpetrators. Four child fatalities
met these criteria and have been reported within the Agency File.
Michigan participates in the Safe Systems Review program, an interagency collaborative
with multiple jurisdictions aimed at systemic improvements within child welfare systems.
Perpetrators
Perpetrators are dened as persons responsible for a child’s health or welfare who have
abused or neglected a child.
Michigan does not report non-caregiver perpetrators of sex trafcking referring these adults
to law enforcement. This population does not meet criteria of “nonparent adult” or “person
responsible” as dened in Michigan’s Child Protection Law. The exception to this is when
law enforcement is the reporting source, and they are reporting child trafcking concerns. In
these instances, Centralized Intake is required to assign the referral for investigation and the
eld determines if the person is responsible and can be substantiated.
Services
Michigan continues to provide prevention and preservation services through statewide
programing by Families First of Michigan, Family Reunication Program, and Families
Together Building Solutions-Pathways of Hope as well as local programming.
Michigan has begun to implement the Family First Prevention Services Act (FFPSA)
plan outlining ten Evidenced Based Practices to implement over time. Home Visiting
and Motivational Interviewing are the rst two practices implemented. The MiSACWIS
Michigan (continued)
Child Maltreatment 2022
Appendix d: State Commentary 203

application has been updated allowing prevention services data to be collected and tracked.
Michigan has a longstanding relationship with private agency providers to deliver all FFPSA
services.
Michigan refers children birth through age three to programs under the Individuals with
Disabilities Education Act (IDEA). IDEA is managed within the Michigan Department of
Education and data is not available to report within the agency le.
Michigan (continued)
Child Maltreatment 2022
Appendix d: State Commentary 204

Minnesota
Contact Yer Chang Phone 651–431–3292
Title Supervisor of Research, Evaluation and Change
Management Units
Child Safety and Permanency Division
Email
Address Minnesota Department of Human Services
444 Lafayette Road
Saint Paul, MN 55155
General
Minnesota has three response paths to reports of alleged child maltreatment, currently
referred to as family assessment response, family investigative response, and facility
investigative response. Reports alleging substantial child endangerment or sexual abuse, as
dened by Minnesota statute, require an investigative response. Child protection workers
must document the reason(s) for providing an investigative response which may include:
statutorily required due to allegations of substantial child endangerment or sexual abuse, or
discretionary use for reasons such as the frequency, similarity, or recentness of reports about
the same family. Family assessment response deals with the family system in a strengths-
based approach and does not substantiate or make determinations of whether maltreatment
occurred; however, a determination is made as to whether child protective services (CPS) are
needed to reduce the risk of any future maltreatment of the children. Acceptance into either
response path, family assessment or investigative, means that a report has been screened
in as meeting Minnesota’s statutory denition of alleged child maltreatment, so allegations
accepted for either response are reported through NCANDS.
Reports
Data on CPS staff represent the full-time equivalent (FTE) of staff as reported by local
agencies (counties, combined agencies, and two tribal agencies). In Minnesota, child protec-
tion staff are employees of the local agencies rather than the state. Overall, local agencies
reported a slight decrease in the number of child protection staff compared to last year, while
the number of supervisory staff remained the same. It is difcult to generalize the impact
COVID-19 had on the child protection workforce in Minnesota due to regional and county
Covid-19 experiential impact and variation.
Reports of child maltreatment are made directly to local child welfare agencies (counties
and two tribal agencies). All three responses (family and facility investigations, and fam-
ily assessment) apply to screened-in reports of alleged child maltreatment in Minnesota.
There was not a signicant difference in the proportion of reports screened to each type
of response. A separate program, Parent Support Outreach Program (PSOP), offers early
intervention supports and services to families when reports alleging child maltreatment are
screened out or a family is voluntarily referred into the program. The number of children
served under this program is reported under preventive services in the Agency File and is
noted below in the services section of this commentary.
The COVID-19 pandemic continued to have an impact on the number of alleged CA/N
reports during FFY 2022. Overall, the number of reports continued to decline slightly from
the previous year, however, there were regional and county variances; likely correlated
to patterns of virtual/distance school programming. While no changes were made to the
statutory requirements for reporting and screening for maltreatment, multiple successive
Child Maltreatment 2022
Appendix d: State Commentary 205

Executive Orders from the Governor during the State’s peacetime emergency required
individuals, organizations, and businesses to intermittently “stay at home,” shutdown, and/
or engage in virtual services and education. While the State’s peacetime emergency ended on
July 1, 2021, it is likely that the physical absence of children and youth from schools, doctor’s
ofces, places of worship and other places minimized exposure to mandated reporters result-
ing in a reduction in reports of alleged CA/N.
The vast majority of referrals are screened out because the stated concerns do not meet
established criteria in Minnesota’s Child Maltreatment Intake, Screening, and Response Path
Guidelines or the denitions of child abuse or neglect under Minnesota law. Other reasons
to screen out a referral include: children not in the county’s jurisdiction, allegations have
already been assessed or investigated, not enough identifying information was provided, or
the incident did not occur within the family unit or a licensed facility. There is little variation
in the proportion of screened out referrals for each of the reasons across years. In addition,
Minnesota Screening and Response Path Guidelines and statute apply screen-in requirements
to children who have been born. Screened in reports alleging substantial child endangerment
or sexual abuse must be responded to within 24 hours. Other reports must be responded to
within 5 days or 120 hours under Minnesota statutes. Reports with either a determination
of maltreatment (substantiation) or a determination of need for child protective services are
retained for 10 years. Reports with neither determination (including all family assessment
response reports) are kept for 5 years. Screened out child maltreatment reports are also kept
for 5 years. Timelines for record retention and destruction are set in Minnesota statutes.
The NCANDS category of “other” report sources include the state categories of
clergy, Department of Human Services (DHS) birth match, other mandated, and other
non-mandated.
Children
During FFY 2022 the number of victims decreased by 4.4 percent. The number of victims
is based on determined/substantiated child victims in investigation cases. In FFY 2022,
the state continued to be affected by the COVID-19 related public health guidelines and
Governor Executive Orders requiring activities to slow the spread of coronavirus, modica-
tions were made to the timelines and face-to-face requirements for certain child protection
responses. For reports of substantial child endangerment or sexual abuse, law enforcement
or hospital staff were permitted to serve as the initial face-to-face contact with alleged
child victims; these exibilities ended on June 30, 2021. Beginning July 1, 2021, exceptions
allowing delayed contact for reports of sexual abuse or substantial child endangerment were
codied. The new exceptions allow child welfare agencies to have face to face contact with
the child within ve calendar days (versus 24 hours) when the child resides in a location
that is conrmed to restrict access with the alleged offender, or the child welfare agency is
pursuing a court order for the caregiver to produce the child for questioning. The department
encouraged face-to-face contacts and indicated that alternative methods should be used
sparingly throughout the state’s peacetime emergency. When alternative methods were used,
video were preferred. Overall, the median time to initial contact throughout the state was
longer compared to last year.
Minnesota (continued)
Child Maltreatment 2022
Appendix d: State Commentary 206

To ensure the safety of all children who have or had contact with an alleged offender,
Minnesota statute requires other children who currently reside with, or who have resided
with, an alleged offender to be interviewed in the early stages of an assessment or investiga-
tion. These children are subject to the same protections and provisions as the alleged victim.
The State currently collects and reports data related to infants with prenatal substance
exposure. While there were no policy changes during FFY 2022, the State has taken efforts
to improve its response through partnerships and communications. The State has also created
a dashboard to monitor data more timely to support strategies for improvement.
Fatalities
In FFY 2022, the number of maltreatment-related fatalities as compared to 2021 increased
from 22 to 25. Given the rarity and complexity of these cases, it would be misleading to
speculate on the reasons for this increase. Each fatality is a tragedy, and it is imperative that
when such an incident occurs, the state have a process for learning what we can to improve
outcomes for all children and families moving forward.
The primary source of information on child deaths resulting from child maltreatment is local
agency child protective services staff; however, some reports originate with law enforce-
ment or coroners/medical examiners. Local agencies also submit results of any local child
mortality review to the department’s critical incident review team. The department’s critical
incident review team also regularly reviews death certicates led with the Minnesota
Department of Health (MDH) and directs local agencies to enter child deaths resulting from
child maltreatment, but not previously recorded by child protective services, into Minnesota’s
Comprehensive Child Welfare Information System, to ensure that complete data are
available.
Occasionally, a child who is a resident of Minnesota becomes the subject of an alleged CA/N
related fatality in another jurisdiction. When the department’s critical incident review team
becomes aware of such an incident, documentation, including police reports, are requested
from law enforcement in the other state. The local agency within Minnesota is asked to
record the data in Minnesota’s Comprehensive Child Welfare Information System.
Minnesota has a critical incident review team that conducts reviews of maltreatment related
child fatalities. The review process, based in human factors and safety science, is a robust,
thorough and time intensive endeavor that includes a review of the child and family’s history
of involvement with the child welfare system. This process results in the identication of
systemic barriers and inuences that impact work occurring in Minnesota’s child welfare
system; this information is used to inform the state’s broader continuous quality improve-
ment efforts. In addition to the critical incident review team, Minnesota has a State Child
Mortality Review Panel. The multidisciplinary team including representatives from state,
local, and private agencies; disciplines represented include social work, law enforcement,
medical, legal, and educators. Other than conducting reviews and meetings virtually, all
other policies and procedures for reviewing child fatalities in Minnesota remained the same
throughout the pandemic.
Minnesota (continued)
Child Maltreatment 2022
Appendix d: State Commentary 207

Perpetrators
The NCANDS category of “other” perpetrator relationships includes other nonrelative. In
Minnesota, maltreatment determinations can be made against children age 10 and older, as
long as there is a preponderance of evidence. Noncaregiver perpetrators of sex trafcking are
included.
Services
Primary prevention services are often provided without reference to individually identied
recipients or their precise ages, so reporting by age is not possible. Clients of an unknown
age are not included as specically children or adults. Data reported in preventive services
funded by Community-Based Child Abuse Prevention (CBCAP) and Promoting Safe and
Stable Families (Title IV-B) represents the unduplicated number of children who received
Parent Support Outreach Program supports and services. Services in this program are
provided to children and families who were reported as having an allegation of child mal-
treatment, but the reported allegation was screened out and did not receive a child protective
response. Community agency referrals and self-referrals are also eligible for the Parent
Support Outreach Program. This program is completely voluntary.
Services offered by local agencies vary greatly in availability between rural and metropolitan
areas of the state. Although all agencies use a statewide service listing, resource development
without a large customer base can be difcult. Cost effectiveness is an issue for providers
who must serve large geographic areas that are sparsely populated.
As a result of the pandemic, the department temporarily lifted age restrictions and decreased
the number of risk factors that were needed to be eligible for the Parent Support and
Outreach Program. In addition, the department increased the amount of funding provided to
local agencies, encouraging a higher amount per family when indicated, and expanded the
eligible supports and services to meet the evolving needs of families during the pandemic,
including technology to participate virtually in services and educational activities.
Minnesota (continued)
Child Maltreatment 2022
Appendix d: State Commentary 208

Mississippi
Contact Tameika Givens Phone 601–576–1614
Title Ofce of Federal Reporting Email
Address Department of Child Protection Services
P. O. Box 346
Jackson, MS 39205
General
Mississippi does not have two types of responses to screened-in referrals (reports).
Reports
There was an increase of reports for FFY 2022 compared to FFY 2021.
MDCPS is constantly hiring and training new staff and rehires to the agency. The hotline
Mississippi Centralized Intake and Assessment began in July 2022, utilizing all contracted
staff for intake positions, utilizing full-time MDCPS employees for most of the intake work-
load, and utilizing contracted part-time staff for intake positions on weekends and holidays.
During the second half of FFY 2022, signicant changes were made regarding using data to
determine stafng amounts for the hotline. The shifts were streamlined into three distinct
shifts for each day, making the data used to determine stafng amounts needed for each shift
clearer and more relevant to inform stafng needs. MDCPS does not employ part time case-
workers or investigators. Full-time equivalents were used as the number of staff responsible
for intake and screening, due to there being a mixture of full-time employees and part-time
contracted staff.
A transition is being made for more of the screening to be done at the intake level, which
is a move away from the current two-part screening system in which initial screening is
conducted at intake and a nal screening is done at the county assignment level. There are
plans to implement a structured decision-making tool in the future. For FFY 2022, there was
an increase in the amount of screening assessment conducted at the intake level, especially
pertaining to whether information on children in open cases constituted a situation of abuse
or neglect by the caregiver, or whether the information pertained to the ongoing casework
management of assessing, monitoring, and managing safety, risks, and well-being.
Children
There was an increase of victims for FFY 2022 compared to FFY 2021, but the increase was
less than 10 percent. While no policy changes were made, guidance was issued for contact
precautions. No policy around response times changed and MDCPS did not observe any
unusual variances in timely initiation or completion of investigations during the pandemic
period and FFY 2022.
MDCPS has reported the human trafcking maltreatment type since FFY 2019. For FFY
2022, there were 273 sex trafcking reports in Mississippi. MDCPS continues to collaborate
with the National Human Trafcking Assessment Team (Hotline and advocates), Local Law
Enforcement, and the Mississippi Attorneys General Ofce. Ongoing efforts will continue to
address human trafcking and additional resources to serve victims.
Child Maltreatment 2022
Appendix d: State Commentary 209

The Comprehensive Addiction and Recovery Act continues to assist mothers and infants
affected by substance use exposure. For FFY 2022, MDCPS continued the Memorandum
of Understanding (MOU’s) with the Mississippi Department of Mental Health, Mississippi
Department of Health, and Healthy Families of Mississippi. These programs combined
offers case/care management services for mothers and infants, parenting education, home
visiting, and substance use treatment (inpatient and outpatient). Additionally, the Healthy
Moms, Healthy Babies program provides support in all 82 counties such as: community
support, Medicaid, SNAP, WIC, Health education for depression, anxiety, and healthy infant
development. The state does not report referrals of infants with prenatal substance exposure
in the NCANDS Child File. For FFY 2022, there were 68 children identied as IPSE. The
CARA referrals are tracked through a software called Smartsheet. The providers, Mississippi
Department of Health, Mississippi Department of Mental Health, and Healthy Families are
sent referrals through DocuSign and comments are made through Smartsheet. Mississippi
Department of Child Protection Services tracks information such as: successful/unsuccessful
attempts of contacting the mother and/or medical provider, and if the mother accept/deny
services. There are no alcohol abuse child risk factor or drug abuse child risk factor reporting
limitations. There are no alcohol abuse caregiver risk factor or drug abuse caregiver risk
factor reporting limitations.
There are no barriers on how Mississippi collects and report data to NCANDS for infants
with prenatal substance exposure.
Fatalities
There was an increase in fatalities for FFY 2022 compared to FFY 2021.The agency devel-
oped a Special Investigations Unit that is responsible for investigating all reports of child
fatalities that meet criteria for agency investigations. Previously, the investigations were
conducted by regular workers in the eld. The development of the SIU has standardized
screening and decision-making processes in fatality investigations. In addition, the investiga-
tors that make up the unit are required to have an advanced level of licensure and experience.
Having the dedicated, specialized investigators has contributed to the increase of fatalities
reported with substantiated ndings of abuse and neglect.
Mississippi previously counted only those fatalities where the medical examiner or coroner
ruled the manner of death was a homicide. In 2007, Mississippi also began counting those
child fatalities determined to be the result of abuse or neglect that has been substantiated
by MDCPS. Other sources that compile and report fatalities due to abuse and neglect are
Serious Incident Reports (SIRs) and Child Death Review Panel (CDRP) facilitated by the
Mississippi Department of Health. Child Death Review meetings are attended by MDCPS
staff and executive leadership responsible.
All fatalities reported to the agency are investigated regardless of the manner of death.
However, all reports accepted for an investigation must have an allegation.
Mississippi (continued)
Child Maltreatment 2022
Appendix d: State Commentary 210

Perpetrators
MDCPS does report non-caregiver perpetrators of sex trafcking to NCANDS. “Other”
perpetrator relationship would be selected when the alleged perpetrator’s relationship to the
victim is known, but it does not t into the other categories listed.
Human Trafcking laws in Mississippi stipulate that child abuse has occurred when a child
is trafcked by any person, whether or not that person is the child’s caregiver. Therefore, the
nonrelative perpetrators of Human Trafcking would be included in reporting.
Services
There were no changes to preventive services funding. Some prevention services are con-
tracted to two providers. These services continue to be outsourced to two Providers. In previ-
ous years, children who received preventive services covered under the Promoting Safe and
Stable Families grant (PSSF) during the year were utilized by the Families First Resources
Centers with some of these funds. The PSSF grant funds a portion of the in-CIRCLE Family
Support Services Program, formally known as CFFSP, or Family Preservation/Family
Reunication/Family Support Services. Beginning on October 1, 2017, the CFSSP transi-
tioned to the in-CIRCLE Family Support Services Program. Two vendors provide services
for this program, however, only one provides services funded through PSSF funds, Youth
Villages. Canopy Children’s Solutions utilized state general funds to provide services.
■ in-CIRCLE is an intensive, home and community-based family preservation, reuni-
cation, and support services program for families with children who are at risk of
out-of-home placement. It is designed and implemented to help break the cycle of family
dysfunction by strengthening families, keeping children safe, and reducing foster care and
other forms of out-of-home placements. Services are also offered to families with pregnant
mothers who were at high risk of the child being removed due to substance use issues once
the child is born.
• The primary goal of the program is to remove the risk of harm to the child rather than
removing the child by (1) reducing unnecessary out-of-home placements, (2) preventing
and/or reducing child abuse and neglect, (3) improving family and informal concrete
supports, (6) addressing mental health and substance use issues, (7) reducing child
behavior problems, and (8) safely reunifying families.
For FFY 2022, the Dorcas In-Home Family Support Program is also another program that
provided family-driven, youth-guided interventions to improve the stability of enrolled fami-
lies and their ability to provide adequate care for the children for whom they are responsible.
These interventions increased families’ access to and utilization of community resources and
assistance. 139 children/ families were served through The Dorcas In-Home Family Support
Program. The Dorcas Program is funded privately through Baptist Children’s Village as
a support to our Preventive programs. It is a no cost to our families as it is provided pro
bono. in-CIRCLE Services through Youth Villages and it is funded through PSSF. Canopy
is funded through General Funds. In Home Services served 445 children/families during
FFY 2022 under the PSSF grant. In addition, 1285 children/families were served through the
General Funds, and 139 families/children were served through the No Cost funds.
Mississippi (continued)
Child Maltreatment 2022
Appendix d: State Commentary 211

Services to child victims outside of a service case are provided through the Family
Reunication and Preservation Program within the In-Home Services Unit of the Agency.
Through Promoting Safe and Stable Families, General State Funds, and No Cost Services.
The total number of children/families served under these preventive services were 802
families and 1869 children. Subgrantees have continued services for this contract year to
provide step-down and soft support; whereby, it promotes less probability of reentry into the
program.
The goal is to reduce the likelihood of removal or other disruption of their living arrange-
ment. The funding stream for the Prevention subgrantees are funded through Community
Based Child Abuse Prevention Grants, (CBCAP). For, the Prevention subgrantees, the
reported numbers for October 1, 2021 — September 30, 2022 were 3, 147 families served
and 4, 362 children served. COVID- 19 continues to be a barrier for many families. However,
grantees resumed face-to-face services. Grantees continued virtual services such as parent-
ing classes/education and the ACT Raising Safe Kids Curriculum. Additionally, Support and
Concrete Groups, Counseling Referrals, Safe Sleep Education, Food Box Give Always, and
various community-based workshops were offered. The Resource Center was also utilized in
addition to case management services.
When a service case is opened and maintained by MDCPS staff, it is referred to as an
In-Home service case. These cases are opened to either maintain successful reunications
after a foster care episode or prevent the need for initial removals from home into foster care.
Mississippi (continued)
Child Maltreatment 2022
Appendix d: State Commentary 212

Missouri
Contact Mary Faucett, Jennifer Gunnels Phone 573–368–2400
Title Senior Social Services Specialist Email
jennifer[email protected]
Address Children’s Division (Dept. of Social Services)
Jefferson State Ofce Building
205 Jefferson Street
Jefferson City, MO 65101
General
The Children’s Division, under the Department of Social Services umbrella, is designated
to direct and supervise the administration of child welfare services. The Children’s Division
works in partnership with families, communities, the courts and other governmental entities
toward ensuring the safety, permanency, and well-being of Missouri children. The division
works with all parties to safely maintain children in their homes whenever possible and
to secure safe, permanent living arrangements when out-of-home placement is necessary.
The Children’s Division administers the Child Abuse/Neglect Hotline, Intensive In-Home
Services, Family Centered Services, Adoption Services, Independent Living, Foster Care,
Residential Licensing and preventive services including early childhood and early interven-
tion strategies. The division is responsible for the assessment and investigation of all reports
to the Child Abuse/Neglect Hotline. These services are administered statewide within a
centralized organizational framework. Children’s Division Responsibilities include:
■ Oversees a 24 hour child abuse and neglect hotline
■ Investigates child maltreatment reports
■ Provides foster care services for maltreated children
■ Provides preventive services to at-risk families
■ Provides intensive family supports for at-risk families
■ Assists with children nding permanency with adoption and guardianship services
Children’s Division Geographical Structure Missouri has 114 counties and the City of St.
Louis, which are grouped together using pre-established judicial circuit boundaries. Each
circuit has oversight by a Circuit Manager. The state is divided into six regions, with each
governed by a Regional Director. The St. Louis Region includes the county and the city of
St. Louis. Missouri’s six regions are: St. Louis, Kansas City, Southeast Region, Southwest
Region, Northeast and Northwest Region.
Missouri operates under a differential response program, where each referral of child abuse
and neglect is screened by the centralized hotline system and assigned to either investigation
or family assessment. Both types are reported to NCANDS.
Investigations are conducted when the acts of the alleged perpetrator, if conrmed, are crimi-
nal violations; or where the action or inaction of the alleged perpetrator may not be criminal,
but if continued, would lead to the removal of the child or the alleged perpetrator from the
home. Investigations include but are not limited to child fatalities, serious physical, medical,
or emotional abuse, and serious neglect where criminal investigations are warranted, and
sexual abuse. Law enforcement is notied of reports classied as investigations to allow for
co-investigation.
Family assessment responses (alternative responses) are screened-in reports of suspected
maltreatment. Family assessment reports include mild, moderate, or rst-time noncriminal
Child Maltreatment 2022
Appendix d: State Commentary 213

reports of physical abuse or neglect, mild or moderate reports of emotional maltreatment, and
educational neglect reports. These include reports where a law enforcement co-investigation
does not appear necessary to ensure the safety of the child. When a report is classied as a
family assessment, it is assigned to staff who conducts a thorough family assessment. The
main purpose of a family assessment is to determine the child’s safety and the family’s needs
for services. Taking a non-punitive assessment approach has created an environment in
which the family and the children’s service worker are able to develop a rapport and build on
existing family strengths to create a mutually agreed-upon plan. Law enforcement is gener-
ally not involved in family assessments unless a specic need exists.
Reports
The response time indicated is based on the time from the login of the call to the time of the
rst actual face-to-face contact with the victim for all report and response types, recorded
in hours. State policy enables, in addition to CPS staff, multidisciplinary team members
to make the initial face-to-face contact for safety assurance. The multidisciplinary teams
include law enforcement, local public school liaisons, juvenile ofcers, juvenile court of-
cials, or other service agencies. Child protective services (CPS) staff will contact the multi-
disciplinary person to help with assuring safety. Once safety is assured, the multidisciplinary
person will contact the assigned worker. The worker is then required to follow-up with the
family and sees all household children within 72 hours. Data provided for 2021 does not
include initial contact with multidisciplinary team members.
Missouri uses structured decision-making protocols to classify hotline calls and to determine
whether a call should be screened out or assigned. If a call is screened out, all concerns are
documented by the division and the caller is provided with referral contact information when
available.
During Covid, Missouri had an increase in referrals that were called in for educational
neglect that were linked to distance learning issues and did not meet the guidelines for
educational neglect. Due to the volume of calls, these reports were accepted as preventative
service referrals. As of May 2021, Missouri no longer accepted these referrals if they did not
meet the guidelines for educational neglect. This led to a decrease in the overall number of
referrals in FFY 2022 compared with FFY 2021.
Children
The state counts a child as a victim of abuse or neglect based on a preponderance of evidence
standard or court-adjudicated determination. Children who received an alternative response
are not considered to be victims of abuse or neglect as dened by state statute. Therefore, the
rate of prior victimization, for example, is not comparable to states that dene victimization
in a different manner, and may result in a lower rate of victimization than such states. For
example, the state measures its rate of prior victimization by calculating the total number of
2021 substantiated records, and dividing it by the total number of prior substantiated records,
not including unsubstantiated or alternate response records.
Missouri implemented multiple protocols to meet our investigation and assessment guide-
lines on ensuring safety and child contact. Temporary policies addressed both child and
worker safety, proper use and availability of PPE, virtual, curbside and in-person visits. In
Missouri (continued)
Child Maltreatment 2022
Appendix d: State Commentary 214

many situations, we did continue to investigate reports in-person. Safety of children contin-
ued to be a primary concern and when a child needed to be removed from the home, practice
was not impacted. Changes were made to our states’ calculation for our time from the start of
an investigation to nal determination for the Agency File by mirroring the same logic used
in the Child File.
Missouri tracks cases with sex trafcking victims as a result of the 2017 Preventing Sex
Trafcking and Strengthening Families Act. With the 2019 expansion of the denition
of care, custody, and control in Missouri Children’s Division policy to include those who
take control of a child by deception, force, or coercion, we have been able to identify any
perpetrator of sex trafcking as a caregiver and include them in NCANDS data. Missouri’s
concern with barriers is the current lack of an evidence-based model specic to assessing,
identifying, and responding to trafcking as it relates to working with children through the
child welfare system. CD has worked with other states to develop a comprehensive assess-
ment tool for child victims of both labor and sex trafcking. This new tool was incorporated
into CD policy and supported by Advanced Human Trafcking training.
Missouri collects data on Plans of Safe Care in the instance of a Newborn Crisis Assessment
Referral. During FFY 2022, there were 273 children who had a Plan of Safe Care developed.
During a prior review of reports, it was that noticed that staff were not checking the box as
they should. Our agency has been telling staff during their training to check the box in our
system if a plan of safe care is put in place. This is being addressed again on our agency’s
monthly CA/N call.
Newborn Crisis Assessments in Missouri are not considered reports of abuse or neglect and
there are no plans, in Missouri, to change the way Newborn Crisis Referrals are categorized.
They will continue to be considered referrals and not reports of abuse/neglect.
Fatalities
Missouri statute requires medical examiners or coroners to report all child deaths to the
Children’s Division Central Hotline Unit. Deaths due to alleged abuse or those which are
suspicious in nature are accepted for investigation, and deaths which are nonsuspicious,
accidental, natural, or congenital are screened out as referrals. Through Missouri statute,
legislation created the Missouri State Technical Assistance Team (STAT) to review and assist
law enforcement and the Children’s Division in instances of severe abuse of children.
While there is not currently an interface between the state’s electronic case management
system and the Bureau of Vital Records statistical database, STAT has collaborative pro-
cesses with the Bureau of Vital Records to routinely compare fatality information. STAT also
has the capacity to make additional reports of deaths to the hotline to ensure all deaths are
captured in Missouri’s electronic case management system (FACES). The standard of proof
for determining if child abuse and neglect was a contributing factor in the child’s death is
based on the preponderance of evidence.
Because Missouri’s hotline (CPS) agency is the central recipient for fatality reporting and
because of the state statute requiring coroners and medical examiners to report all fatalities,
Missouri could appear to have a higher number of fatalities when compared to other states
Missouri (continued)
Child Maltreatment 2022
Appendix d: State Commentary 215

where the CPS agency is not the central recipient of fatality data. Other states may have to
obtain fatality information from other agencies and, thus, have more difculty with fully
reporting fatalities.
In FFY 2020, Missouri adjusted coding on our mapping document to more accurately
provide child fatality information in the Child File rather than the Agency File, based on a
mapping issue found in FFY 2019 data.
Perpetrators
The state retains individual ndings for perpetrators associated with individual children. For
NCANDS, the value of the report disposition is equal to the most severe determination of
any perpetrator associated with the report.
In the 2019 Missouri legislative session, a statutory addition to the denition of those respon-
sible for the care, custody and control of a child was enacted. Current statutory denition of
care, custody and control of a child includes:
■ The parents or legal guardians of a child;
■ Other members of the child’s household;
■ Those exercising supervision over a child for any part of a twenty-four-hour day;
■ Any adult person who has access to the child based on relationship to the parents of the
child or members of the child’s household or the family;
■ Any person who takes control of the child by deception, force, or coercion; or
■ School personnel, contractors, and volunteers, if the relationship with the child was estab-
lished through the school or through school-related activities, even if the alleged abuse or
neglect occurred outside of school hours or off school grounds.
The last bullet was added to the denition to provide the Children’s Division an enhanced
ability to investigate child abuse/neglect when the alleged perpetrator has a relationship with
the victim child through school.
Missouri made a policy change to the category of “other” that changed the wording “par-
amour” to “partner” which added additional coding that fell to the “other” category. In
FFY 2020, Missouri updated coding on our mapping document to capture “partner” which
resulted in an elevated percent changed from the “other” category. The “other” category also
includes reports where the perpetrator is coded as “self” for the victim. These are instances
usually involving older victim children that are also perpetrators themselves, to younger
children on the same report, which puts them in the “other” category.
Services
Children younger than 3 years are required to be referred to the First Steps program if the child
has been determined abused or neglected by a preponderance of evidence in a child abuse and
neglect investigation. Referrals are made electronically on the First Steps website or by submit-
ting a paper referral via mail, fax, or email. First Steps reviews the paper or electronic referral
and noties the primary contact to initiate the intake and evaluation process.
Missouri (continued)
Child Maltreatment 2022
Appendix d: State Commentary 216


Nebraska
Contact Jake Malone Phone 40 2– 471– 9112
Title IT Business Systems Analyst Supervisor Email
Address Nebraska Department of Health and Human Services
Nebraska State Ofce Building, 3rd Floor
301 Centennial Mall South
Lincoln, NE 68509
General
Nebraska continued to utilize the Structured Decision Making (SDM®) model, a set of
research-based decision-support assessments, to assess reports of child safety and risk. The
utilization of SDM® provides consistency in the decision-making of protective services staff
from the point of accepting reports of abuse and neglect through the assessment of child safety
and risk levels.
Nebraska has a two-tiered system of responding to accepted reports of abuse and neglect.
Reports are assigned to a Traditional assessment or an Alternative Response. Alternative
Response (AR) is an approach to keep children safe in a family-friendly way by doing things
such as making appointments to see the family, asking the parents or caregivers for permission
to talk to their children and other collaterals, not entering abuse or neglect ndings, and offer-
ing concrete supports, among other things. AR started as a pilot in ve counties in 2014 and has
since expanded statewide as of October 1, 2018. Data for traditional and AR cases are reported
to NCANDS.
Successful child welfare practice is predicated on engaging the families with whom we come
into contact. To enhance our engagement skills, the Division of Children and Family Services
introduced Safety Organized Practice (SOP) to our staff beginning in April 2019. SOP is an
approach to child welfare casework designed to help all key stakeholders—the family and
professionals—involved with a child keep a clear focus on assessing and enhancing safety at all
points in the case process. By employing solution-focused interviewing, proven strategies for
meaningful child and youth participation, and a common language for concepts like “safety,”
“danger,” and risk,” SOP compliments SDM® to create a rigorous child welfare practice model
that is neither too naïve nor negative in its view of families. The tools utilized in SOP are
proven to enhance the development of good working relationships and create detailed practi-
cal, achievable safety plans. In the last four years, CFS has completed the roll-out of all 12
modules of SOP training statewide and is developing ongoing refresher training for staff across
Nebraska.
Reports
All reports of child abuse and neglect are received at the toll-free, 24/7, centralized Nebraska
Child and Adult Abuse and Neglect Intake Hotline (Hotline). The Hotline workers and
supervisors utilize SDM® to determine whether a report meets criteria for intervention and
the subsequent response time for accepted reports. Accepted reports are assigned to a worker
to conduct an initial assessment, which includes an SDM® Safety Assessment and SDM®
Safety Plan (if applicable) and an SDM® Risk or Prevention Assessment. Each SDM®
Assessment provides decision-making support to the worker to determine whether a case
should remain open for ongoing services.
Child Maltreatment 2022
Appendix d: State Commentary 218

Nebraska experienced a decrease in screened-in reports to the Hotline in FFY 2022. Despite
this decrease, Nebraska experienced an approximately 25 percent increase in screened-out
reports during FFY 2022 compared to FFY 2021 after several years of decreases during the
pandemic. The number of screened-out reports dropped signicantly during the pandemic
and has not reached the pre-pandemic levels. To ensure the safety of Nebraska’s most vulner-
able population, in June 2019, a policy was enacted whereby all reports made by medical
professionals that involve an identied child or child victim age ve and under are accepted
for assessment. That same month, Central Ofce program policy staff began performing
second-level reviews of all reports screened out at the Hotline. As of November 2021, these
reviews are conducted by Hotline supervisors. These reviews ensure the correct screening
decisions concerning reports not accepted for assessment are made.
Since the onset of the pandemic and throughout the ensuing three years, child abuse and
neglect referrals have been affected within Nebraska. Overall, the Hotline experienced
decreased call volume. Specically, there were fewer calls from educational professionals due
to school closings. However, there has been increased reporting from local law enforcement
agencies. Notably, referrals to the Hotline during this time have involved families experienc-
ing high-stress levels and involving more serious physical abuse of young children. Nebraska
has seen increased severity of verbal and physical family violence involving both weapons
and serious threats of harm. There has also been an increase in the number and complexity
of sex trafcking reports and exposure to sexualized content due to children having more
access to the internet.
The Nebraska Department of Health and Human Services (DHHS) did not change any
Hotline policies or procedures related to screening due to the pandemic. Nebraska also did
not experience staff reduction due to the pandemic. Specically, the Hotline did not have any
reductions due to the pandemic. However, with natural attrition, positions were utilized to
help other areas of child welfare to ensure coverage to meet child and family contact dead-
lines and complete safety assessments promptly and accurately.
Children
In FFY 2022, Nebraska saw a decrease in unique child victims. The continued expansion of
the use of Alternative Response, partly accounts for this decrease. Also, the policy enacted
whereby all reports made by medical professionals that involve an identied child or child
victim age ve and under are accepted for assessment affected this as many of those reports
are also screened as Alternative Response. Further, all Agency Substantiated ndings are
reviewed and entered by supervisors who have administrative oversight of this process. The
supervisor considering a nding of Agency Substantiated and the entry of the alleged perpe-
trator’s name on the Central Registry must nd sufcient evidence to support that the subject
of the report, the alleged perpetrator, committed child abuse or neglect as outlined in state
statute and determine that the evidence meets statutory requirements.
Nebraska did not change any policies related to investigating allegations of child abuse and
neglect or conducting assessments with families during the COVID-19 pandemic, except that
the time frame identied for CFS Specialists to complete assessments was extended from 30
to 45 days, and an Administrative Exception could be granted for an additional 15 days.
Nebraska (continued)
Child Maltreatment 2022
Appendix d: State Commentary 219

CFS experienced an increase in the average response time. During FFY 2022, Nebraska ended
privatization in the Eastern Service area of the state, which is the largest population area. This
change affected stafng and the ability to respond timely to reports and complete assessments.
Nebraska also changed policy during FFY 2022 to remove the lowest response priority time-
frames. Previously, Nebraska had three priority response timeframes, 24 hours, ve days, and
ten days. Now Nebraska prioritizes reports as needing a 24-hour or ve-day response.
For FFY 2022, Nebraska reported the sex trafcking maltreatment type for the entire year. As
of August 2019, Nebraska accepts all reports of trafcking without regard to the subject (the
alleged perpetrator) of the report for assessment of child safety. Findings allow for differentiation
between labor and sex trafcking. However, the nding is not an accurate indication of who is a
trafcking victim since often the identity of the subject is not known, and CFS cannot substanti-
ate an unknown perpetrator or list them on the Central Registry. Most victims of sex trafcking
engage in “survival sex,” and thus far, there is no mechanism for tracking these cases.
Beginning on April 1. 2021, CFS entered into a contract with HTI Labs to include the
Providing Avenues for Victim Empowerment (PAVE) tool in the intake and assessment
processes. PAVE is a screening, assessment, and referral process that connects trafcking
victims to services. PAVE provides a “no wrong door” entry to Children and Family Services
for victims of labor and sex trafcking. Any provider participating in PAVE completes the
PAVE screening and forwards it to the Abuse and Neglect Hotline. The Hotline receives the
report and refers it to eld staff for investigation and assessment. The level of trafcking risk
is assessed, and appropriate next steps and services that law enforcement and CFS Specialists
can implement for victims are recommended. This will result in increased reporting, ensur-
ing that those at risk of being trafcked, have been trafcked, or are survivors of trafcking
are connected with the appropriate services.
All reports from medical professionals involving children 0-5 years of age are accepted at the
Hotline. Through the Comprehensive Addiction and Recovery Act (CARA), Nebraska has set
up a notication process for birthing hospitals. If the hospital does not feel there are concerns
of abuse or neglect, but an infant was born affected by substance use, a notication is made
to DHHS. While we continue to work with our hospitals on implementing CARA and the
difference between reporting and sending a notice, some infants are missed due to noti-
cations not being sent to DHHS. In November 2020, an updated letter explaining the two pro-
cesses was sent out to all Nebraska hospitals. The Nebraska Perinatal Quality Improvement
Collaborative held a video conference in January 2021 for all hospitals to receive additional
training and guidance on Nebraska’s CARA Implementation. This video conference was
recorded for those unable to join live.
Nebraska continues to work with external partners, including hospitals, to ensure they pro-
vide CFS staff with the necessary information to complete Plans of Safe Care. Nebraska was
chosen to receive In-Depth Technical Assistance, a two-year project through the National
Center for Substance Abuse and Child Welfare and Children and Family Futures. While the
main focus is on developing Plans of Safe Care prenatally, the data and work with external
stakeholders will allow Nebraska to grow and improve practice, ensuring all infants born
affected by substance use have a Plan of Safe Care documented.
Nebraska (continued)
Child Maltreatment 2022
Appendix d: State Commentary 220

Nebraska continues to increase identication and reporting on infants with prenatal
substance exposure, and CFS continues to discuss improvement strategies with the admin-
istration. Currently, only data based on children’s characteristics are included, but CFS is
working on incorporating caregiver characteristics related to substance use. In the past year,
a Standard Work Instruction was updated for all staff on what to do when an infant affected
by prenatal substance use is identied. Recently, data was made available to all service areas
to monitor the completion of Plans of Safe Care.
Fatalities
Nebraska reports child fatalities in both the Child File and the Agency File. Nebraska
reported three child fatalities resulting from maltreatment in FFY 2022. All child fatalities
are under investigation as of the date of this writing. Nebraska continues to work with the
state’s Child and Maternal Death Review Team (CMDRT) to identify child fatalities resulting
from maltreatment but not included in the child welfare system. When a child fatality is not
included in the Child File, the state determines if the child fatality should be included in the
Agency File. The ofcial report from CMDRT with nal results is usually made available
two to three years after submitting the NCANDS Child and Agency les. Nebraska will
resubmit the Agency File for previous years when there is a difference in the count than was
initially reported due to the CMDRT nal report. No policies were changed concerning child
fatality reviews.
Perpetrators
Nebraska collects information on the perpetrators and enters the data into the child welfare
information system. Information includes perpetrator demographics and the relationship
of the perpetrator to the child. Nebraska state statute prohibits a perpetrator under 12 years
of age from being listed as a substantiated perpetrator. The maltreatment will be listed, but
there is no nding entered indicating if the maltreatment was substantiated or unfounded.
In FFY 2022, Nebraska saw a decrease in unique perpetrators compared to FFY 2021. This
decrease correlated with the decline in victims and is likely due to a combination of factors:
more reports are going to Alternative Response than previously; supervisors are reviewing
all recommended ndings; and the COVID-19 pandemic has affected the number of reports
received at the Hotline and assessments performed.
Nebraska reports noncaregiver perpetrators of sex trafcking to NCANDS. Nebraska
Revised Statutes 28-710 and 28-713 require DHHS to conduct in-person investigations of
trafcking regardless of the alleged perpetrator’s relationship to the alleged victim. This
legislation was effective in August 2019. Nebraska reports “Other” relationships for perpetra-
tors of sex trafcking, including non-relatives and other people who are not professional
caregivers.
Services
Nebraska refers children younger than three years old to the Early Development Network
(EDN) in a substantiated case or a case referred by the county attorney for prosecution.
Nebraska has automated its referral system to its Early Childhood Development Network and
automatically notify the network of these children.
Nebraska (continued)
Child Maltreatment 2022
Appendix d: State Commentary 221

Nebraska believes most of the services provided to families can be accomplished during the
assessment phase, between the report date and the nal disposition. When a case disposi-
tion is delayed due to awaiting a court disposition, services are provided to the family. Case
management, supervised visitation, family support services, and addiction services are only
a few of the services frequently utilized by families during the pendency of their court cases.
Some or all of the services may often be concluded before the disposition. In many cases,
these are the only services required to keep the child or victim safe. Services provided before
disposition are not included in the NCANDS Child File; only those services that extend
beyond the disposition are included.
Nebraska DHHS Division of Children and Family Services provides child welfare services to
the citizens of Nebraska. The statewide Hotline is centralized in Omaha but serves the entire
state. Initial Assessment (investigation) is conducted by State of Nebraska Child and Family
Services Specialists (CFS Specialists). Before FFY 2022, CFS Specialists conducted case
management in all but one service area. In the Eastern Service Area, the privatization of case
management ended during FFY 2022.
Nebraska (continued)
Child Maltreatment 2022
Appendix d: State Commentary 222

Nevada
Contact Alexia Benshoof Phone 775– 687–9013
Title Management Analyst IV Email
abenshoof@dcfs.nv.gov
Address NV Department of Health and Human Services
4126 Technology Way, 3rd Floor
Carson City, NV 89706
General
Nevada child welfare agencies use a single statewide child welfare information system known
as Unied Nevada Information Technology for Youth (UNITY). UNITY is governed by
federal Comprehensive Child Welfare Information System (CCWIS) regulations. Child welfare
agencies in Nevada follow the Safety Assessment and Family Evaluation (SAFE) model. The
SAFE model supports the transfer of learning and ongoing assessment of safety throughout the
life of the case. The model emphasizes the differences between identication of present and
impending danger, assessment of how decient caregiver protective capacities contribute to the
existence of safety threats and safety planning and management services, assessment of motiva-
tional readiness, and utilization of the Stages of Change theory as a way of understanding and
intervening with families. All child welfare agencies in Nevada have implemented this model,
which has changed the state’s way of assessing child abuse and neglect and has enhanced the
state’s ability to identify appropriate services to reduce safety issues in the children’s home of
origin. Additionally, this model has unied the state’s CPS processes and standards regarding
investigation of maltreatment.
Nevada has an alternative response program, called Differential Response (DR). Families
referred to the program are the subject of reports of child abuse and/or neglect which were
determined by the agency as likely to benet from voluntary early intervention through assess-
ment of their unique strengths, risks, and individual needs, rather than the more intrusive
approach of investigation. Each child welfare agency provides DR services differently through
their agency
Reports
In FFY 2022, there was an increase in reports of abuse or neglect completed or dispositioned in
the year as compared to the previous year. Nevada has established intake processes, governed
by the SAFE model, to determine if CPS referrals constitute reports of abuse or neglect.
Referrals that contain insufcient information about the family or maltreatment of the child and
no allegations of child abuse/ are screened-out. Referrals that do meet criteria are screened-in.
Based on various factors associated with the report, CPS supervisors decide what type of
response the report merits, assign the report to either Investigation or Differential Response,
and assign a response time according to policy.
The statewide intake policy was updated in April 2020 due to challenges of the COVID-19
pandemic. One adjustment made was that some response times to make face-to-face contact
with children were modied. Report response times are one of the following:
■ Priority 1: respond within 6 hours when the identied danger is urgent or of emergency
status, there is present danger, and safety factors are identied; this response type requires
a face-to-face contact by CPS (due to COVID, this was changed from 3 hours to 6 hours
for all jurisdictions; Rural Region child welfare was previously using 6 hours as response
time so it did not change for them).
Child Maltreatment 2022
Appendix d: State Commentary 223

■ Priority 2: respond within 24 hours with any maltreatment of impending danger and safety
factors identied including child fatality; this response type requires a face-to-face contact
by CPS or may involve collateral contact by telephone or case review (this response time
did not change due to COVID; it is the still the same as it was prior to the pandemic).
■ Priority 3: respond within 7 business days when maltreatment is indicated, but no safety
factors are identied; this response type requires a face-to-face contact by CPS or may
involve collateral contact by telephone or case review. In situations where the initial
contact is by telephone, the agency must make a face-to-face contact with the alleged child
victim within 24 hours following the telephone contact (this response time changed due
to COVID; previously contact had to be made within 72 hours). The DR program has a
required report response time of Priority 3: respond within 7 business days (this was not
affected by the pandemic).
During FFY 2022, policies governing response times and pandemic modications for CPS
were still in place, although program oversight staff indicated workers are returning to pre-
pandemic practices for investigations and assessments as much as possible.
Over the last year, Nevada continued various Continuous Quality Improvement (CQI) initia-
tives related to Nevada’s last federal Child and Family Services Review (CFSR) and subsequent
Program Improvement Plan (PIP). One ongoing CQI initiative is related to improving the
timeliness of initial contact with all children on screened-in reports. As part of the PIP, over
the last few years, child welfare staff improved processes to reach out to families and make
child contact promptly and improved processes for timely documentation of contact in the child
welfare information system. A monitoring and oversight report was developed as a tool for eld
supervisors as well as CQI and QA units to track adherence to processes and policies in this
area, and training and technical assistance have been provided regularly to improve documen-
tation of initial child contact, which has improved the overall average response times for reports
included in our NCANDS data.
Nevada’s CPS reports received are back up to pre-pandemic levels. Additionally, the statewide
CPS Hotline for child maltreatment referrals did not go through any changes to the hours of
operation or stafng levels during FFY 2022. The Rural Region opened a new centralized
intake unit during FFY 2021 and were still only 60% staffed through FFY 2022, but plan to
become fully staffed in January 2023.
Children
In FFY 2022, there was an increase in the number of children reported as possible victims as
compared to the previous year. Further, the number of conrmed unique victims increased
compared to the previous year. Nevada child welfare policy requires that all children in a
household are assessed for safety and well-being if any child in the household has a maltreat-
ment allegation.
Regarding alcohol and drug abuse risk factors for both children and caregivers, some reporting
limitations exist in our data. For example, there are several places in the statewide child welfare
information system where data related to NCANDS alcohol or drug abuse risk factors for
children or caregivers can be captured. Depending on how and where data is entered, the value
for both the alcohol abuse and drug abuse risk factors for a child or caregiver may be reported
Nevada (continued)
Child Maltreatment 2022
Appendix d: State Commentary 224

as ‘1-yes’ or only one risk factor may be set to ‘1-yes.’ There is overlap where the risk factor for
both alcohol and drug abuse can be set to ‘1-yes’ when there is documented substance abuse,
but it is not clear whether it due to alcohol or drugs.
Over the last year, the child welfare information system was updated to be able to collect
whether a substance-exposed infant has a plan of safe care. The changes to the information
system were deployed in late May 2022, which allowed certain CARA-related data collection
to start at the end of May 2022. For many substance-exposed infants in our NCANDS Child
File, both child risk factors related to alcohol and drug abuse are set to ‘1-yes’ based on the way
substance-exposed infants are often documented in Nevada’s child welfare information system.
In the past year, functionality was added to the state’s child welfare information system for
collecting and documenting Commercial Sexual Exploitation of Children (CSEC). However,
this documentation does not always involve a screened-in CPS report with allegations of
maltreatment, as perpetrators may often be noncaregivers or may be unknown. When CSEC
is identied for a child and no maltreatment is alleged against the child’s known caregiver,
then Nevada’s coordinated model response protocol may be initiated. Staff will input CSEC
information into the child welfare information system, but not necessarily as a report requiring
a traditional CPS Investigation; in those instances, because there is no maltreatment allegation
or investigation initiated, these youth and the CSEC data cannot be reported in the NCANDS
Child File. Regarding instances where CSEC-related maltreatment is alleged against the child’s
caregiver, then a report and investigation will be initiated.
Fatalities
Fatalities identied in the child welfare information system as maltreatment deaths are reported
in the Child File. Deaths not included in the Child File, for which substantiated maltreatment
was a contributing factor, are included in the Agency File as an unduplicated count. Reported
fatalities can include deaths that occurred in prior periods, for which the determination was
completed in the next reporting period. The total number of NCANDS reported fatalities has
decreased since the last reporting period.
Nevada uses a variety of sources when compiling reports and data about child fatalities result-
ing from maltreatment. Any instance of a child suffering a fatality or near fatality, who previ-
ously had contact with, or was in the custody of, a child welfare agency, is subject to an internal
case review. Data are extracted from the case review reports and used for local, state, and
federal reporting as well as to support prevention messaging. Additionally, Nevada has both
state and local child death review (CDR) teams which review deaths of children. The purpose
of the Nevada CDR process is public awareness and prevention, enabling many agencies and
jurisdictions to work together to gain a better understanding of child deaths. The regional and
statewide CDR teams did not undergo any policy changes to the child fatality review process
due to the pandemic.
Perpetrators
Nevada does not report caregiver perpetrators of sex trafcking to NCANDS.
Nevada (continued)
Child Maltreatment 2022
Appendix d: State Commentary 225

Services
In FFY 2022, Nevada has returned to pre-pandemic working practices whenever possible.
Program staff indicate there are, however, some circumstances that continue to require some
appointments to be delivered via telehealth methods.
Many of the services provided to children and families served by CPS agencies are handled
through outside providers. Information on services received by families is reported through
various programs. Each child welfare jurisdiction manages its service array differently.
Services provided in conjunction with the new safety model are documented in the UNITY
system, but these data are not always readily reportable as they may documented as text in
lengthy case notes instead of in easily query-able data elds. The state is continuing to investi-
gate how to improve reporting of services-related data.
Nevada follows its statewide policy (#0502 CAPTA-IDEA Part C), which states: “Child welfare
agencies will refer children under the age of three (3) who are involved in a substantiated case
of child abuse or neglect, or who have a positive drug screen at birth, to Early Intervention
Services within two (2) working days of identifying the child(ren) pursuant to CAPTA Section
106 (b)(2)(A)(xxi) and IDEA Part C of 2004.” The policy further denes “involved” to include
children that are identied as: having been abused or neglected; having a positive drug screen
at birth; or found in need of services.
Nevada (continued)
Child Maltreatment 2022
Appendix d: State Commentary 226

New Hampshire
Contact Daniel Paton Phone 603–271–4714
Title Data Analyst Email
Address Division for Children, Youth and Families
Department of Health and Human Services
97 Pleasant Street
Concord, NH 03301
General
New Hampshire was able to update the NCANDS extract code this year to provide more
accuracy in the following areas:
■ “Added Allegations,” additional information that came in as subsequent referrals during
an investigation and were rolled up into the original referral. This accounted for over 500
additional records and nearly 2,600 additional maltreatment allegations and dispositions.
■ New services in our service array for home-based therapeutic services.
■ A new voluntary Case Management service provided following unfounded investigations.
■ Some CARA elds are being reported for the rst time.
New Hampshire’s child protection system does not include Differential Response. The state
uses a tiered system of required response time, ranging from 24 to 72 hours, depending
on level of risk at the time of the referral, as determined by a Structured Decision Making
(SDM) tool.
Reports
There was no signicant change in the number of reports received during the year, nor the
number of screen-outs. Stafng rates for both intake and investigations also remained the same,
although the State experienced about a 20 percent turnover in stafng for CPS functions. The
State contracts with a vendor to receive and document reports after hours and on weekends and
holidays.
The screening process in New Hampshire relies on a structured decisionmaking tool to deter-
mine whether a report rises to a level of risk requiring an investigation. Screened-out reports
are retained in the system to provide context for future reports.
Response time for screened-in reports decreased for a fourth year in a row as the agency
continues to focus on improving practice and compliance with recommended timeframes. This
improvement is supported by daily conferences between workers and supervisors to determine
the workers’ priorities for the day, including meeting required response times for assessments.
Children
There was no signicant change in the number of children or victims this year. For sex
trafcking reports, New Hampshire began screening in all reports of sex trafcking, regard-
less of the relationship to the perpetrator(s), in September 2021. Prior to that date, only the
reports where the perpetrator was a member of the household were screened in. As a result of
this policy, and a concerted educational campaign to ensure that all suspected sex trafcking
cases are reported to DCYF, regardless of who the perpetrator may be, and to ensure that
police departments understand the denitions of sex trafcking that are reportable offenses,
the number of sex trafcking reports and potential victims rose by approximately 140
percent.
Child Maltreatment 2022
Appendix d: State Commentary 227

This is the rst year that Plans of Safe Care and Referrals to Appropriate Services for CARA
are included in the NCANDS Child File. However, because the elds that collect this infor-
mation in the system are not mandatory we did not meet the recommended goal of 95 percent
reporting. We expect these numbers to improve in the future, particularly after the state
implements a new CCWIS, currently in design.
Fatalities
New Hampshire documents fatalities that are suspected of being the result of abuse or
neglect in the state SACWIS. Therefore, all immediately known fatalities are reported in
the Child File. However, in a situation where a child is rst reported missing, but then found
deceased months or years later, the fatality may not have been documented in the SACWIS
and will be included in the Agency File.
The state’s Child Fatality Review Committee (CFRC) reviews child deaths from many differ-
ent causes, including abuse/neglect. However, the committee is not a source of reporting to
intake or for the NCANDS submission.
In addition to the CFRC, the NH Division for Children Youth and Families conducts fatality
reviews internally, employing a safety science model that focuses on systems and how those
systems impacted decision making. The assigned worker and supervisor for the case affected
by a fatality attends these reviews.
The NH Ofce of Child Advocate also conducts their own fatality reviews, using a systems
learning model. The assigned worker and supervisor do not attend those reviews, but a team
from the child protection agency does participate.
Perpetrators
With the exception of sex trafcking, New Hampshire screens in only those reports where
the alleged perpetrator is a member of the child’s household, having access to the child. The
perpetrator may or may not be a caregiver, but is always a member of the household. For sex
trafcking, New Hampshire began screening in all reports of sex trafcking, regardless of
the relationship to the perpetrator(s), in September 2021. Prior to that date, only the reports
where the perpetrator was a member of the household were screened in.
New Hampshire generally does not name minors as perpetrators of neglect or physical abuse,
except for juvenile parents who have abused or neglected their own children. Other minors
may be named as perpetrators of physical abuse, however it is more likely that the report
will be approached as parental neglect (lack of supervision) when a child is reported to be
physically abused by another child in the home. By policy, no child under the age of 13 may
be named as a perpetrator of sexual abuse. There are no other policies governing the age at
which a minor may be named as a perpetrator.
All perpetrator relationships are mapped to one of the NCANDS values, and we do not use
“other” for any perpetrator relationships.
New Hampshire (continued)
Child Maltreatment 2022
Appendix d: State Commentary 228

Services
In February 2021, DCYF began providing case management services, through an indepen-
dent service provider, for some families following an assessment in which concerns did not
warrant a nding of abuse or neglect, but where the family was found to be at higher risk.
This is the rst year that we have reported on this service.
“Other” services in Element 85 includes “ISO In-Home,” an Individual Service Option that
provides comprehensive services for children/youth with signicant challenges, which may
be medical, physical, behavioral, or psychological. The service therefore ts into several
different service categories, but not precisely into any one category.
New Hampshire is only able to report services that were paid for or authorized directly by the
child protection agency. Services that were paid for by Medicaid or the family’s own health
insurance are not reported for:
■ Counseling Services
■ Health-Related and Home Health Services
■ Substance Abuse Services
New Hampshire does not provide or collect data on the following services, as dened by
NCANDS:
■ Employment Services
■ Family Planning Services
■ Home Based Services
■ Information and Referral Services
■ Housing Services
■ Legal Services
New Hampshire (continued)
Child Maltreatment 2022
Appendix d: State Commentary 229

New Jersey
Contact Nicole Ruiz Phone 609–888–7336
Title Program Specialist
Ofce of Research, Evaluation and Reporting
Email
Address New Jersey Department of Children and Families
50 East State Street
Trenton, NJ 08625
General
Each NCANDS Child File data element is reported from New Jersey’s system, called NJ
SPIRIT. The state is continuously making enhancements toward improving the quality of
NCANDS data. New jersey has declared that NJ SPIRIT will be its comprehensive child
welfare information system (CCWIS) and plans to achieve compliance.
New Jersey’s Department of Children and Families’ (DCF) Division of Child Protection and
Permanency (CP&P) investigates all reports of child abuse and neglect. New jersey does
not use a differential response protocol; all allegations of child abuse and neglect meeting
statutory criteria for investigation are screened-in for response. In New Jersey, the category
of neglect includes allegations of medical neglect. NJ SPIRIT allows the linking of multiple
CPS reports to a single investigation. The state system also allows for documenting the date
and time of the initial face-to-face contact that began the investigation.
Reports
In FFY 2022, the number of unique reports increased compared to FFY 2021, however,
this number is consistent with reports received prior to COVID-19. Phone calls to our State
Central Registry (SCR) decreased with the onset of COVID-19. We attribute the number of
reports increasing in FFY 2022 to the leveling of our call volume.
Our screening process for reports only takes place at our SCR. As a result of COVID-19,
there was a change in stafng protocols in which resulted in a decrease in the number of SCR
staff. A new 40-hour work week is being implemented to assist with call volume and these
positions are expected to be lled by the end of FFY 2023.
For a CPS report to be accepted, four criteria must be met:
■ The alleged child victim is a born child, under 18 years of age.
■ The alleged perpetrator(s) is the child’s parent, guardian, or other person in a caregiving
role, who has custody or control of the child.
■ The child victim(s) was harmed or placed at substantial risk of harm; meeting criteria
specied in the allegation based system.
■ There is a specic incident or set of circumstances that suggest the harm or substantial
risk of harm was caused by the child’s parent, guardian or other person having custody or
control of the child.
Children
New Jersey investigates allegations of commercial sexual exploitation for alleged victims
under the age of 18; in addition, New Jersey only investigates child abuse and neglect allega-
tions of sex trafcking when the alleged perpetrator is in a caregiving role. For FFY 2022,
there were additional children subject to human trafcking by a non-caregiver who received
services from DCF; however, they are not included in the CPS report count.
Child Maltreatment 2022
Appendix d: State Commentary 230

Children with allegations of maltreatment are designated as alleged victims in the CPS report
and are included in the NCANDS Child File. NJ SPIRIT allows for reporting more than one
race for a child. Race, Hispanic/Latino origin, and ethnicity are each collected in separate
elds. Despite the number of CPS referrals increasing from FFY 2021 to FFY 2022, the
number of child victims continues to decrease. The rate in which NJ substantiated reports
also decreased from FFY 2021 to FFY 2022.
In 2017, in response to the comprehensive addiction and recovery act of 2016 (CARA), New
Jersey amended its regulations and further modied the allegation-based system to capture
allegations of substance affected newborns. For FFY 2022, New Jersey identied more than
two thousand substance exposed newborns of which, 1,909 (94 percent) had a plan of safe
care and 1,909 (94 percent) were referred to appropriate services. We anticipate reporting the
number of plans of safe care created and the number referred to appropriate services in the
FFY 2023 NCANDS Child File.
Fatalities
In FFY 2022, the number of child fatalities increased compared to FFY 2021, however, New
Jersey has maintained a stable annual child fatality rate for the last ten years. Fluctuations in
the number of fatalities from year to year are likely due to random case-level variation and
are monitored closely. Child fatalities are reported to New Jersey DCF by many different
sources including law enforcement agencies, medical personnel, family members, schools,
ofces of medical examiners and, occasionally child death review teams. The CP&P assistant
commissioner ultimately determines if the child fatality was the result of child maltreatment.
The ofce of quality manages a critical incident review process that uses safety science
approaches, including human factors debrieng. The state NCANDS liaison consults with
the ofce of quality and CP&P to ensure that all child maltreatment fatalities are reported in
the state NCANDS les.
NJ SPIRIT is the primary source of reporting child fatalities in the NCANDS Child le.
Specically, child maltreatment deaths are reported in the NCANDS Child File in the eld
maltreatment death. The data is collected and recorded by investigators and the person man-
agement screens are updated in NJ SPIRIT. Other child maltreatment fatalities not reported
in the Child File due to data anomalies, but which are designated child maltreatment fatalities
by the Ofce of Quality under the Child Abuse Prevention and Treatment Act (CAPTA), are
reported in the NCANDS Agency File under child maltreatment fatalities not reported in the
Child File. New Jersey only investigates child deaths if there is a reported allegation of abuse
or neglect.
Perpetrators
In New Jersey, perpetrators are dened as persons responsible for a child’s welfare who have
engaged in the abuse or neglect of that child. Minors shall be considered caregivers to their
own children and may be considered caregivers to other children if caring for that child at the
time of an alleged act of abuse or neglect and of sufcient age and maturity to reasonably be
expected to provide such care. New Jersey does accept perpetrator relationship types that are
categorized as “other”, including but not limited to: child in foster/adoptive home, child in
other licensed care, and other. For sex trafcking, New Jersey only investigates child abuse
and neglect allegations in which the alleged perpetrator is in a caregiving role.
New Jersey (continued)
Child Maltreatment 2022
Appendix d: State Commentary 231

Services
New jersey aims to preserve children in their own home for support services. For more than
10 years, New Jersey continues to observe a decline in the volume of children separated
from their family as a child welfare intervention. Data regarding services to children with
behavioral health and substance use disorder diagnoses, as well as the volume of children
separated from their family as a child welfare intervention is available on the NJ child
welfare data hub at (www.njchilddata.rutgers.edu).
New jersey contracts for all direct services except for case management services. NJ SPIRIT
reports those services specically designated as family preservation services, family support
services, and foster care services as postinvestigation services in the Child File.
New Jersey (continued)
Child Maltreatment 2022
Appendix d: State Commentary 232

New Mexico
Contact Doreen Chavez Phone 505–412–9868
Title SACWIS/AFCARS/NCANDS/FACTS Program
Manager
Ofce of Performance and Accountability
Email
doreen.chavez@state.nm.us
Address Children, Youth & Families Department
1120 Paseo de Peralta
Santa Fe, NM 87501
General
There have been no recent changes in the state’s policies, programs, or procedures that would
affect New Mexico’s FFY 2022 NCANDS submission.
Currently, New Mexico does not have more than one type of response for screened-in
reports. All screened-in reports are investigated. Screened-out reports are cross-reported to
local law enforcement. A differential response pilot program was implemented in a limited
scope during FFY 2020 (to support families with allegations of educational neglect during
widespread remote schooling). Referral criteria expanded, and the program is now operating
as envisioned to support families with a wider variety of risk factors and needs. The program
is still only operational in four counties but will be rolled out to more counties in FFY 2023
and FFY 2024.
Reports
The number of screened-in referrals in FFY 2022 increased from New Mexico’s FFY 2021
NCANDS submission. This slight increase may be attributed to FFY 2022 being the year that
children were back to in-person learning and school personnel comprise a signicant propor-
tion of our reporting sources.
The agency has not made any signicant changes to its call center processes and procedures,
other than normal staff turnover and training, as well as concerted efforts to reduce call
center wait times.
The New Mexico denition for the investigation start date (“initiation”) is dened as the
caseworker making face-to-face contact with each alleged victim identied in the report,
rather than the individual child referenced in the NCANDS Child File. New Mexico also
measures initiation time frames from the point at which the report is accepted by Statewide
Central Intake, rather than the point at which the report is received or assigned to a worker in
the county where the family resides.
New Mexico has modied the state’s data collection system to capture incident information.
New Mexico updated the data collection to coincide with the 2022 reporting period. The
2022 submission should have an accurate incident date for the entire reporting year.
Children
The total number of unique children for FFY 2022 increased and the number of unique child
victims in FFY 2022 decreased from New Mexico’s FFY 2021 NCANDS submission.
New Mexico investigation procedures do include face-to-face assessment of all children
living in the household, regardless of whether they are identied as an alleged victim in the
initial report.
Child Maltreatment 2022
Appendix d: State Commentary 233

The state does not have the capacity to report sex trafcking as an allegation type currently.
As New Mexico transitions to a CCWIS, this change will be fully implemented, and report-
ing will likely begin once resources to map the changes become available.
New Mexico’s Department of Health receives the plans of care through the portal, although
there remain some training issues statewide with birthing hospitals on consistent use of the
portal.
Fatalities
New Mexico reported an increase by approximately 77 percent in FFY 2022 as compared to
FFY 2021. Percent differences in fatalities from year to year are highly susceptible to broad
uctuation due to the overall low numbers of applicable fatalities occurring in the population.
New Mexico’s overall child population is small compared to many other states. The total
number of fatalities from year to year is proportionately small, so even incrementally small
increases in the number of fatalities from one year to the next impacts the data but do not
necessarily indicate systemic changes in agency practice. Because these records are included
in the submission that corresponds with the investigation closure date, the length of time that
some of these cases must remain open to allow for thorough investigation can also create
year-over-year variation.
New Mexico identies applicable child fatalities for inclusion in the NCANDS Agency File
by comparing homicides in the child le with homicides identied by the state Ofce of the
Medical Investigator (OMI). Any child victims who do not already appear in the agency’s
NCANDS Child File are reviewed to determine the identity and relationship of the perpetra-
tor. Only children known to have died due to maltreatment by a parent or primary caregiver,
not already included in the child le, are then included in the NCANDS Agency File.
The agency does not investigate all fatalities. Only fatalities reported to the agency by law
enforcement, medical personnel, or other reporting source are investigated.
Perpetrators
The state only investigates and reports maltreatment allegations in which the alleged perpe-
trator is a parent or other caregiver such as a relative, other household member, stepparent,
guardian, foster parent, sibling, or any individual with responsibility for the care, supervi-
sion, and safety of a child. However, the agency does not report information on residential
staff perpetrators, as CPS does not have jurisdiction under state law to investigate allegations
of abuse and neglect in facilities. If such allegations are reported to Statewide Central Intake,
the following procedures are followed:
■ The report is screened out to CPS but cross-reported to the law enforcement agency that
has jurisdiction over the facility/incident.
■ The report is cross reported to the Licensing and Certication Authority, which as adminis-
trative oversight of residential facilities.
■ Upon request from law enforcement, CPS investigation staff may act in consultation in
conducting investigations of child abuse and neglect in schools and facilities and may assist
in the interview process.
New Mexico (continued)
Child Maltreatment 2022
Appendix d: State Commentary 234

Services
Postinvestigation services are reported for any child or family involved in a child welfare
agency report that has an identied service documented in the SACWIS as: 1) a service
delivered, 2) a payment for service delivered, or 3) a component of a service plan. Services
must fall within the NCANDS date parameters to be reported.
The state is not able to report on the following services data elds regarding information and
referral services:
■ Special services-juvenile delinquency
■ Employment services
■ Family planning
■ Housing services
■ Independent and transitional living services
■ Legal services
■ Pregnancy/parenting services for young parents
■ Respite care
Every substantiated investigation involving a child younger than 3 years old, per state policy,
is referred to the Family Infant Toddler (FIT) Program for a diagnostic assessment. The
referral occurs within 2 days of the substantiation. The date of this referral is documented in
the state SACWIS prior to approval of the investigation results. The worker also noties the
family of the referral and provides them with a copy of the FIT fact sheet.
New Mexico no longer offers Family Preservation services per the Family Preservation
Model. New Mexico offers In-Home Services, which is a clinical intervention aimed at
reducing safety threats and enhancing parental protective capacities. In-Home Services is
a 4-to-6-month intervention, specically geared toward families who are at risk of child
removal. New Mexico’s In-Home Services clinicians are all licensed social workers or
licensed clinical counselors.
New Mexico (continued)
Child Maltreatment 2022
Appendix d: State Commentary 235

New York
Contact Hui-Shien Tsao, Ph.D. Phone 518–474–6791
Title Research Scientist
Bureau of Research, Evaluation and Performance
Analytics
Strategic Planning and Policy Development
Email
Address New York State Ofce of Children and Family Services
52 Washington St, Room 323 North
Rensselaer, NY 12144
General
Prior to January 1, 2022, the level of evidence required in NY to substantiate an allegation of
child abuse or maltreatment was “some credible evidence.” Beginning on January 1, 2022, the
level of evidence required was raised to “a fair preponderance of the evidence” standard. New
York State Ofce of Children and Family Services (OCFS) regulations (18 New York Code
Rules and Regulations-NYCRR, section 434.10) dene these terms as follows:
■ “Some credible evidence” is evidence that is worthy and capable of being believed.
■ “A fair preponderance of the evidence” is evidence that outweighs other evidence that is
offered to oppose it.
A core component of the legislative intent behind raising the evidentiary standard was to
address disparities. Overrepresentation of low-income individuals and those of color in the
child welfare system is well documented. The enacted statutory changes will work to rectify
potential employment consequences for allegations of child maltreatment that are not sup-
ported by a fair preponderance of the evidence. The new law does not change the criteria
to be utilized when determining whether to register a report of suspected child abuse or
maltreatment.
Reports
On March 31, 2021, the Marihuana Regulation and Taxation Act (MRTA) was signed into
law legalizing adult-use cannabis (commonly referred to as recreational marihuana). In
response to this change, OCFS notied local districts in April 2022 that the Statewide
Central Register of Child Abuse and Maltreatment (SCR) will “not register a report of
suspected child abuse or maltreatment when the only reported concern is that a birthing
parent and/or an infant tested positive for the presence of cannabis. Additionally, the SCR
continues to not register a report when the only reportable concern is that a parent uses
cannabis products.”
The NY SCR operates 24/7. It is staffed by trained Child Protective Specialists who conduct
a focused interview with the caller and use the information to determine if a report of
suspected abuse or maltreatment can be registered, or if other action is necessary and appro-
priate, such as a Law Enforcement Referral (LER). New York does not collect information
about calls not registered as reports.
In FFY 2022 the number of full-time SCR screening staff decreased 15 percent. NY is facing
a work force challenge and is working to recruit additional staff. While NY maintains a
statewide hotline for CPS referrals, response to accepted referrals is handled at the county
level. New York State law requires that each local department of social services (LDSS)
establish a Child Protective Services unit (CPS) within the LDSS to investigate suspected
child abuse and maltreatment, provide protection from further abuse or maltreatment and
Child Maltreatment 2022
Appendix d: State Commentary 236

offer rehabilitative services for the child or children and parents or caregivers involved.
Investigations must start within 24 hours of receipt of the report and caseworkers are
required to conduct a safety assessment within 7 days of an accepted referral to determine
whether the child named in the report or any other children in the household are in immedi-
ate danger of serious harm.
To allow for a more exible response to families reported to the SCR, New York State
enacted a law in 2007 authorizing a dual track child protective system [SSL §427-a]. The law
prescribes the broad parameters of Family Assessment Response (FAR) and allows LDSSs
that are authorized to establish a FAR program considerable exibility to develop approaches
that best match local resources, stafng capacity, and needs of families.
The law excludes reports containing allegations of sexual abuse, physical abuse, severe or
repeated abuse, abandonment, and failure to thrive from consideration for FAR [SSL §427-
a(3)(a)-(i)]. It also requires an initial assessment of child safety, and if a child is deemed
unsafe, the report may not be handled using FAR [SSL §427-a(4)(c)]. LDSSs can opt to
impose more restrictive eligibility criteria for assignment to FAR than those required by the
statute [SSL §427-a(3), 18 NYCRR 432.13(b)(4)(ii)].
Accepted referrals handled on the CPS track receive a CPS investigation and are determined
to be indicated or unfounded. Data from both traditional Child Protective Services path and
FAR path are reported in NCANDS.
Prior to FFY 2021, approximately 10 percent of NY reports submitted to NCANDS were
mapped to the “other” report source category. To address this concern, NY revised its report
source mapping rules beginning with the FFY 2021 submission. Under these new rules
several report sources previously attributed to “other” were reassigned to existing NCANDs
categories. For example, reporters from shelters, community agencies or service providers
were reassigned to the “Social Service Personnel” category. Additional changes included
moving “Substance Abuse Counselors” to the “Mental Health Personnel” category; “Parent
Substitute” and “Guardian” to the “Parent” category; and “Godparent”, “Non-relative”,
“Concerned Citizens”, and “Unrelated Household Members” to the “Friends and Neighbors”
category. These changes signicantly reduced the percentage of reports attribute to the
“Other” reporter source.
Children
NY has an allegation type of “Parent Drug/Alcohol Use.” During the investigation, CPS case-
workers can document the drug or alcohol use of the caregivers, giving the state the capability
to separate caregivers’ use of drugs from use of alcohol. This allegation does not directly cor-
respond to any of the predened NCANDS maltreatment type categories. Beginning with the
FFY 2021 le, NY changed its mapping rules to move this allegation from “Other” to “Neglect
or Deprivation of Necessities.”
Not all children reported in the Child File have AFCARS IDs because the State uses different
child identiers for child protective service cases and child welfare cases. If a child’s system
involvement is limited to CPS investigation, the child will not be assigned a child welfare
New York (continued)
Child Maltreatment 2022
Appendix d: State Commentary 237

identier (i.e., AFCARS ID). Additionally, the Justice Center for the Protection of People with
Special Needs which investigates reports of institutional abuse uses a different child identier.
Ideally a child should have a single child protective services case id that spans across all
CPS reports. However, in some instances a child is assigned a new child protective services
case id when a new report is received, resulting in some children having more than one
child protective services case id. New York State is exploring ways to detect and reduce the
circumstances that lead to multiple child protective case ids per child.
Information on “child alcohol and drug abuse” risk factors was reported for the rst time in
FFY 2020. In NYS accepted allegations include “child drug or alcohol abuse” and “parent drug
or alcohol abuse.” If a child is over the age of one and named as an alleged victim of an allega-
tion of child drug or alcohol abuse, the child is identied in the NCANDS le as having a drug
or alcohol risk. If a child is under the age of one and named as an alleged victim of parent drug
or alcohol abuse and one or more additional risk factors are checked (positive tox, withdrawal,
Fetal Alcohol Spectrum) the child is identied in NCANDS as having a drug or alcohol risk.
For every child younger than one year old named as an alleged victim of parent drug or alco-
hol abuse, where one or more additional risk factors are checked (positive tox, withdrawal,
Fetal Alcohol Spectrum), NY requires that information on plans of safe care and service
referral be completed, regardless of reporter type. This differs from NCANDS rules, which
state that information on plans of safe care and referral only be provided when the reporter
was classied as “medical personnel.” In NY, many reporters identify by professional quali-
cation (e.g., social worker) rather than setting (e.g., medical personnel). As a result, while NY
maintains information on the plan of safe care and referral for all children identied in the
NCANDS le as substance exposed, the plan of safe care and referral numbers reported in
the NCANDS le are limited to those cases in which the report source identied as medical
personnel, under reporting the number of children in each category. Information on plans of
safe care and service referral is reported for the entire FFY 2022.
In FFY 2022, NY reported an 11 percent decrease in the unique child victims. This change is
likely driven by the change in evidentiary standards described above.
Fatalities
By state statute, all child fatalities due to suspected abuse and neglect must be reported by
mandated reporters, including, but not limited to, law enforcement, medical examiners,
coroners, medical professionals, and hospital staff, to the Statewide Central Register of Child
Abuse and Maltreatment. No other sources or agencies are used to compile and report child
fatalities due to suspected child abuse or maltreatment. NY also has a state Child Fatality
Review Team that fulls oversight and reporting roles.
State practice allows for multiple reports of child fatalities for the same child and deaths that
occurred in previous years to be reported to the State Central Register (SCR). These fatalities
are then investigated, and dispositions made. This practice allows for reporting of fatalities
reported in previous NCANDS les to be reported again. After further review of reporting
instruction and clarication with NCANDS technical assistance, NY revised how it reports
fatalities within NCANDS starting in FFY 2020. NY now includes all fatalities regardless
New York (continued)
Child Maltreatment 2022
Appendix d: State Commentary 238

the date of death to NCANDS fatality reporting, as long as the fatality report investigation
ended during the reporting period and the fatality had not been reported in a prior NCANDS
submission.
Perpetrators
In NY, any of the following persons who are allegedly responsible for causing injury, abuse
or maltreatment to, or allowing injury, abuse or maltreatment to be inicted on, a child
named in a report to the SCR may be a subject of a report:
■ A child’s parent or guardian; or other persons legally responsible
■ A director, operator, employee or volunteer of a home operated or supervised by an autho-
rized agency, OCFS, a family day-care home, a day-care center, a group family day-care
home, or a school-age child care program; who allegedly is responsible for causing injury,
abuse, or maltreatment to a child who is reports to the Statewide Central Register of child
abuse or maltreatment, or who allegedly allows such injury, abuse or maltreatment to be
inicted on such child.
There is no age limitation for parents. Noncaregivers are not considered legally responsible
individuals, and thus do not meet the criteria as a subject in a registered report.
Prior to FFY 2022, perpetrator relationship was missing or unknown in approximately 6
percent of cases submitted to NCANDS. For the FFY 2022 submission, NYS revised the
programming used to determine perpetrator relationship. As result of this change, there is a
noticeable increase in the “unmarried partner of parent” relationship category.
In FFY 2022, NY reported an 11 percent decrease in the unique perpetrators. This change is
likely driven by the change in evidentiary standards described above.
Services
The State is not currently able to report the NCANDS services elds. Title XX funds are
not used for providing child preventive services in this state. Local departments of social
services provide all services, and many of those services are contracted services with various
preventive agency providers. NY does provide funding for primary prevention programs
such as the Healthy Families New York home visiting program.
New York (continued)
Child Maltreatment 2022
Appendix d: State Commentary 239

North Carolina
Contact Joy Smith Phone 919–527–6433
Title Data Analyst Email
Address NC Division of Social Services–Performance Mgmt Section
820 S. Boylan Avenue, 2415 Mail Service Center
Raleigh, NC 27699-2401
The state did not submit commentary for the Child Maltreatment 2022 report.
Child Maltreatment 2022
Appendix d: State Commentary 240

North Dakota
Contact Jenn Grabar Phone 701–328–1863
Title Child Maltreatment and Fatality Manager
Children and Family Services
Email
Address North Dakota Department of Health and Human Services
600 E Boulevard Avenue, Dept 325
Bismarck, ND 58505
General
North Dakota implemented a central “hotline,” the Child Abuse and Neglect Reporting
Line, for the receipt of reports of suspected child abuse and neglect in January 2021. Since
the inception of this centralized process, the number of reports received has continued to
increase, resulting in an increase in completed assessments. On August 1, 2021, there was
a change to state law and policy that provides for a denition of impending danger. North
Dakota Century Code Chapter 50-25.1-02(15) denes “impending danger” as a foreseeable
state of danger in which a behavior, attitude, motive, emotion, or situation can be reason-
ably anticipated to have severe effects on a child according to criteria developed by the
Department. Two determinations are made upon the conclusion of a child protection assess-
ment, one that determines if a child meets the denition of an abused or neglected child and
another that determines if impending danger threats are present.
The presence of impending danger threats mandate child welfare involvement through case
management (protective services), either in-home or out-of-home. The provision of protective
services is now no longer directed by substantiated maltreatment, but rather the presence of
impending danger threats to a child’s safety. Substantiated child victims remain those with
identied maltreatment. Once case management (protective services) begins, the caseworker
must continually assess the parents/caregivers, children, and alternate caregivers (when appli-
cable to the case) on an ongoing basis to ensure all needs are addressed through appropriate
services and progress towards goal achievement is being made. The state’s decrease in child
victims and perpetrators is likely due to the above-mentioned changes to statute and policy.
It is noted that although there was a decrease in identied victims, there was an increase in
those receiving prevention services.
In addition, the state’s child abuse and neglect law changed on August 1, 2021, to allow for
a child protection services decision of “Unable to Determine.” State statue denes the child
protection services decision of “unable to determine” as insufcient evidence is available to
enable a determination whether a child meets the denition of an abused or neglected child.
These assessments are coded as closed, no nding. The previous reporting period did not
include a full year of utilization of this type of report disposition, resulting in the marked
increase of this type of determination this year, as well as likely impacted decrease in other
types of assessment determinations.
State law denes three types of assessments that may be carried out in response to a report of
suspected child abuse and neglect:
■ Alternative Response Assessment–means a child protection response involving substance
exposed newborns which is designed to provide referral services to and monitor support
services for a person responsible for the child’s welfare and the substance exposed new-
born; and to develop a plan of safe care for the substance exposed newborn.
Child Maltreatment 2022
Appendix d: State Commentary 241

■ Child Protection Assessment–means a factnding process designed to provide informa-
tion that enables a determination of whether a child meets the denition of an abused or
neglected child, including instances that may not identify a specic person responsible for
the child’s welfare which is responsible for the abuse or neglect.
■ Family Services Assessment–means a child protection services response to reports of
suspected child abuse or neglect in which the child is determined to be at low risk and
safety concerns for the child are not evident according to guidelines developed by the
department.
The alternative response assessments are exclusive to substance exposed newborns. The
assessments are considered voluntary; however, prenatal substance exposure is a form of
neglect as identied in state law. Caregivers who decline to participate in an alternative
response assessment receive a child protection services assessment response. Other primary
reasons for an alternative response assessment to revert to a child protection services assess-
ment include a violation of the plan of safe care that places the infant in danger and the
receipt of new reports that allege a different maltreatment or victims.
The family services assessment was implemented statewide in March 2022 after being pilot
tested in four Human Service Zones. The primary suspected maltreatment receiving a family
services assessment is educational neglect. Data elements for the Alternative Response
Assessment and Family Services Assessment response have been added to the child welfare
data management system, however, they have not yet been mapped to the NCANDS Child
File. The total number of completed Alternative Response Assessments in FFY 2022 is 122.
The total number of completed Family Services Assessments in FFY 2022 is 85.
North Dakota Century Code requires that all reports of suspected child abuse and neglect
be reported to the Department of Health and Human Services through its authorized agent
and requires that any report must be accepted: “The department or authorized agent, in
accordance with rules adopted by the department, immediately shall initiate a child protec-
tion assessment, alternative response assessment, or family services assessment or cause an
assessment, of any report of child abuse and neglect, including, when appropriate, the child
protection assessment, alternative response assessment, or family services assessment of the
home or the residence of the child, any school or child care facility attended by the child, and
the circumstances surrounding the report of abuse or neglect.” The statute for child abuse
and neglect (North Dakota Century Code Chapter 50-25.1) was changed on August 1, 2021,
to allow child protection services assessment decisions as follows:
■ Conrmed–means that upon completion of a child protection assessment, the department
determines, based upon a preponderance of the evidence, that a child meets the denition
of an abused or neglected child, and the department conrms the identity of a specic
person responsible for the child’s welfare which is responsible for the abuse or neglect.
■ Conrmed With Unknown Subject–means that upon completion of a child protection
assessment, the department determines, based upon a preponderance of the evidence,
that a child meets the denition of an abused or neglected child, but the evidence does
not conrm the identity of a specic person responsible for the child’s welfare which is
responsible for the abuse or neglect.
North Dakota (continued)
Child Maltreatment 2022
Appendix d: State Commentary 242

■ Unable to Determine–means insufcient evidence is available to enable a determination
whether a child meets the denition of an abused or neglected child. These assessments
are coded as closed with no nding.
■ Unconrmed–means that upon completion of a child protection assessment, the depart-
ment has determined, based upon a preponderance of the evidence, that a child does not
meet the denition of an abused or neglected child.
Reports
North Dakota encompasses four American Indian Reservations. These reservations are sov-
ereign nations, each of whom maintains the reservation’s own child welfare system. Because
of this, North Dakota’s NCANDS data does not include child abuse and neglect data, or data
on child deaths from abuse or neglect or near deaths from abuse or neglect which occurred in
a tribal jurisdiction.
North Dakota statute does not allow referrals (reports) to be screened out. All referrals must
be accepted and assessed to some degree. North Dakota has an administrative assessment
process to correctly triage reports received. Data regarding the number of children included
in reports that are administratively assessed is not collected. An administrative assessment is
dened as the process for documenting the disposition of Child Protection Services Intakes
that fall outside the criteria for a report of suspected child abuse or neglect. Under this deni-
tion, reports can be administratively assessed when the concerns in the report clearly fall
outside of the state child protection law. Such circumstances include:
■ The report does not contain a credible or causal reason for suspecting the child has been
abused or neglected
■ The report does not contain sufcient information to identify or locate the child or family
(after performing due diligence)
■ There is reason to believe the reporter is willfully making a false report (these reports are
referred to the county prosecutor)
■ The concern in the report has been addressed in a prior assessment
■ The concerns are being addressed through county case management or a Department of
Health and Human Services therapist
■ Reports of pregnant women using controlled substances or abusing alcohol (when there
are no other children reported as abused or neglected) are also included in the category
of administrative assessments, as state law doesn’t allow for a decision of “conrmed”
(substantiation) in the absence of a live birth.
Assessments that are in progress when information found during the assessment indicates
the reported concerns fall outside the denitions in the child abuse and neglect law are then
terminated in progress. Reports may also be referred to another jurisdiction when the children
of the report are not physically present in the Human Service Zone (these reports are referred to
another jurisdiction (tribal, or state), where the children are present or believed to be present).
Reports involving a Native American child living on an Indian Reservation are referred to
tribal child welfare systems or to the Bureau of Indian Affairs child welfare ofce. Reports
concerning sexual abuse or physical abuse by someone who is not a person responsible for
the child’s welfare (non-caregiver) are referred to law enforcement. The total number of
administrative assessments or referrals in FFY 2022 is 11,484. This total breaks down to
North Dakota (continued)
Child Maltreatment 2022
Appendix d: State Commentary 243

5,700 administrative assessments; 2,435 administrative referrals; 3,61 terminated in progress
(14 were alternative response assessments terminated in progress); and 188 pregnant woman
assessments. There were 2,912 completed full assessments.
Data mapping and calculating the response time, both in the Agency File and in the Child
File, has proven to be quite challenging as there had been a signicant divergence between
the state’s administrative rule and policies and the denitions required for NCANDS report-
ing. State administrative rule was amended on April 1, 2022, to allow initiation of an assess-
ment to be done by contact with the subject of the report, by contact with the alleged abused
or neglected child or by contact with a law enforcement ofcer with jurisdiction in the loca-
tion where the child may be found or where the alleged abuse or neglect occurred. Previous
to this change, contact with the alleged abused or neglected child was not included in the
administrative code. Therefore, many assessments initiated under the previous state’s admin-
istrative rule do not meet the initiation denition in the Child File or Agency File. Child
Protection Services Policy for initiation changed with the adoption of the Safety Framework
Practice Model in December 2020, which states that initiation of child protection assessments
is face to face contact with all reported child victims, the initial face to face contact with a
victim must be completed by child welfare, is no longer allowed to be conducted prior to the
report date and the timeline for contact with victims does not exceed three days.
When response time is calculated according to state policy and administrative rule during
FFY 2022, the response time is 265 hours. Workforce challenges are present statewide with
the primary impact being higher caseloads than desired and increased response time to
reports not identifying present danger. Several agencies have numerous vacancies, result-
ing in extremely high caseloads and decreased capacity. Vacancies are being lled with a
younger, less experienced workforce, increasing the need for training and supervision.
North Dakota is a county administered system, the state can only determine the numbers
of Full- Time Equivalents (FTEs) employed by a county for certain job titles, such as Social
Worker or Family Service Specialist. These FTEs may be employed in various county
programs for varying portions of their FTE. For Example: A county employee may be a full
FTE, but ¼ time will be CPS functions, ¼ time maybe foster care, ¼ time may be in adult
services, and ¼ time may be in-in home case management. The state has no independent way
to determine what portions of the FTE are dedicated to CPS functions.
North Dakota implemented a centralized intake “hotline” (ND Central Child Abuse and
Neglect Reporting Line) for reporting suspected child abuse and neglect in January 2021. The
workforce for this unit is comprised of 15 county FTE’s. In an attempt to glean the required
information for NCANDS reporting, the state has completed a survey of the 19 Human Service
Zones (formerly county social service agencies) in which the Human Service Zones are asked
to report the number of FTEs in their agency dedicated to CPS functions. An electronic survey
was prepared in two sections, using Survey Monkey as the vehicle for collecting the data. This
survey was transmitted via email to directors of all Human Service Zones in the state. The
survey was administered in May 2022 and represents the workforce for FFY 2021. Directors
reported a total of 130 employees, including supervisors, responsible for intake and assessment.
Of these 130 FTEs, 15 were responsible for CPS intake functions, 100 were responsible for CPS
assessment functions, and 18 were responsible for supervision functions. The second portion of
North Dakota (continued)
Child Maltreatment 2022
Appendix d: State Commentary 244

the survey was forwarded to the workers and supervisors by the director with a request for each
worker listed by the director to complete the education/training and demographic portion of the
survey. The worker demographic and training portion of the survey was completed by 80 of the
workers/supervisors, for a response rate of 62 percent. The results of the worker demographic
portion of the report are included in the state’s CAPTA report.
Children
As mentioned, there was a decrease 16 percent in child victims this reporting period and
this is likely the result of the previously mentioned change in state statute and policy, adding
the presence of impending danger as the determining factor in accessing postassessment
protective services, rather than substantiated maltreatment. When children do not meet the
denition of an abused or neglected child, yet there is identied impending danger, protective
services to address child’s safety is now mandated, even without the maltreatment substantia-
tion. This has also resulted in an increase in children receiving preventative services.
Due to mapping requirements and limited data resources, NCANDS mapping for risk factor
data elements are limited for this reporting period. The data reporting is expected to improve
when the revised risk factor changes are mapped for NCANDS reporting. Data elds have
been added to the child welfare data management system to capture the maltreatment type
of sex trafcking as well as sex trafcking as a child risk factor. This data has not yet been
mapped for NCANDS reporting. There were zero children identied with a conrmed
maltreatment of sex trafcking in FFY 2022 and 7 children with an identied child risk
factor for sex trafcking. An identied child risk factor indicates that trafcking may have
occurred by someone who is not a “person responsible for a child’s welfare” under state law.
Child victim counts with a caregiver risk factor for alcohol abuse is 187, methamphetamine
use is 329, opioid use is 93, other drug use by caregiver is 373. Child victim risk factor counts
for prenatal exposure to alcohol is 18, prenatal exposure to methamphetamine is 105, prenatal
exposure to opioids is 27 and prenatal exposure to other drugs is 158. In addition, the child
victim risk factors for environmental exposure to methamphetamine is 320 and environmen-
tal exposure to all other drugs is 439.
The lead agency completed the process of analysis and design to incorporate data system
changes for the data reporting elements for prenatally substance exposed infants, however
appropriate mapping for NCANDS continues to be delayed for technical and resource
reasons, including priority for the development of a new child welfare data management
system. Program data reports as well as data management system development pull from the
same pool of data resources available to Health and Human Services and this is beyond the
control of the program.
According to state law a “Substance Exposed Newborn” is dened as an infant younger
than twenty-eight days of age at the time of the initial report of child abuse or neglect and
who is identied as being affected by substance abuse or withdrawal symptoms or by a fetal
alcohol spectrum disorder. The state law requires referral services and monitoring of support
services for caregivers as well as a Plan of Safe Care for the newborn, mirroring the federal
CARA legislation amending CAPTA. Notication of substance exposed newborns by health
care providers are reported as child maltreatment. State statute denes a “neglected child” as
“subject to prenatal exposure to chronic or severe use of alcohol or any controlled substance
North Dakota (continued)
Child Maltreatment 2022
Appendix d: State Commentary 245

as dened in section 19-03.1-01 in a manner not lawfully prescribed by a practitioner.” There
were 166 substance exposed newborns identied during FFY 2022. Of the 166 identied
substance exposed newborns, 152 of them had a Plan of Safe Care developed (92 percent); all
166 of these substance exposed newborns and their affected caregivers received some degree
of appropriate services. The most frequently identied reasons for lack of a Plan of Safe Care
included: toxicology testing conrmed the infant was not drug exposed and lack of coopera-
tion from the caregiver. There were 26 additional identied substance exposed infants (under
one year of age), those over the age of 28 days when the report/notication is received, in
FFY 2022. Of these 26 identied substance exposed infants, 25 of them had a Plan of Safe
Care developed (96 percent).
Fatalities
All fatalities were reported in the Child File. The North Dakota Department of Health and
Human Services, Children and Family Services is the agency responsible for coordination
of the statewide Child Fatality Review Panel as well as serving as the state’s child welfare
agency. The Child Maltreatment and Fatality Administrator / Prevention and Protection
serves as the Presiding Ofcer of the Child Fatality Review Panel. This dual role provides
for close coordination between these two processes and aides in the identication of child
fatalities due to child abuse and neglect as a sub-category of child fatalities from all causes.
The North Dakota Child Fatality Review Panel coordinates with the North Dakota
Department of Health and Human Services Vital Records to receive death certicates for
all children, ages 0–17 years, who receive a death certicate issued in the state. These death
certicates are screened against the child welfare database and any child who has current
or prior CPS involvement as well as any child who it can be determined is in the custody of
county Human Service Zones or the Division of Juvenile Services at the time of the death is
selected for in-depth review by the Child Fatality Review Panel, along with any child whose
Manner of Death as listed on the Death Certicate is “Accident”, “Homicide”, “Suicide” or
“Undetermined”. Any child for whom the Manner of Death is listed on the Death Certicate
as “Natural”, but whose death is identied as sudden, unexpected, or unexplained is also
selected for in-depth review. As part of these in-depth reviews, records are requested from
any agency identied in the record as having involvement with the child in the recent period
prior to death, including law enforcement, medical facilities, Child Protection Services,
the County Coroner, and the State Medical Examiner’s Ofce for each death. Under North
Dakota law, any hospital, physician, medical professional, medical facility, mental health pro-
fessional, mental health facility, school counselor, or division of juvenile services employee
shall disclose all records of that entity with respect to any child who has or is eligible to
receive a certicate of live birth and wo has died. Additionally, the State Medical Examiner’s
Ofce forensic pathologists participate in conducting the reviews. Data from each review
is collected and maintained in a separate database. It is this database that is correlated with
data extracted from the child welfare database for NCANDS reporting. Even though the
NCANDS data does not contain child welfare data concerning children in tribal jurisdiction,
the state is condent that all deaths in the state from all causes are identied, reviewed, and
reported. Another safeguard in data reporting is that the child welfare agency is also the
entity that convenes the Child Fatality Review Panel, reviews the records for each death,
compiles that data following the reviews and publishes the annual Child Fatality Review
Panel Data report as well as being responsible for NCANDS reporting.
North Dakota (continued)
Child Maltreatment 2022
Appendix d: State Commentary 246

Perpetrators
State law limits CPS actions to reports involving “a person responsible for a child’s welfare”,
dened as “an individual who has responsibility for the care or supervision of a child and
who is the child’s parent, an adult family member of the child, any member of the child’s
household, the child’s guardian, or the child’s foster parent; or an employee of, or any person
providing care for the child in, a child care setting. (N.D.C.C. 50-25.1-02(1)). Reports which
do not meet statutory denitions mandated to CPS, but which may be a potential viola-
tion of criminal law are to be “disposed” through referral to law enforcement (N.D.C.C.
50-25.1-05.3).
For the purposes of institutional child abuse and neglect, “a person responsible for the
child’s welfare” means an institution that has responsibility for the care or supervision of a
child. Under state statute, “Institutional child abuse or neglect” means situations of known
or suspected child abuse or neglect when the institution responsible for the child’s welfare
is a public or private school, a residential facility or setting either licensed, certied, or
approved by the department, or a residential facility or setting that receives funding from the
department. The following are excluded: correctional, medical, home and community based
residential rehabilitation and educational boarding care settings. An individual working as
facility staff is not held culpable within Institutional Child Protection Services, rather, the
facility itself is considered to be the “subject’ (perpetrator) of the report. Assessments of
institutional child abuse or neglect are assessed at the state level (DHHS) rather than at the
county (Human Service Zone) level as are CPS reports that are non-institutional. All reports
of institutional child abuse and neglect are reviewed by a multi-disciplinary State Child
Protection Team on at least a quarterly basis. Determinations of institutional child abuse
and neglect are made by team consensus. A determination of “indicated” means that a child
was abused or neglected by the facility. A decision of “not indicated” means that a child was
not abused or neglected by the facility. State law was changed on August 1, 2021, moving
individual perpetrators from public and private schools out of child protection services and
added them to institutional child protection services; thus, teachers and other education
professionals are no longer perpetrators rather the school is seen as the subject.
There were 155 reports of Institutional Child Abuse or Neglect in FFY 2022, making up 48
completed full assessments. Of these 48 assessments, 42 had a nding of “not indicated” and
6 had a nding of “indicated”. There were 68 assessments Terminated in Progress, and 36
reports were administratively assessed/administratively referred (see above under ‘reports’
for denitions of administrative assessments and referrals). Three (3) reports remained open
at the time of this report.
North Dakota reports unknown perpetrators as Unknown within the state’s child welfare
data management system (FRAME). Perpetrator IDs for unknown perpetrators are unique to
each assessment. State law allows for a child protection services assessment determination of
“conrmed with an unknown subject” which means that upon completion of a child protec-
tion assessment, the department determines, based upon a preponderance of the evidence,
that a child meets the denition of an abused or neglected child, but the evidence does not
conrm the identity of a specic person responsible for the child’s welfare which is respon-
sible for the abuse or neglect.
North Dakota (continued)
Child Maltreatment 2022
Appendix d: State Commentary 247

Data elds have been added to the child welfare data management system to capture sex traf-
cking by a noncaregiver. This data has not yet been mapped for NCANDS reporting. There
were 14 reported perpetrators of sex trafcking that were identied as noncaregivers.
Services
The methods for Agency File Data components 5.1 and 5.2 include only children less than
3 years of age. The number of children eligible for referral for IDEA is 111. The number of
children actually referred is 102. Of the 9 children eligible and not referred, ve (5) children
moved out of state, two (2) children had been previously referred and were receiving IDEA
services. The reason for non-referral for the remaining two children was not available.
The state has limitations when reporting reunication services. Case management services
provided by county agencies (Human Service Zones) are dependent upon correct data entry
connecting the service with the CPS assessment. Additionally, services provided through
referral to service providers outside the county agency may only be documented in narrative
form, which prohibits data extraction.
On Aug. 17, 2020, North Dakota became the seventh state in the country to receive approval
of its Family First Prevention Services Act Title IV-E Prevention Services Plan ND from the
federal Children’s Bureau. The plan provides the state access to federal Title IV-E funding
for approved evidence-based prevention services proven to strengthen and stabilize children
and families so children can stay in their family home safely. Services include both mental/
behavioral health and substance abuse treatment and recovery support services as well as
in-home parent skill-based programs. The state’s eligibility application and portal went live
February 2021 with prevention services starting March 1, 2021. There are nine approved
prevention services eligible for Tile IV-E reimbursement, they are:
■ Healthy Families
■ Parents as Teachers
■ Nurse-Family Partnership
■ Homebuilders
■ Brief Strategic Family Therapy
■ Parent-Child Interaction Therapy
■ Multisystemic Therapy
■ Functional Family Therapy
■ The Family Check-Up
Community agencies and private service providers can apply to become an approved Title
IV-E prevention services provider by completing an application. Title IV-E providers must
identify the approved Title IV-E prevention service(s) they want to provide, submit verica-
tion they have the required qualications, training, certication and/or accreditation to
provide the service, outline their delity review process, and agree to the responsibilities and
requirements set forth by ND Children and Family Services Division (CFS) and the Family
First Prevention Services Act.
North Dakota (continued)
Child Maltreatment 2022
Appendix d: State Commentary 248

Ohio
Contact Denielle Ell-Rittinger Phone 614–752–1143
Title Program Administrator
Ofce of Families and Children
Email
denielle.ell-rittinger@jfs.ohio.gov
Address Ohio Department of Job and Family Services
PO Box 183204
Columbus, OH 43218–3204
General
Ohio implements a Differential Response (DR) System for screened in reports of alleged
child abuse and/or neglect. The DR system is comprised of a traditional response (TR)
pathway and an alternative response (AR) pathway. Children who are subjects of reports
assigned to the AR pathway are mapped to NCANDS as AR nonvictim and have a disposi-
tion of “AR.” Those who are “alleged child victims” of reports assigned to the TR pathway
receive a disposition:
■ Unsubstantiated—the assessment/ investigation determined no occurrence of child abuse
or neglect.
■ Substantiated—there is an admission of child abuse or neglect by the person(s) respon-
sible; an adjudication of child abuse or neglect; or other forms of conrmation deemed
valid by the Public Children Services Agency (PCSA).
■ Indicated—there is circumstantial or other isolated indicators of child abuse or neglect
lacking conrmation; or a determination by the caseworker that the child may have been
abused or neglected based upon completion of an assessment/investigation.
Reports
The number of screened out referrals between FFY 2021 and FFY 2022 showed an increase.
Ohio is a state supervised, county administered, child protection services program and does
not operate a state referral hotline. Ohio continues to operate a centralized state referral
hotline which provides the referent with the local county PCSA referral contact information.
The intake of referrals is required to be received by each county PCSA. The requirements
established for recording referral information received, completing a screening decision
of the referral, conducting assessment/investigations of alleged abuse or neglect are main-
tained per Ohio Administrative Code rules. During the review period, provisions to rules
governing face to face monthly contacts and parental visits for cases receiving ongoing
case planning services were relaxed based on federal guidance during the pandemic. When
State Emergency Orders were lifted many counties reported a workforce crisis. Ohio PCSAs
continue to have a high number of vacancies and staff turn-over. The Ohio Department of
Job and Family Services (ODJFS) have increased efforts in addressing the retainment and
recruitment of child protective services caseworkers.
The revised Ohio Child Protective Services Screening Guidelines were released on
September 7, 2022. This guide was revised and reformatted to provide child welfare profes-
sionals enhanced guidance of screening examples along with a streamlined ow within the
document, supporting the decision-making process. References to Ohio Administrative
Code (OAC) and Ohio Revised Code (ORC) were made in the beginning of each section/
sub-section of the categories to assist with decision making. Considerations for each category
have been provided to promote critical thinking during the intake and screening processes.
The revised guidelines inuence statewide consistency and serve as a training resource.
Child Maltreatment 2022
Appendix d: State Commentary 249

Children
Requirements to record the race/ethnicity of children in Statewide Automated Child Welfare
Information System (SACWIS) were effectuated in FFY 2015 and remain in place today.
Child victims as reported by Ohio are children who have received a disposition of substanti-
ated or indicated in the traditional response pathway.
Information is also captured at disposition. There are two identied description of harm
values addressing human trafcking; one for a child trafcked in forced labor, and the other
for a child trafcked in sex. When either is selected by the end-user, the date the incident was
reported to law enforcement is required.
Ohio continues to improve in the reporting of human trafcking. When a referral is received by
the PCSA, and human trafcking is suspected by the reporter, a “human trafcking” checkbox
is selected in Ohio SACWIS. Ohio PCSAs also have the ability to identify a case involving
human trafcking at any point during the assessment/investigation. Often referral information
received regarding a concern of child maltreatment may not be known, or identied as, human
trafcking by the reporter. Initial concerns reported may be regarding the child’s condition of
being neglected or physically abused. During the assessment/investigation processes additional
information may be gathered regarding human trafcking. If this occurs, the PCSA is required
to contact law enforcement. Information is also captured at disposition. There are two identied
description of harm values addressing human trafcking; one for a child trafcked in forced
labor, and the other for a child trafcked in sex. When either is selected by the end-user, the
date the incident was reported to law enforcement is required.
Ohio’s screening guidelines were revised to include ORC denitions of trafcking and the
criminal offenses associated to assist in screening decisions related to trafcking. Universal
human trafcking assessments for all children screened into a PCSA child abuse or neglect
report will assist in the identication of human trafcking and service provision. Human
trafcking assessments and resource links are to be added to assessment and planning tool
eld guides. The eld guides include examples of trafcking in addition to guided questions
for the caseworker. Adoption and Foster Care Analysis and Reporting System (AFCARS) –
elements have been added to Ohio SACWIS and reporting systems to capture sex trafcking
for children in substitute care:
■ 106 Prior Victim of Sex Trafcking
■ 107 Prior Report to Law Enforcement
■ 108 Prior Date of Sex Trafcking Report to Law Enforcement
■ 109 Victim of Sex Trafcking While in Foster Care
■ 110 Report to Law Enforcement for Current Victimization
■ 111 Date of Sex Trafcking Report to Law Enforcement
Ohio’s Comprehensive Addiction Recovery Act (CARA) data collection has improved over
the past few years. Infants with prenatal substance exposure are tracked when child abuse
or neglect is reported and at the completion of the assessment/investigation in the Family
Assessment. In FFY 2022, Ohio worked toward streamlining CARA related reporting with
community partners, software developers, and other states. A mandated reporter portal is
under development. A pilot will begin Spring 2023 with a major metro county PCSA.
Ohio (continued)
Child Maltreatment 2022
Appendix d: State Commentary 250

Since the passage of CARA legislation in 2016, ODJFS has teamed with numerous projects,
initiatives, and workgroups to train and educate the entities who are responsible in serving
infants who are substance exposed and their families. In May of 2020, the Practice and
Policy Academy launched its work on creating a collaborative systemic approach to imple-
mentation of CARA and Plans of Safe Care (PoSC). The Practice and Policy Academy is led
by Ohio Department of Mental Health and Addiction Services and the Ohio Department of
Job and Family Services, with Children and Family Futures previously providing oversight.
The Practice and Policy Academy is comprised of participants from state agencies, state
associations, PCSAs, and other community partners that work with families experiencing
substance use during pregnancy.
In November of 2020, ODJFS, in coordination with Ohio Department of Mental Health and
Addiction Services and the Ohio Family and Children First Council, sent out a Communities
of Support grant application which supports existing and new local community planning and
coordinated service delivery efforts with CAPTA funding.
OFC is creating a standalone CARA Dashboard for PCSA and community use and is explor-
ing new CARA and plan of safe care funding opportunities for PCSAs for State Fiscal Year
2024.
Fatalities
Ohio continued to improve in the collection of data surrounding child fatalities and fewer
errors were made this year. It was determined the mandated reporters statutorily required
to participate on child fatality review boards refer cases of suspected abuse and neglect to
the local PCSA if the PCSA had not received a referral prior to the review. Thus, closing a
potential gap in Ohio’s reporting system. FFY 2022 fatality counts had an increase of 15%
from FFY 2021. Unfortunately, the overall death rate in Ohio due to violence has been on the
rise over the past few years.
Child maltreatment deaths reported in Ohio’s NCANDS submission are compiled from the
data maintained in the SACWIS. The SACWIS data contains information on those children
whose deaths were reported to a PCSA, or children involved in a CPS report who died
during the assessment or investigation period. As a county administered CPS system, Ohio
PCSAs have discretion of which referrals are accepted for assessment or investigation. In
some cases, the PCSA will not investigate a child fatality report unless it is deemed there
was suspected abuse or neglect or other children in the home who may be at risk of harm or
require services. Referrals of child deaths due to suspected maltreatment not accepted by the
PCSA are investigated by law enforcement.
No policy changes were made regarding child fatality reviews for this reporting period.
The ODJFS internal fatality review team was able to continue meeting virtually. ODJFS is
researching ways to improve our internal fatality review team.
Ohio (continued)
Child Maltreatment 2022
Appendix d: State Commentary 251

Perpetrators
The NCANDS category of “other” perpetrator relationship includes nonrelated (NR) child
and NR adult. These are catch-all categories that can be used for an individual who is not a
family member. Guidance continues to be provided to agencies to select the most appropriate
relationship code (e.g., neighbor) instead of using the nonrelated categories.
Ohio does report noncaregiver perpetrators of sex trafcking to NCANDS in the “other”
category as described above. These cases are also tracked at disposition and the date they
were referred to law enforcement entered.
Services
Ohio is continually working to improve the recording of services data in the SACWIS.
Federal grant funds are used for state level program development and support to county
agencies providing direct services to children and families.
Ohio successfully implemented phase one of the Family First Prevention Services Act
(FFPSA) on October 1, 2021. Ohio secured funding for a pilot of the program which ran
April 1, 2021, through October 1, 2021, funded by the Family First Transition Act which was
also part of a bipartisan federal budget bill. Ohio secured a vendor, the Center of Excellence
to ensure statewide capacity building of evidence-based practice models for multi-system
therapy and family functional therapy and to monitor for delity to their model. Ohio’s state
plan was approved for the use of the evidence-based practices known as OhioSTART for
families struggling with substance abuse; Healthy Families America and Parents as Teachers
to help those families in need of in-home parenting-based services. Ohio is moving forward
with amending its State Plan and implementing phase two which will include the evidence-
based programs Triple P Parenting and Motivational Interviewing.
Ohio (continued)
Child Maltreatment 2022
Appendix d: State Commentary 252

Oklahoma
Contact Elizabeth Roberts Phone 405–850–6994
Title Programs Manager II, Child Welfare Services Email
Address Oklahoma Department of Human Services
P.O. Box 25352
Oklahoma City, OK 73125
General
Throughout FFY 2022 OKDHS continued to transform through an intense focus on transpar-
ency and innovation and our commitment to improve the trajectory of Oklahoma families.
OKDHS continues to modernize our real estate footprint to position OKDHS to be even
more scally efcient while adding what we call “access points” for our customers by
embedding our workforce with community partners in locations convenient for people who
need our services. Oversized buildings are being traded for intentionally designed spaces to
better serve customers and our workforce. Using our True North Executive Strategies, we are
building pathways to support, empower and celebrate our staff so they can be more creative
and innovative in their work to serve vulnerable children and families. OKDHS continues to
support a family-strengthening system to help ensure safe homes for all children including
safety, well-being and connections to family, community and cultures; and we tirelessly
pursue every child’s right to connect to a stable and loving family and the support they need
to grow and develop into healthy adults.
In FFY 2022, CWS began the implementation of the Oklahoma Title IV-E Prevention
Program Plan, an optional prevention program authorized through the Family First
Prevention and Services Act, securing ongoing funding for prevention programs and services
to prevent the need for foster care placement, and elevating quality improvement and evalu-
ation of prevention programs. OKDHS is focusing on in-home parent skill-based programs,
SafeCare® and Intercept®, that have been well established within the infrastructure of the
child welfare system and contracted with community-based providers with an established
history of serving families involved with the CW system who have experienced child
maltreatment. These contracted community-based services support the promotion of health,
safety and wellness of Oklahoma’s children and families preventatively, as well as to help
reunite families whose children are in out-of-home care. During the reporting period October
1, 2021 through September 30, 2022 statewide 1,857 families received SafeCare® and 347
families received Intercept®.
OKDHS aims to not bring more families into the CW system, but rather improve prevention
practices and enhance and expand the services and supports that allow for more families to
be served in Family-Centered Services (FCS) and not within foster care. FCS focuses on
prevention and protection to prevent maltreatment so a child can remain with their family
and in their community. CWS continues to utilize multiple strategies toward improving
safety decision-making and increasing positive outcomes for children and families while
also building capacity to accurately identify safety threats, provide appropriate services to
eliminate safety threats, and improve parental protective capacities. Oklahoma has continued
to strengthen programs and services to achieve measurable outcomes that are focused on
prevention and protection to prevent maltreatment and unnecessary removal of children from
their families and placed into foster care through the goals, objectives, and strategies outlined
in the 2020–2024 Child and Family Services Plan (CFSP).
Child Maltreatment 2022
Appendix d: State Commentary 253

It is critical to note that both the delivery of in-home services and data collection have
continued to be affected by the ongoing COVID-19 pandemic. During this reporting period,
OKDHS and the contracted service providers have experienced workforce shortages that
have resulted in less capacity to provide prevention services for families. CWS Programs,
along with support through the existing CWS CQI/QA, continues to collaborate with regional
leadership and contracted services providers to support them towards improved outcomes
of child safety, permanency and well-being, parent/kin caregiver well-being, prevention of
future child maltreatment, and entry into foster care.
Four bills related to Child Welfare Services were passed during the 2022 legislative session.
Of note, HB 2992 adjusts various references to the testimony of child witnesses in certain
court cases, removes references to specic ages, provides general denitions of children in
law, and permits guardians ad litem to be present during proceedings.
Reports
The Oklahoma Department of Human Services has a statewide, centralized hotline to receive
child abuse and neglect reports. An allegation of child abuse or neglect reported in any man-
ner to a DHS county ofce is immediately referred to the Hotline.
Each report received at the Hotline is screened to determine whether the allegations meet
the denition of child abuse or neglect and are within the scope of child protective services
(CPS) assessment or investigation. DHS responds to an accepted report of child abuse or
neglect by initiating an assessment of the family or an investigation of the report in accor-
dance with priority guidelines. The primary purpose of the assessment or investigation is the
protection of the child. For assessments or investigations, DHS gives special consideration to
the risks of any minor child, including a child with a disability, who is vulnerable due to his
or her inability to communicate effectively about abuse, neglect, or any safety threat.
A Priority I report indicates the child is in present danger and at risk of serious harm or
injury. Allegations of abuse and neglect may be severe and conditions extreme. The situation
is responded to immediately, the same day the report is received. Priority II is assigned to all
other reports. The response time is established based on the vulnerability and risk of harm to
the child. Priority II assessments or investigations are initiated within two – to 10-calendar
days from the date the report is accepted for assessment or investigation.
An assessment is conducted when a report meets the abuse or neglect guidelines but does not
constitute a serious and immediate safety threat to a child. An assessment is a comprehensive
review of child safety and evaluation of family functioning and protective capacities conducted
in response to a child abuse or neglect report that does not allege a serious and immediate safety
threat to a child. The assessment uses the same comprehensive review to address allegations,
identify behaviors and conditions in the home that lead to risk factors; and evaluate the protective
capacities of the person responsible for the child’s health, safety, or welfare to address the safety
needs of each child in the family. Assessments do not have ndings. When a child is determined
unsafe in the initial stages of the assessment and the family’s circumstances or the person respon-
sible for care’s (PRFC) behavior poses a risk to the child, an investigation is immediately initiated
by the Child Welfare specialist. The family is told an investigation rather than an assessment is
necessary and the CW specialist immediately follows investigation protocol.
Oklahoma (continued)
Appendix d: State Commentary 254
Child Maltreatment 2022

An investigation is conducted when:
■ a report meets the abuse or neglect guidelines and constitutes a serious and immediate
threat to the safety of a child
■ there have been three or more reports accepted for assessment or investigation regarding
the family
■ the family has been the subject of a deprived petition; or
■ the child was diagnosed with fetal alcohol syndrome or DHS determines the child meets
the denition of drug-endangered child.
Reports that are appropriate for screening out and are not accepted for assessment or investi-
gation are reports:
■ that clearly fall outside the denitions of abuse and neglect per OAC 340:75-3-120, includ-
ing minor injury to a child 10 years of age and older who has no signicant child abuse
and neglect history or history of neglect that would be harmful to a young or disabled
child, but poses less of a threat to a child 10 years of age and older;
■ concerning a victim 18 years of age or older, unless the victim is in voluntary placement
with DHS;
■ where there is insufcient information to locate the family and child;
■ where there is an indication that the family needs assistance from a social service agency
but there is no indication of child abuse or neglect;
■ that indicate a child 6 years of age or older is spanked on the buttocks by a foster or trial
adoptive parent with no unreasonable force used or injuries observed;
■ that indicate the alleged perpetrator of child abuse or neglect is not a PRFC, there is no
indication the PRFC failed to protect the child, and the report is referred to local law
enforcement; and
■ the family resides on tribal land includes tribal members or the family is a tribal foster
home with placement of only tribal custody children and the tribe accepted jurisdiction of
the investigation.
■ Allegations concerning the same incident received from the same or a different reporter
are considered duplicate reports and may be screened out and associated with the original
assigned assessment or investigation.
Allegations concerning the same child and family received within 45 calendar days of a
previously accepted and assigned report are considered subsequent reports and may be
screened out and the allegations addressed in the on-going report, unless the subsequent
report contains allegations of a child death, child near death, child trafcking, or sexual
abuse to a child by a PRFC or other adult who has close contact or access to the child. These
are not screened out as subsequent and the allegations are investigated in a new report.
Children
Oklahoma denes a child as any unmarried person younger than 18 years of age, including
an infant born alive. A drug endangered child is dened as a child who is at risk of suffer-
ing physical, psychological, or sexual harm as a result of the use, possession, distribution,
manufacture, or cultivation of controlled dangerous substances or the attempt of any of these
acts by a Person Responsible For Care (PRFC).
Oklahoma (continued)
Appendix d: State Commentary 255
Child Maltreatment 2022

■ (This term includes circumstances wherein the PRFC’s substance use or abuse interferes
with his or her ability to parent and provide a safe and nurturing environment for the child.
■ Every physician, surgeon, or other health care professional including doctors of medicine,
licensed osteopathic physicians, residents and interns, any other health care professional,
or midwife involved in the pre-natal care of expectant mothers or the delivery or care of
infants who test positive for alcohol or a controlled dangerous substance, must promptly
report the matter to the DHS. This includes infants who are diagnosed with neonatal
abstinence syndrome or fetal alcohol spectrum disorder.
■ Whenever DHS determines that a child meets the denition of a “drug-endangered child”
or was diagnosed with neonatal abstinence syndrome or fetal alcohol spectrum disorder,
and the referral is assigned, DHS conducts an investigation of the allegations and does not
limit the evaluation of the circumstances to an assessment.
■ Whenever DHS determines an infant is diagnosed with neonatal abstinence syndrome or
fetal alcohol spectrum disorder, DHS develops a plan of safe care that addresses the infant
and affected family member or caregiver and, at a minimum, their health and substance
use or abuse treatment needs.
Oklahoma denes a “plan of safe care” as a plan developed for an infant with neonatal absti-
nence syndrome or a fetal alcohol spectrum disorder, upon release from healthcare provider
care that addresses the infant’s and mother’s or caregiver’s health and substance use or abuse
treatment needs.
Oklahoma denes a “substance exposed infant” as a newborn who tests positive for alcohol
or a controlled dangerous substance with the exception of substances administered under
the care of a physician. Oklahoma denes “substance affected infant” as one who was born
experiencing withdrawal symptoms as a result of prenatal drug exposure or fetal alcohol
spectrum disorder as determined by the direct health care provider.
Fatalities
Oklahoma investigates all reports of child death and near death that are alleged to be the
result of abuse or neglect. When DHS has reasonable cause to suspect that a child death or
near-death is the result of abuse or neglect, DHS noties the Governor, the President Pro
Tempore of the Senate, and the Speaker of the House of Representatives of the initial inves-
tigative ndings of the child protective services review. Notice is communicated securely no
later than 24 hours after the reasonable determination of suspicion.
A nal determination of death or near death due to abuse or neglect is made after a report
is received from the ofce of the medical examiner which may extend beyond a 12-month
period. Fatalities are not reported to NCANDS until both the investigation and Child Protective
Services program review, which is inclusive of the nal determination, are completed.
The Child Protective Services Programs Unit program review includes:
■ a review of the case record which is inclusive of the Report to District Attorney; law
enforcement reports; medical examiner’s Report of Autopsy; medical records pertain-
ing to the death or near-death and previous records when applicable; all pertinent case
information.
Oklahoma (continued)
Appendix d: State Commentary 256
Child Maltreatment 2022

■ an assessment of compliance of ndings with CPS standards.
■ requests for additional information when determined necessary.
The Oklahoma Child Death Review Board conducts a review of every child death and near
death in Oklahoma. The Bureau of Vital Statistics forwards all death certicates of persons
under 18 years of age to the Ofce of the Chief Medical Examiner monthly, received during
the preceding month. The Ofce of the Chief Medical Examiner conducts an initial review of
death certicates in accordance to the criteria established by the Child Death Review Board
and refers to the Board cases that meet the criteria.
The Child Death Review Board is composed of 27 members or designees. Fourteen mem-
bers are specied positions, including the Chief Medical Examiner, the Director of the
Department of Human Services, the State Commissioner of Health, the State Epidemiologist
of the State Department of Health, the Director of the Oklahoma State Bureau of
Investigation, and the Chair of the Child Protection Committee of the Children’s Hospital of
Oklahoma. Thirteen of the members are appointed and include law enforcement, attorneys,
social workers, physicians, advocacy, a psychologist, and emergency medical personnel. State
Ofce Child Protective Services staff work closely with the Child Death Review Board and
participate as a member of this board.
Perpetrators
Oklahoma denes a person responsible for the child’s health, safety, or welfare (PRFC) as:
■ the child’s parent, legal guardian, custodian, or foster parent;
■ a person 18 years of age or older with whom the child’s parent cohabitates or any other
adult residing in the home of the child;
■ an agent or employee of a public or private residential home, institution, facility, or day
treatment program;
■ an owner, operator, or employee of a childcare facility whether the home is licensed or
unlicensed; or
■ a foster parent maintaining a therapeutic, emergency, specialized-community, tribal, kin-
ship, or foster family home responsible for providing care, supervision, guidance, rearing,
and other foster care services to a child.
A referral to law enforcement is immediately made either verbally or in writing for the pur-
pose of conducting a possible criminal investigation when, upon receipt of a report alleging
abuse, neglect, or during the assessment or investigation, DHS determines:
■ the alleged perpetrator is someone other than a PRFC (third-party perpetrator)
■ abuse or neglect of the child does not appear attributable to failure on the part of a PRFC
to provide protection for the child.
After making the referral to the appropriate law enforcement jurisdiction, DHS is not respon-
sible for further investigation unless:
■ DHS has reason to believe, or law enforcement has determined that the alleged perpetrator
is a parent of another child, not the subject of the criminal investigation, or is a PRFC of
another child;
Oklahoma (continued)
Appendix d: State Commentary 257
Child Maltreatment 2022

■ The appropriate law enforcement jurisdiction requests DHS participate in the investiga-
tion. When funds and personnel are available, as determined by the DHS Director or
designee, DHS may assist law enforcement in interviewing children alleged to be victims
of physical or sexual abuse.
A prior perpetrator is dened as a perpetrator of a substantiated maltreatment within the
reporting year who has also been a perpetrator in a substantiated maltreatment anytime
back to 1995, the year of implementation of the State Automated Child Welfare Information
System.
Oklahoma reports all unknown perpetrators. “Other” perpetrator relationship includes those
with no relation to the alleged victim and roommate.
Services
Through the CPS safety evaluation and investigation process a nding as to the allegation
of child abuse and neglect is made, along with a determination of the safety of the child in
the home, the protective capacities of the person responsible for the child, and appropriate
ongoing service needs for the family. CPS, through the safety evaluation and investigation
process, determines the need for child abuse and neglect prevention and intervention-related
services and what CW intervention would be the least-restrictive, least-intrusive that
ensures the child is safe. Ongoing service options include a determination that no services
are needed, a referral for community-based services, opening a FCS case, or foster care. In
addition to ISS, SafeCare®, and Intercept®, OKDHS contracts with twelve service providers
for families and children involved in the CW system through CPS or ongoing prevention and
intervention-related services through FCS and Permanency Planning for parents’ assistance
and sexual abuse treatment services. During the reporting period October 1, 2021, through
September 30, 2022, statewide 1268 families received parents assistance services and 486
families received sexual abuse treatment services.
Oklahoma (continued)
Child Maltreatment 2022
Appendix d: State Commentary 258

Oregon
Contact Tammy Freeman Phone 503–884–1049
Title Business Analyst Email
tammy.freeman@state.or.us
Address Dept of Human Services Child Welfare
500 Summer St.
Salem, OR 97304
The state did not submit commentary for the Child Maltreatment 2022 report.
Child Maltreatment 2022
Appendix d: State Commentary 259

Pennsylvania
Contact Elysa Springer Phone 717–409–3933
Title Director of Systems and Data Management Email
elyspringe@pa.gov
Address Bureau of Policy, Programs and Operations,
Division of Systems and Data Management
Ofce of Children, Youth and Families
2525 North 7th Street
Harrisburg Uptown Building
Harrisburg, PA 17110
General
In Pennsylvania, only General Protective Services (GPS) referrals may be screened out. GPS
data is not currently included in Pennsylvania’s NCANDS submission. Reports of suspected
child abuse are not able to be screened out.
Reports
Pennsylvania saw that the total reports of child abuse are increasing to a rate that is more
consistent with totals prior to the pandemic. This was expected, following the decrease in
the total reports during the height of the pandemic, which we attributed to limited/reduced
contact between children and mandated reporters of suspected child abuse.
Children
Again, it can be said that we are observing a re-stabilization of our total numbers of sus-
pected abuse reports following the COVID-19 pandemic.
Fatalities
Our Child Welfare Information System (CWIS) only contains the child abuse investigation
outcome for the referral involving the fatality. The fatality records in the NCANDS populations
all rise to the level of suspected child abuse under the Child Protective Services Law (CPSL). A
death which does not rise to the level of a suspected child abuse referral may be captured in the
system under a different referral type if it does not rise to the level of suspected child abuse, but
it is not tracked as a fatality by our system.
Perpetrators
A perpetrator is dened as a person who has committed child abuse as dened in this sec-
tion. The following shall apply:
(1) The term includes only the following:
(i) A parent of the child.
(ii) A spouse or former spouse of the child’s parent.
(iii) A paramour or former paramour of the child’s parent.
(iv) A person 14 years of age or older and responsible for the child’s welfare or having
direct contact with children as an employee of child-care services, a school or
through a program, activity or service.
(v) An individual 14 years of age or older who resides in the same home as the child.
(vi) An individual 18 years of age or older who does not reside in the same home as the
child but is related within the third degree of consanguinity or afnity by birth or
adoption to the child.
(vii) An individual 18 years of age or older who engages a child in severe forms of traf-
cking in persons or sex trafcking, as those terms are dened under section 103 of
the Trafcking Victims Protection Act of 2000 (114 Stat. 1466, 22 U.S.C. § 7102).
Child Maltreatment 2022
Appendix d: State Commentary 260

(2) Only the following may be considered a perpetrator for failing to act, as provided in this
section:
(i) A parent of the child.
(ii) A spouse or former spouse of the child’s parent.
(iii) A paramour or former paramour of the child’s parent.
(iv) A person 18 years of age or older and responsible for the child’s welfare.
(v) A person 18 years of age or older who resides in the same home as the child.
Pennsylvania’s records would include any incidents of sex trafcking which have a perpetra-
tor who meets the legal denition of a perpetrator of child abuse.
Services
Pennsylvania plans to opt into the Family First Prevention Services Act Title IV-E Prevention
Program and is revising the state ve-year prevention plan for nal submission to the
Administration for Children and Families. Once this plan is approved, Pennsylvania will
begin claiming reimbursement for eligible prevention services. Pennsylvania continues to
incentivize use of evidence-based services to support prevention through the existing special
grants initiative. This initiative provides a higher state funding match for county use of
evidence-based programs, truancy prevention programs, housing support and other promis-
ing practices when compared for the state funding match made available for other service
categories. However, these plans do not impact NCANDS submission data, as preventa-
tive service data is maintained at the county level, and therefore not included in the state
NCANDS submission.
Pennsylvania is state supervised, and county administered for child welfare. As such,
services are provided by the counties and not by the state. Pennsylvania’s Child Protective
Services Law allows for counties to outsource nearly all services except for child abuse
investigation and general protective services assessments. There are many counties within
Pennsylvania who select to outsource services and the counties hold the contracts for these
services, not the state. Again, NCANDS data is not impacted by this information, due to the
fact that this data is currently maintained within the county systems and not the state Child
Welfare Information System, and therefore is not currently part of Pennsylvania’s NCANDS
data submission.
Pennsylvania (continued)
Child Maltreatment 2022
Appendix d: State Commentary 261

Puerto Rico
Contact Lisa M. Agosto Carrasquillo/Glenda Gerena Ríos Phone
Title Director of Central Registry/ Administrator ADFAN Email
glenda.gerena@familia.pr.gov
Address Division Administrator for Families and Children (ADFAN)
Family Department
185 Roosevelt Avenue, San Juan PR 00910
The Puerto Rico Department of the Family (DF) is the agency of the Government of Puerto
Rico responsible for the provision of the diversity and /or a variety of social welfare ser-
vices. As an umbrella agency, four Administrations operate with scal and administrative
autonomy.
The Department of the Family composition is as follows:
■ Ofce of the Secretary
■ Administration for Children and Families- ACF (ADFAN, Spanish acronym)
■ Administration of the Socioeconomic Development of the Family (ADSEF, Spanish
acronym)
■ Child Support Administration (ASUME, Spanish acronym), enacted by PL 86, August 17,
1994
■ Administration for Integral Development of Childhood (ACUDEN, Spanish acronym)
PL-179 August 1, 2003
The Administrations are agencies dedicated to executing the public policy established by the
Secretary, in the different priority areas of services to children and their families including the
elderly population in Puerto Rico. It establishes the standards, norms, and procedures to man-
age the programs and provide the operation and supervision of the Integrated Services Centers
(ISC) at the local levels. The regional levels (10 regional ofces) supervise the local ofces.
They are also responsible for implementing and developing those functions delegated by the
Secretary through the redenition and reorganization of the variety of services for the family
including traditional services and the creation of new methods and strategies for respond-
ing to the needs of families. Work plans are prepared in agreement with the directives and
require nal approval of the Secretary.
Administration for Children and Families (ADFAN):
The functions and responsibilities of ADFAN are executed through the following program-
matic and administrative components:
■ Administrator’s Ofce
■ Assistant Administration for Adults and Community Services
■ Assistant Administration for Prevention and Community Services
■ Assistant Administration for Child Protective Services,
■ Family Preservation and Support Services
■ Assistant Administration for Foster Care and Adoption
Assistant Administration for Child Protective Services
The Assistant Administration for Child Protective Services is responsible for the investiga-
tion of intra-familial and institutional CA/N referrals. As one of its primary components,
the State Center for the Protection of Children is responsible for the operation of the Child
Abuse and Neglect Hotline and the Orientation and Family Support Hotline. Both lines are
Child Maltreatment 2022
Appendix d: State Commentary 262
787–625–4900 X 1734/1800

responsible for providing an expedited system of communication to receive family and/or
institutional referrals and to provide orientation and crisis intervention in different areas of
family life. It also operates the Central Registry, which maintains updated statistical and
programmatic information about the movement of CAN referrals and cases receiving ser-
vices by ADFAN.
General
In Puerto Rico it has not been established changes in policy processes related to child
abuse investigations. Puerto Rico does not have an alternative response in child abuse
investigations.
Reports
This year did not reect a signicant change compared to the previous year. The percentage
difference was 3 percent less this year in reports.
The call screening process has not changed. The protocol establishes the entire procedure
involved in handling calls received on the hotline and the questions to better screen the
decision-making process when accepting referrals for social investigation.
Stage One: Receipt of Referral
The process involving the collection of information at the Abuse, Institutional Abuse,
Neglect and Neglect Hotline or local ofce, screening of the referral, assignment of response
priority and transfer to the appropriate work unit shall not exceed a time frame of two (2)
hours from the receipt of the call. This procedure shall be applicable to any situation in which
abuse is alleged in a family home, foster home or family resource home.
The hotline management in coordination with the agency establishes plans to offer training
to new staff.
The number of employees is calculated using the equivalent of full time This calculation is
used in the direct line and with all staff dedicated to referral research in the agency.
Children
The number of child victims decreased this year compared to the previous year.
The MANUAL OF RULES, PROCEDURES AND RULES OF EXECUTION OF THE
SECURITY MODEL IN THE INVESTIGATION OF REFERRALS reviewed in April
2013, establishes the fundamental objectives of the child maltreatment referral investigation
process:
■ To assess the safety of the child.
■ To take immediate protective actions as necessary.
■ Determine the disposition of the referral.
This process involves the evaluation of all children in a referred family. The interview proto-
col establishes the parties to be interviewed and the children to be evaluated, considering the
essential objectives of the investigation.
Puerto Rico (continued)
Child Maltreatment 2022
Appendix d: State Commentary 263

The data related to any alcohol abuse child risk factor or drug abuse child risk factor can be
collected through data entry in investigation of referrals and case management. The alcohol
abuse and drugs abuse area are collected separate.
Our information system has the option to collect data in both areas, sex trafcking and
prenatal child victims of substance abuse. We have been able to identify them in recent years
as they are correctly documented in our system, perhaps the limitation is in the data entry by
the workers. For this reason, we are directed to emphasize the importance of this information
and what it implies for the child victim.
Fatalities
Puerto Rico works in collaboration with other agencies such as; police and justice department,
forensic sciences for the collection of information on child deaths. Generally, it is the external
agencies that validate child abuse deaths and collaborate with our agency in this area.
In PR, generally, deaths of minors are reported through the direct line even when there is no
suspected allegation of abuse or neglect. In these cases, a social emergency is activated for
due intervention and if an allegation of abuse or neglect is identied, a referral is generated.
Perpetrators
In PR there is no policy as to how young a perpetrator can be. We included the perpetrators
who are other caregivers; staff of institution for children, school, foster care, childcare and
others institution responsibility for the care, education, supervision, and treatment of physical
and emotional needs, as dened by our protection law.
Our system has the capacity to collect data related to sex trafcking, these data are cata-
logued in the typologies, however, our protection law only catalogues situations of sex traf-
cking when the perpetrator is a parent or caregiver, but not a third party or non-caregiver.
Services
Prevention Services
Gender violence prevention services were offered to women and men (of any age) and their
children, through private non-prot organizations and municipalities committed to eradicat-
ing this problem. These services under the Family Violence Prevention and Services Act,
which is legislation that promotes the development of innovative projects aimed at achieving
a better quality of life for victims of gender violence and their children, to prevent family
violence and provide alternative services such as shelters and support for victims and their
dependents, reduce the incidence of deaths from gender violence, and raise community
awareness of the problem of family violence.
The Family and Children’s Administration, through the Auxiliary Administration for
Community Prevention, entered into collaborative agreements with governmental and non-
governmental entities, especially with agencies interested in providing support services to
survivors of domestic violence and their children.
Puerto Rico (continued)
Child Maltreatment 2022
Appendix d: State Commentary 264

At least 95 percent of the funds are granted to nonprot institutions, municipalities and
government agencies that offer services. Additional services with FVPSA funds:
■ Parent cafés: Strategies such as “parent cafés”, which are held weekly on Facebook, allow
us to reach more people. Community cafés are another activity made possible by these
funds, addressing prevention issues and strengthening the leadership of the participants.
■ Individual and/or group support services for women victims or survivors of domestic
violence. FVPSA grants enabled us to provide individual and/or group support services to
women victims or survivors of domestic violence.
■ Psychotherapy support program: This service is designed for victims and their children,
and individual and group psychotherapy for perpetrators. Both programs are operated by a
clinical psychologist with experience in domestic violence issues.
Supplementary funds FVPSA- ARP (COVID 19)
■ The FVPSA Covid-19 grant has allowed for individual counseling in atypical cases, such
as male victims or female victims, with an expert in forensic social work, sexual abuse
assessment and staff trained to provide these services.
■ The FVPSA Covid-19 grants allowed for virtual conferences on topics related to violence
prevention in times of pandemic, impacting the community at large throughout the island.
■ The provision of uninterrupted services to sheltered women and their children in a safe
environment has been completed. Purchase the necessary equipment and materials for risk
mitigation in the face of Covid-19. Provide prevention services to the community from an
equity perspective with trained staff and offer nursing services to all refugees, thus giving
continuity to the coordination of medical services.
■ Provide training for victims and survivors of domestic violence on self-esteem, skills
development and creativity so that they can become economically independent and earn
income to support their families.
■ Virtual services such as educational videoconferences for the community on topics related
to covid-19 and how it affects families suffering from domestic violence and child abuse,
how to prevent it, vaccination and other topics through Facebook Live. Expressive art
workshops were offered at Zoom.
Not all services, only some support services are contracted, for example, for coaching and
training, technical assistance, investigation of referrals in arrears, case management in areas
with larger numbers of families and as complementary support and legal assistance, among
others.
Child removals were not affected. The agency took the necessary precautions. In the case of
removals as a result of a report investigation, the Investigations Units oversaw following the
procedure, including the location of the children. In the case of removals in active agency
cases, each Region had a plan for dealing with these situations through the associate director.
Violencia Familiar (2002PRFVC3) was helpful during the pandemic.
The Administration for Families and Children, Department of Families, delegated funds to
all its community-based organizations for the provision of integrated services to vulnerable
sectors of the country. The primary population served was battered women with their chil-
dren who are victims of child abuse. The American Rescue Plan was another fund received
and used to expand and extend support services to underserved communities.
Puerto Rico (continued)
Child Maltreatment 2022
Appendix d: State Commentary 265

Some support services are contracted, for example, for coaching and training, technical
assistance, investigation of referrals in arrears, case management in areas with larger num-
bers of families and as complementary support and legal assistance, among others.
Puerto Rico (continued)
Child Maltreatment 2022
Appendix d: State Commentary 266

Rhode Island
Contact Leon Saunders Phone 401–528–3850
Title Agency IT Manager
Information Technology
Email
Address RI Department of Children, Youth and Families
101 Friendship St.
Providence, RI 02903
General
In November of 2019, DCYF implemented the SAFE Practice Model across all divisions. In
CPS, the model determines child safety through an assessment of family functioning and
caregiver capacities. The practice shifts from making safety determinations based primarily
on the absence or presence of an incident of maltreatment to an assessment of the needs and
strengths of each family member. Investigations are documented using a Family Functioning
Assessment which addresses specic areas of functioning for all children and their caregiv-
ers. This assessment identies safety threats and protective capacity, creates the basis for
safety plans when appropriate, and identies behavioral changes required to mitigate those
safety threats. For families transferred to on-going Family Service Units, those behavioral
changes formulate the foundation for service plans. Safety is re-assessed throughout the
life of a case through the On-going Family Functioning Assessment which re-assesses the
areas safety addressed by CPS in the Family Functioning Assessment. The model shifts the
practice in our Family Service Units from making decisions about safety and permanency
based on compliance with services to the identication of positive behavioral changes and a
network of informal supports for the family.
Rhode Island does not have two types of response to screened-in referrals. All reports
meeting criteria for a CPS investigation are screened in for investigation. The criteria for an
investigation are:
Investigation Criteria 1- Child Abuse/Neglect (CA/N) Report – RIGL 40-11-3 requires the
Department to immediately investigate reports of child abuse and neglect. The circumstances
reported, if true, must constitute child abuse/neglect as dened by RIGL 40-11-2.
Investigation Criteria 2: Non-Relative Caregiver – RIGL 42-72.1-4 requires that no parent
assigns or otherwise transfers to another, not related to him or her by blood or marriage,
his or her rights or duties with respect to the permanent care and custody of his or her child
under eighteen years of age unless duly authorized by an order or decree of the court.
Investigation Criteria 3: Sexual Abuse of a Child by Another Child – RIGL 40-11-3 requires
the Department to immediately investigate sexual abuse of a child by another child.
Investigation Criteria 4: Duty to Warn – RIGL 42-72-8 allows the Department to release
information if it is determined that there is a risk of physical injury by a person to himself/
herself or others and that disclosure of the records is necessary to reduce that risk. If the
Hotline receives a report that a perpetrator of sexual abuse or serious physical abuse has
access to another child in a family dwelling, that report is classied as an investigation and
assigned for investigation.
Child Maltreatment 2022
Appendix d: State Commentary 267

Investigation Criteria 5: Alert to Area Hospitals, Safety of Unborn Child – RIGL 42-72-8
allows the Department to release information if it is determined that there is a risk of
physical injury by a person to himself/herself or others and that disclosure of the records is
necessary to reduce that risk. The Department issues an alert to area hospitals when a parent
has a history of substantiated child abuse/neglect or a child abuse/neglect conviction and
there is concern about the safety of a child.
Investigation Criteria 6: Serious, Critical Injury, Child Near Fatality or Child Fatality-
Serious, critical injury of a child, near child fatality or Child Fatality. Under RIGL 40-11-3.1
the Department is required to investigate all instances of child fatalities or near fatalities in
which child abuse or neglect is suspected to be a contributing factor regardless of whether the
family is currently active or has ever received services from the Department.
Under RIGL 40-11-3.1 the Department is required to investigate all instances of child fatali-
ties or near fatalities in which child abuse or neglect is suspected to be a contributing factor
regardless of whether the family is currently active or has ever received services from the
Department.
§ 40-11-3.3. Duty to report — Sexual abuse of a child in an educational program.
(a) Any person who has reasonable cause to know or suspect that any child has been the
victim of sexual abuse by an employee, agent, contractor, or volunteer of an educational
program as dened in § 40-11-2 shall, within twenty-four (24) hours, transfer that informa-
tion to the department of children, youth and families, or its agent; provided, however,
that if the person mandated to report is an employee, agent, contractor, or volunteer of an
educational program as dened in § 40-11-2, they shall immediately notify the principal,
headmaster, executive director, or other person in charge of the educational program, or his
or her designated agent. The principal, headmaster, executive director, or other person in
charge of the educational program, or his or her designated agent, shall be responsible for all
subsequent notication to the department of children, youth and families, or its agent in the
manner required by this section. In the case of a public educational program, the principal,
headmaster, executive director, or other person in charge of the educational program, or his
or her designated agent, shall also notify the superintendent of the public educational pro-
gram. Any transferred information shall include the name, title, and contact information for
every employee, agent, contractor, or volunteer of the educational program who is believed to
have direct knowledge of the allegation. Nothing in this section is intended to require more
than one report from any educational program for a specic incident.
(b) To provide guidance and consistency in reporting, the commissioner of elementary and
secondary education shall promulgate policies and procedures for the creation and handling
of reports made by the principal, headmaster, executive director, or other person in charge of
the educational program, or his or her designated agent to carry out the intent of this section.
(c) The department of children, youth and families, or its agent shall immediately forward
the report to state police and local law enforcement and shall initiate an investigation of the
allegations of sexual abuse if it determines that the report meets the criteria for a child pro-
tective services investigation. As a result of those reports and referrals, the department shall
refer those children to appropriate services and support systems to provide for their health
Rhode Island (continued)
Child Maltreatment 2022
Appendix d: State Commentary 268

and welfare. In the event the department substantiates the allegations of sexual abuse against
an employee, agent, contractor, or volunteer of an educational program, the department shall
immediately notify the state police; the local law enforcement agency; the department of
education; the educational program; the person who is the subject of the investigation; and
the parent, or parents, of the child who is alleged to be the victim of the sexual abuse of the
department’s ndings.
Sexually exploits the child in that the person allows, permits, or encourages the child
to engage in prostitution as dened by the provisions in § 11-34.1-1 et seq., entitled
“Commercial Sexual Activity”. “Commercial Sexual Exploitation of Children (CSEC)” refers
to a range of crimes and activities involving the sexual abuse or exploitation of a child for the
nancial benet of any person or in exchange for anything of value (including monetary and
non-monetary benets) given or received by any person.
Reports
The Structured Decision Making tool was implemented in 2019 and staff were re-trained on
the SDM Hot Line Screening Tool in 2022. The Tool guide and automated tool were edited to
include clear language to describe maltreatment types as dened in RI General Law. Under
RI General Laws, anyone who has a reasonable suspicion that a child has been maltreated has
24 hours to make a report to the DCYF CPS Hot Line. The Hot Line is in operation seven
days per week, 24 hours per day and is staffed by Child Protective Investigators. All calls
are recorded, and reporters may remain anonymous. The investigator takes the information
from the reporter and uses the Structured Decision-Making screening tool. Based on the tool,
reports are screened out or assigned for investigation within the designated response priority
times.
Children
Any child who is a household member or was a member of the household at the time of the
alleged maltreatment must be interviewed by a Child Protective Investigator to assess child
safety.
The risk factors involving the use of illicit substances as well as misuse of prescribed and
legal substances are not separated. The screening tool and process does not differenti-
ate between substances, therefore specic risk factors are not associated with different
substances.
Plans of safe care are monitored by the state health department. DCYF is only able to report
this data via comments. The RIDOH reports that for FFY 2022, 425 substance exposed
newborns were identied in KIDSNET. The RIDOH reports receiving 126 plans of safe care
for substance exposure.
Perpetrators
“Other perpetrator” would include any adult who does not have a relationship to the child
listed under the denition of “caretaker.” This would include noncaregiver perpetrators of sex
trafcking.
Rhode Island (continued)
Child Maltreatment 2022
Appendix d: State Commentary 269

Services
Case management is the responsibility of the DCYF caseworker. Most residential and
community-based services are outsourced.
Rhode Island (continued)
Child Maltreatment 2022
Appendix d: State Commentary 270

South Carolina
Contact Lynn Horne Phone 803–394–9737
Title CAPSS Business Analyst Email
Address Division of Technology Services
Department of Social Services
1628 Browning Road, Suite 100
Columbia, SC 29210
General
South Carolina only has one response to screened in reports which is to “Refer for
Investigation.”
Reports
South Carolina implemented a 24/7/365 intake hotline model in November 2021, so FFY
2022 was the rst full year of having a 24/7/365 centralized intake operation. Prior to this
time, each individual county was responsible for receiving on-call referrals outside of the
hours M-F 8:30a-5:00p.
The CPS workforce data are calculated using full-time equivalents (FTEs). Intake case
managers collect information, complete the SDM tool, and make a recommendation. The
intake supervisor reviews the information and makes a nal decision about the disposition of
the intake referral.
Children
The state has a policy to investigate/assess all children in a household if any child in the
household has a maltreatment allegation.
Fatalities
South Carolina Department of Social Services (SCDSS) has a Systems Transformation
Unit that tracks child fatalities internally and keeps data on child fatalities without SCDSS
involvement.
Law enforcement, the coroner, the medical examiner, and the Department of Health and
Environmental Control (Bureau of Vital Statistics Division) report all child deaths that were
not the result of natural causes, to the State Law Enforcement Division (SLED) for an inves-
tigation. SLED investigates all preventable child deaths and then refers their ndings to DSS,
where this unit reviews the agency’s response to these child fatalities.
The State Child Fatality Advisory Committee (SCFAC) also reviews a portion of cases
referred from SLED. As such, SCDSS’s comprehensive systems-level review, including
SCDSS’s records, records collected by SLED, and when available, records collected by
the SCFAC, form the Systems Transformation’s determination that the child fatality was
caused by maltreatment by a person responsible for the child’s welfare or maltreatment by
a person responsible for the child’s welfare contributed to the child fatality for the purposes
of reporting Agency File data. This list is compared to the agency’s SACWIS system and
children whose deaths have been reported in the Child File (indicated by SCDSS for death by
maltreatment) are removed.
Child Maltreatment 2022
Appendix d: State Commentary 271

Fatalities reported on the Agency File include but are not limited to fatalities not investigated
by SCDSS due to the perpetrating person responsible for the child’s welfare also being
deceased and indicated incidents of maltreatment causing a near- and eventual-fatality, but
due to time limits (60 days) on CPS investigations imposed by state statute and the fatality
itself occurring outside this timeframe, the case is not indicated for death by maltreatment in
SCDSS’s CCWIS system.
Perpetrators
Anyone in a “loco parentis” role can have a maltreatment nding and be labeled as a perpe-
trator. South Carolina includes noncaregivers as sex trafcking perpetrators. However, due to
the complexity of criminal cases related to human trafcking, nonparent or caregiver perpe-
trators of human trafcking are named as “Unknown” in our CCWIS system. This is because
if the perpetrator is engaged in a family court case because of the SCDSS involvement and
enters into an Alford Plea, the same plea can be applicable in a criminal trial and can impede
criminal charges and court procedures.
South Carolina (continued)
Child Maltreatment 2022
Appendix d: State Commentary 272

South Dakota
Contact JoLynn Bostrom Phone 605–347–2588 ext. 203
Title Program Specialist
Division of Child Protection Services
Email
Address Department of Social Services
2200 W Main Street
Sturgis, SD 57785
General
Child Protection Services (CPS) does not utilize the Differential Response Model. CPS
either screens in reports, which are assigned as Initial Family Assessments, or the reports are
screened out. However, the Initial Family Assessment allows CPS to open a case for services
based on danger threats without substantiation of an incident of abuse or neglect. South
Dakota does refer reports to other agencies if the report does not meet the requirements for
assignment, and it appears the family could benet from the assistance of another agency.
South Dakota did not change any policies related to conducting investigations and assess-
ments due to the COVID-19 pandemic. The state was not on lockdown and Child Protection
Services continued to serve families throughout the pandemic. Child Protection staff were
considered and deemed as essential staff and were provided with necessary masks and
coverings to ensure their safety and the safety of the families requiring intervention. The
Child Protection intake hotline continued to operate with staff working in the ofce during
the pandemic. Visits that were previously conducted face-to-face were allowed to temporarily
be conducted virtually; however, this was dependent on case specic information.
Reports
CPS child abuse and neglect screening and response processes are based on allegations that
indicate the presence of danger threats, which includes the concern for child maltreatment.
CPS makes screening decisions using the Screening Guideline and Response Assessment.
Assignment is based on child safety and vulnerability. The response decision is related
to whether the information reported indicates present danger, impending danger, or any
other danger threat. A report is screened out if it does not meet the criteria in the Screening
Guideline and Response Assessment as described above.
The reporter types listed as “other” in the NCANDS Child File include clergy, community
person, coroner, domestic violence shelter employee or volunteer, funeral director, other state
agency, public ofcial and tribal ofcial.
Reports of abuse and neglect are categorized into ve types- neglect, physical abuse, sexual
abuse, sex trafcking, and/or emotional maltreatment. Medical neglect is included in the
neglect category.
Children
The data reported in the child le includes children who were victims of substantiated
reports of child abuse and neglect where the perpetrator is the parent, guardian or custodian.
Fatalities
Children who died due to substantiated child abuse and neglect by their parent, guardian or
custodian are reported as child fatalities. The number reported each year are those victims
Child Maltreatment 2022
Appendix d: State Commentary 273

involved in a report disposed during the report period, even if their date of death may have
actually been in the previous year. The State of South Dakota reports child fatalities in the
NCANDS Child File.
South Dakota Codied Law 26-8A-3 mandates which entities are required to report child
abuse and neglect.
“26-8A-3. Persons required to report child abuse or neglected child--Intentional failure as
misdemeanor. Any physician, dentist, doctor of osteopathy, chiropractor, optometrist, emer-
gency medical technician, paramedic, mental health professional or counselor, podiatrist,
psychologist, religious healing practitioner, social worker, hospital intern or resident, parole
or court services ofcer, law enforcement ofcer, teacher, school counselor, school ofcial,
nurse, licensed or registered child welfare provider, employee or volunteer of a domestic
abuse shelter, employee or volunteer of a child advocacy organization or child welfare service
provider, chemical dependency counselor, coroner, or any safety-sensitive position as dened
in § 3-6C-1, who has reasonable cause to suspect that a child under the age of eighteen has
been abused or neglected as dened in § 26-8A-2 shall report that information in accordance
with §§ 26-8A-6, 26-8A-7, and 26-8A-8. Any person who intentionally fails to make the
required report is guilty of a Class 1 misdemeanor. Any person who knows or has reason to
suspect that a child has been abused or neglected as dened in § 26-8A-2 may report that
information as provided in § 26-8A-8.”
South Dakota Codied Law 26-8A-4 mandates that anyone who has reasonable cause to
suspect that a child has died as a result of child abuse or neglect must report. The reporting
process required by SDCL 26-8A-4 stipulates that the report must be made to the medical
examiner or coroner and in turn the medical examiner or coroner must report to the South
Dakota Department of Social Services.
“26-8A-4. Additional persons to report death resulting from abuse or neglect--Intentional
failure as misdemeanor. In addition to the report required under § 26-8A-3, any person who
has reasonable cause to suspect that a child has died as a result of child abuse or neglect as
dened in § 26-8A-2 shall report that information to the medical examiner or coroner. Upon
receipt of the report, the medical examiner or coroner shall cause an investigation to be made
and submit written ndings to the state’s attorney and the Department of Social Services.
Any person required to report under this section who knowingly and intentionally fails to
make a report is guilty of a Class 1 misdemeanor.”
When CPS receives reports of child maltreatment deaths as required under SDCL 26-8A-4
from any source, CPS documents the report in FACIS (SACWIS). Reports that meet the
NCANDS data denition are reported to NCANDS.
The Justice for Children’s Committee (Children’s Justice Act Task Force) is also updated
annually on the handling of suspected child abuse and neglect related fatalities.
South Dakota (continued)
Child Maltreatment 2022
Appendix d: State Commentary 274

Perpetrators
Perpetrators are dened as individuals who abused or neglected a child and are the child’s
parent, guardian or custodian. The state information system designates one perpetrator per
child per allegation.
Services
The Agency File data includes services provided to children and families where funds were
used for primary prevention from the Community Based Family Resource and Support
Grant. This primarily involves individuals who received benet from parenting education
classes or parent aide services.
The State of South Dakota, Division of Child Protection Services with the consent of the
parent, refers every child under the age of 3 involved in a substantiated case of child abuse or
neglect to the Department of Education’s Birth to Three Connections program. This program
is responsible for the IDEA services. The parent or guardian is advised by the Division of
Child Protection Services that with their permission, a referral to Birth to Three Connections
will be made for a developmental screening of their child. The parent or guardian needs to
sign a DSS Information Authorization Form before the referral is made. The parent or guard-
ian is also given a Birth to Three Connections brochure and provided the name of the service
coordinator that will be contacting them to schedule the screening. The Birth to Three
Connections intake form is then completed and faxed with the Information Authorization to
the Birth to Three Connections coordinators to determine eligibility and write an Individual
Family Service Plan for eligible children within 45 days of the receipt of the referral. Not all
children referred by the Division of Child Protection Services to the Birth to Three program
are eligible for services.
South Dakota (continued)
Child Maltreatment 2022
Appendix d: State Commentary 275

Tennessee
Contact Neal Thompson Phone 615–253–1017
Title Business Intelligence Specialist-Intermediate
Strategic Technology Solutions
Finance and Administration
Email
neal.thompson@tn.gov
Address Davy Crockett Tower 2nd Floor
500 James Robertson Parkway
Nashville, TN 37243
General
Tennessee has multiple pathways when screening referrals through CPS. The Multiple
Response System includes Investigations, Assessments (services approach) and Resource
Linkage. Investigations result in an administrative nding of substantiated/unsubstantiated
for allegations of abuse or neglect. Assessments result in a services nding on whether
services where not needed, recommended, required or court ordered to address the concerns
raised to the Department. Resource Linkage involves situations that do not rise to the level of
state denitions of abuse or neglect but where community or material services would prevent
the need for child welfare involvement. All of these tracks are embedded in the SACWIS/
CCWIS system and available to report to NCANDS..
Reports
The state made the following recent hires:
■ FFY 2021: Hotline Case Managers: 57, Hotline Supervisors: 21, Hotline Core Leadership:
5, Readers: 19
■ FFY 2022: Director: 1, Team Coordinators: 4, Team Leaders (all CAH): 9, Supervisory
Case Manager 3 and Trainers for CAH: 13, Reader Program Non-Supervisory Case
Manager 3 19, Case Managers (all CAH): 56
The screening process has not changed in Tennessee from the prior reporting year. Any
change in data would be a direct result in the continued reopening of Tennessee from the
recent pandemic.
Children
Tennessee includes non-familial trafckers as caregivers.
Fatalities
All child fatalities information recorded comes from data received and entered into the
system and are reported in the Child File. Not all infant/child deaths are investigated. DCS
must have jurisdiction due to a report/concern of child maltreatment or if the incident is
unexplained at the time of report, then we will accept the death for investigation. Through
that process, a determination is made whether the death was due to child maltreatment.
Perpetrators
The SACWIS denes almost 70 different ACV to perpetrator roles, where the most selected role is
“Alleged Perpetrator” which is mapped to the NCANDS value= 88 (other). The number reported in
this category has been reduced by more than 15 percent from FFY 2020.
Services
The state outsources some services.
Child Maltreatment 2022
Appendix d: State Commentary 276

Texas
Contact Kevin Chmiel Phone 512–289–4680
Title Data Manager V
Information and Technology
Email
kevin.chmiel@dfps.texas.gov
Address Department of Family and Protective Services
4900 N Lamar Blvd
Austin, TX 78751
General
Alternative Response (AR) is an approach that responds differently than traditional investiga-
tions to reports of abuse/neglect. It allows for a more exible, family engaging approach while
still focusing on the safety of the children as much as in a traditional investigation. Alternative
Response allows screened-in reports of low to moderate risk to be diverted from a traditional
investigation and serviced through an alternative family centered assessment track. There will
be no change in the number or type of clients served but alternative response clients will be
served in a different manner. Generally, the Alternative Response track will serve accepted
child abuse and neglect cases that do not allege serious harm. AR cases will differ from tradi-
tional investigations cases in that there will be no substantiation of allegations, dispositions will
not be used, names of perpetrators will not be entered into the Central Registry (a repository for
conrmed reports of child abuse and neglect), and there will be a heightened focus on guiding
the family to plan for safety in a way that works for them and therefore sustains the safety.
Beginning in November 2014, Alternative Response was initially implemented in Regions 1,
3, and 11 to begin practicing AR and to develop experience and expertise. Implementation
was staggered to allow for planning and training. Regions 7 and 9 were implemented in 2015.
Regions 4, 5 and 10 were implemented in 2017. In 2018, Regions 2, 6b and 8 implemented
Alternative Response. Region 6A was implemented in 2021. At this time Alternative Response
has been fully implemented statewide.
Reports
All reports of maltreatment within DFPS’ jurisdiction are investigated, excluding those
which during the screening process are determined not to warrant an investigation based on
reliable collateral information.
The state considers the start of the investigation to be the point at which the case is assigned
to an investigative caseworker. In some instances, the caseworker will get a report about
a new incident of abuse or neglect involving a family who is already being investigated or
receiving services in an open DFPS case. There are also instances in which caseworkers
begin their investigation when families and children are brought to or walk-into an ofce
or 24-hour shelter. In both situations, the caseworker would then report the maltreatment
incident after the rst face-to-face contact initializing the investigation has been made. The
report date is the date the person calls into SWI. In the narrative they can specify when the
alleged abuse or neglect occur. The date the investigation starts can be 24-72 hours as set by
the priority time frames.
The state’s CPI schema regarding disposition hierarchy differs from NCANDS hierarchy.
The state has “other” and closed-no nding codes as superseding unsubstantiated at the
report level. Texas works on the principle that the two ends of the disposition spectrum are
founded and unfounded with all else in the middle. NCANDS takes a slightly different view
Child Maltreatment 2022
Appendix d: State Commentary 277

that the two sure points are founded and unfounded and everything else is less than either
of these two points. The state’s hierarchy for overall disposition is, from highest to lowest,
RTB-Reason to Believe, UTD-Unable to Determine, R/O-Ruled Out and UTC-Unable to
Complete. Mapping for NCANDS reporting is; RTB=01, UTD=88, UTC=07, and R/O=05.
An inconsistency in the hierarchies for the state and for NCANDS occurs in investigations
where an alleged victim has multiple maltreatment allegations and one has a disposition of
UTD while the other has a maltreatment disposition of R/O. According to the state’s hierar-
chy, the overall disposition for these investigations is UTD. Mapping the report disposition to
unsubstantiated as indicated in the NCANDS’s Report Disposition Hierarchy report would be
inconsistent with state policy.
There is no CPI program requirement or state requirement to capture incident date so there is
no data eld in the SACWIS system for this information. Historical problem: the date when
an abuse/neglect incident happened does not conform to only one date when abuse/neglect is
ongoing. Therefore, identifying one date would be inaccurate.
Children
The State does not make a distinction between substantiated and indicated victims.
A child has the role of “designated victim” when he or she is named as a victim in an allega-
tion that has a disposition of “reason to believe”.
A child (age 10 or older) has the role of “designated perpetrator” when he or she is named as
a perpetrator in an allegation that has a disposition of “reason to believe.”
A child (age 10 or older) has the role of “designated both” (i.e., designated victim and des-
ignated perpetrator in the same case) when he or she is named as a victim in an allegation
that has a disposition of “reason to believe” and as a perpetrator in an allegation that has a
disposition of “reason to believe.”
A person (child or adult) has the role of “unknown (unable to determine)” when he or she is
named in an allegation that has a disposition of “unable to determine” but is not named in
another allegation that has a disposition of “reason to believe”.
A person (child or adult) has the role of “unknown (unable to complete)” when he or she is
named in an allegation that has a disposition of “unable to complete” but is not named in
another allegation that has a disposition of “reason to believe” or “unable to determine”.
A person (child or adult) has the role of “not involved” when: all the allegations in which the
person is named have a disposition of “ruled out”, the overall disposition for the investigation
is “administrative closure”, or the person was not named in an allegation as a perpetrator or
victim.
The State can provide data for living arrangement at the time of the alleged incident of
maltreatment only for children investigated while in a substitute care living situation. All
others are reported as unknown.
Texas (continued)
Child Maltreatment 2022
Appendix d: State Commentary 278

Since FFY 2017, Texas implemented the breakout of Sex Trafcking from the Sexual Abuse
maltreatment type and Labor Trafcking from other maltreatment types Specically for human
trafcking, DFPS investigates if a person traditionally responsible for the children’s care,
custody, and welfare does either of the following:
■ Knowingly causes, permits, encourages, engages in, or allows a child to be trafcked, or
■ Fails to make a reasonable effort to prevent a child from being trafcked
Fatalities
Child fatalities decreased during FFY 2022 by fteen percent.
The source of information used for reporting child maltreatment fatalities is the reason for
death eld contained in the DFPS IMPACT system plus a child fatality investigation with a
reason to believe – fatal nding for an allegation.
DFPS uses information from the State’s vital statistics department, child death review teams,
law enforcement agencies and medical examiners’ ofces when reporting child maltreatment
fatality data to NCANDS. DFPS is the agency required by law to investigate and report on
child maltreatment fatalities in Texas when the perpetrator is a person responsible for the care
of the child. Information from the other agencies/entities listed above is often used to make
reports to DFPS that initiate an investigation into suspected abuse or neglect that may have
led to a child fatality. Also, DFPS uses information gathered by law enforcement and medical
examiners’ ofces to reach dispositions in the child fatalities investigated by DFPS. Other
agencies, however, have different criteria for assessing and evaluating causes of death that may
not be consistent with the child abuse/neglect denitions in the Texas Family Code and/or may
not be interpreted or applied in the same manner as within DFPS.
There were no changes to child fatality reviews during FFY 2022. It is important to note that
starting September 1, 2021, Texas Family Code, Section 261.001 provided an updated denition
for neglect that requires both the presence of blatant disregard as well as either a resulting harm
or an immediate danger: “an act or failure to act by a person responsible for a child’s care,
custody, or welfare evidencing the person’s blatant disregard for the consequences of the act or
failure to act that results in harm to the child or that creates an immediate danger to the child’s
physical health or safety…”
Child fatalities decreased in FFY 2022. This includes signicant decreases in unsafe sleep,
drownings, and vehicle-related fatalities.
Perpetrators
Relationships reported for individuals are based on the person’s relationship to the oldest
alleged victim in the investigation. The State is unable to report the perpetrator’s relationship
to each individual alleged victim, but rather reports data as the perpetrator relates to the oldest
alleged victim. Currently the State’s relationship code for foster parents does not distinguish
between relative/non relative.
The state only reports on human trafcking perpetrators who meet the Texas Family Code §
261.001(5)(A)-(D) denition of a person responsible for a child’s care, custody, and welfare.
Texas (continued)
Child Maltreatment 2022
Appendix d: State Commentary 279

Services
In FFY 20 DFPS made changes to the policy handbook to align with Federal Plans of Safe Care
guidance. Staff work with the hospitals to ensure that a Plan of Safe Care has been initiated for
families in cases involving prenatal substance exposure. Child Protective Investigation (CPI)
and Child Protective Services (CPS) staff work to ensure that any plans developed for a family
are individualized to address the family’s particular strengths and needs and to ensure that
any appropriate referrals are made. DFPS continues to work with both the local and state level
with appropriate community stakeholders and partner agencies to develop consistent guidance
around Plans of Safe Care.
Texas (continued)
Child Maltreatment 2022
Appendix d: State Commentary 280

Utah
Contact Jennifer Larson Phone 801–538–4100
Title Electronic Business Project Manager/CCWIS Director Email
Address Division of Child and Family Services
195 N 1950 W
Salt Lake City, UT 84116
General
Utah continues to invest in its child welfare programs, both through improved training for
caseworkers and updating the technology that enables those workers. Utah continues to
navigate COVID and the impact on children, families, mandatory reports, and the workforce.
Utah has seen the high caseworker turnover and addressing the impact in training and
mentoring. Overall workforce support is Utah’s top priority.
Utah does not have an alternative response/differential response. All reports are either
screened out or screened in as a referral for a CPS Assessment.
Reports
The investigation start date is dened as the date a child is rst seen by CPS. The data is
captured in date, hours, and minutes. A referral is screened out in situations including, but
not limited to:
■ The minimum required information for accepting a referral is not available.
■ As a result of research, the information is found not credible or reliable.
■ The specic incidence or allegation has been previously investigated and no new informa-
tion is gathered.
■ If all the information provided by the referent were found to be true and the case nding
would still be unsupported.
■ The specic allegation is under investigation and no new information is gathered.
The state uses the following ndings:
■ Supported–a nding, based on the information available to the worker at the end of the
investigation, that there is a reasonable basis to conclude that abuse, neglect, or depen-
dency occurred, and that the identied perpetrator is responsible.
■ Unsupported–a nding based on the information available to the worker at the end of
the investigation that there was insufcient information to conclude that abuse, neglect,
or dependency occurred. A nding of unsupported means that the worker was unable to
make a positive determination that the allegation was actually without merit.
■ Without merit–an afrmative nding at the completion of the investigation that the alleged
abuse, neglect, or dependency did not occur, or that the alleged perpetrator was not
responsible.
■ Unable to locate–a category indicating that even though the child and family services
child protective services worker has followed the steps outlined in child and family
services practice guideline and has made reasonable efforts, the child and family services
child protective services worker has been unable to make face-to-face contact with the
alleged victims to investigate an allegation of abuse, neglect, or dependency and to make a
determination of whether the allegation should be classied as supported, non-supported,
or without merit.
Child Maltreatment 2022
Appendix d: State Commentary 281

Children
Utah’s predominant allegation continues to be neglect. When combined with a family’s risk
factors, neglect is often the result of substance misuse. Utah continues to investigate out-of-
home perpetrators which results in higher than the national average of sexual abuse cases.
Utah has a process which defers pregnant women who are identied as substance using to the
Ofce of Substance Abuse and Mental Health for treatment and services as a preventative
measure to DCFS involvement.
Fatalities
Concerns related to child maltreatment, including fatalities, are required to be reported to the
Utah DCFS. Fatalities where the CPS investigation determined the abuse was due to abuse
or neglect are reported in the NCANDS Child File. No changes to the fatality review process
were made in FFY 2022.
Perpetrators
The only restriction Utah places upon identifying perpetrators is that CPS will not open
a case for sexual abuse where the perpetrator is under the age of 12, except in extreme
circumstances. This change was a result from HB262 during the 2020 session of the Utah
legislature. Utah does report noncaregiver perpetrators of sex trafcking.
Services
There has been no changes to Utah’s prevention funding. Utah continues to explore other pre-
vention services as related to Family First Prevention Services Act (FFPSA). Utah does not
outsource case management responsibilities, but does outsource services where appropriate.
Utah (continued)
Child Maltreatment 2022
Appendix d: State Commentary 282

Vermont
Contact Melissa Burt Phone 802–241–0879
Title Quality Assurance Coordinator
Vermont Family Services Division
Email
Address Vermont Department for Children and Families
280 State Dr HC1 North Bldg B
Waterbury, VT 05671
General
Over the past 10 years, about 35 percent of cases are assigned to the assessment track. In the
assessment track, the disposition options are services needed and no services needed. Cases
assigned to the assessment track may be switched to the investigation track, but not vice
versa. Data from both tracks are reported to NCANDS. Vermont’s Family Services Division
(FSD) is responsible for responding to allegations of child abuse and neglect by parents or
“persons responsible for the child’s welfare”, and sexual abuse by any person (including out-
of-home perpetrators). In addition to conducting our statutory child abuse investigations and
assessments, we also have an option to conduct family assessments under the authority of 33
V.S.A.§ 5106. These family assessments do not meet statutory requirements for abuse and
neglect but provide an option to engage with families where there are concerns. The focus of
the assessment is on whether a child may be in need of care or supervision and are referred
to as CHINS assessments. Because these family assessments are not part of our abuse and
neglect statute, they are not reected in this dataset. However, it is important to acknowledge
that on an annual basis we conduct approximately 1,000 family assessments.
Reports
Vermont operates a statewide child protection hotline, available 24/7. All intakes are handled
by family services workers and screening decisions are handled by hotline supervisors. These
same supervisors make the initial track assignment decision. Vermont’s CPS workforce data
is calculated using full-time equivalents and has experienced some uctuation in capacity
since the COVID-19 pandemic. Some of the changes seen can be attributed to the reduction
in the workforce itself, seen nationwide, as well as a reduction in the number of accepted
child safety interventions since the pandemic. Vermont is beginning to see an increase in the
number of reports made to the child protection hotline, approaching pre-pandemic volumes,
and feels that this may be attributed to society’s acceptance of the virus, and continued
efforts to gain normalcy in a post-pandemic environment. Additionally, it should be noted
that some of the increase seen in Vermont’s FFY 2022 reporting period is a result of the IT
Developer adjusting the coding to include 11 additional types of sexual abuse tracked within
the database, including incest, rape, sodomy, lewd and lascivious, aiding child pornography,
viewing child pornography, voyeurism, luring, obscenity and sexual assault.
All calls to the child abuse hotline are counted as referrals, resulting in a very high rate of
referrals per 1,000 children, and making it appear that Vermont has a very low screen-in
rate. Although Vermont has not conducted a thorough analysis, some of the contributing
factors leading to our increasing number of referrals include, but are not limited to, reports
where child abuse/neglect are not present and issues include truancy, delinquent behavior,
mental health crises, out-of-home sexual abuse reports including teen sexting with or without
consent, teen sexual harassment, as well as family conguration and our practice of entering
reports under the primary caretaker when there are multiple children involved. This often
Child Maltreatment 2022
Appendix d: State Commentary 283

results in multiple reports for the same incident. In situations where multiple reports are
made for the same incident, it is Vermont’s practice to screen in only one of those reports.
Vermont continues to utilize the SDM Safety Assessment and Risk Assessment tools in our
child safety interventions. In 2022, we added language into the Safety Assessment to better
capture human trafcking as a danger item and we shifted our practice to truly give families
a choice in whether they engage in prevention-based services with the Division.
Children
The Family Services Division is responsible for investigating allegations of child abuse or
neglect by caregivers and sexual abuse by any person. The Division investigates risk of
physical harm and risk of sexual abuse. Statute allows the Division to identify other children
living in the same home as the identied child victim, and states that the investigator shall
consider the physical and emotional condition of those children and may interview them,
unless the child is the person who is alleged to be responsible for such abuse or neglect.
Unless unreasonable within the context of the child safety intervention, division policy
requires staff to evaluate the safety of any other children living in the same home. The evalu-
ation should include an interview or observation of the other child(ren) and occurs with the
permission of the child’s parent, guardian or custodian.
Vermont faces a few challenges regarding collecting and reporting data to NCANDS for
some data elements, including child and caregiver risk factors, and infants with prenatal
substance exposure. We will continue to have limitations until the state can successfully
implement a new CCWIS system. Until that time we continue to make system enhancements
to our legacy system when IT resources are available. This work needs to be prioritized
against other department wide initiates, resulting in a substantial lag time for the work to
be complete. As an example of a system limitation regarding prenatal substance exposure,
when child protection services (CPS) or Family Services (FSD) are not involved, meaning
the child does not meet the criteria for making a report to the child abuse and neglect hotline,
we are currently relying on hospital staff to remember to fax a notication to us at FSD.
This information is then tracked in an Excel spreadsheet. Vermont has considered making
enhancements to the state’s database where our centralized intake data lives to better track
this data; however, the state continues to lack IT resources to move this work forward.
Another option that has been considered for this tracking is an external web-based portal that
could be utilized by all hospitals in the state and reported to FSD. Vermont participated in
the 2023 Policy Academy: Advancing Collaborative Practice and Policy: Promoting Healthy
Development and Family Recovery for Infants, Children, Parents, and Caregivers Affected
by Prenatal Substance Exposure, and we have since applied for and been accepted to receive
In Depth Technical Assistance (IDTA) from Children and Family Futures, which is now
underway. Through this collaborative process, we will continue to revisit our approach to
supporting families affected by substance use disorders and substance-exposed newborns.
Related to data collection, one of our goals within this work is to improve data collection as
a strategy to apply quality improvement methods in clinical and community care towards the
goal of increased care coordination a systems integration, including:
1. Understand number of infants born affected by substance use who needed a POSC
2. Explore development of portal to collect notication data
3. Expand use of CAPTA ow sheet in electronic health records (EHRs) across the state
Vermont (continued)
Child Maltreatment 2022
Appendix d: State Commentary 284

4. Subgroup (PLSB Workgroup) continue to meet to address data concerns
5. Determine where redcap database/portal data will live
6. Implement data collection measures as possible within CHARM teams
When CPS/FSD are involved due to safety issues, our current antiquated data system has
many limitations and we currently are not able to capture all cases that would fall into this
category, therefore we are under-reporting. Vermont did not change any polices or proce-
dures regarding reporting or tracking of infants with prenatal substance exposure during the
pandemic.
One system enhancement that Vermont was able to successfully implement was having sex
trafcking report as its own maltreatment type. Vermont has been collecting this data for
years, however, with reduced IT resources and the need for the work to be prioritized, FFY
2022 submission is the rst reporting period that includes the updated mapping. Sex trafck-
ing as a maltreatment type is captured as such for the entire FFY.
Fatalities
DCF FSD is part of Vermont’s Child Fatality Review Team (CFRT), which is housed under
the Vermont Department of Health (VDH). This team reviews all unnatural child fatalities
and provides annual data to the legislature, striving to make recommendations related to
themes which arise.
DCF FSD is a member of the National Partnership for Child Safety, which is now a 26-juris-
diction collaborative with support from Casey Family Programs. As part of our collaboration
with NPCS, Vermont is in the process of developing the Safe System Learning Review
(SSLR); a child death review process which utilizes the Safe Systems Improvement Tool
(SSIT) and seeks to create a psychologically safe process for staff as well as one that pro-
motes system wide improvement over individually based fault nding.
Perpetrators
Division policy denes a perpetrator as an individual of any age who is determined to
have committed child abuse or neglect. Perpetrators of sexual abuse include non-caregiver
perpetrators of any age. Perpetrators of all other types of abuse must be a person responsible
for the child’s welfare (includes the child’s parent; guardian; foster parent; any other adult
residing in the child’s home who serves in a parental role; an employee of a public or private
residential home, institution or agency; or other person responsible for the child’s welfare
while in a residential, educational, or child care setting, including any staff person (33 V.S.A.
§ 4912(10)). Young people may be identied as a perpetrator of sexual abuse on another youth
as young as age 6 (referred to as alleged actor youth); however, according to our differential
response track assignment, those allegations would be assigned as an assessment up until age
14, at which point the case would be assigned as an investigation. Perpetrators that fall into
the “other” relationship category for the purposes of NCANDS reporting include stepparent,
foster sibling, and grandparent. In addition, any perpetrator that is captured using the stand-
alone code of OO (other relationship) within the database will fall into this category. Vermont
does report non-caregiver perpetrators of sex trafcking to NCANDS.
Vermont (continued)
Child Maltreatment 2022
Appendix d: State Commentary 285

Services
Within the last year, as mentioned earlier, Vermont undertook practice changes related to our
use of the SDM Risk Assessment and determination of service need to truly give families
a choice in whether they engage in prevention-based services with the division. Following
an investigation or assessment, a validated risk assessment tool is applied. If the family is
classied as at high- or very-high-risk for future child maltreatment, the family is offered
in-home services, and may be referred to other community services designed to address risk
factors and build protective capacities. State statute dictates that families have the option of
declining services offered as a result of the division’s assessment. Prior to case closure, staff
should be assisting the family in making referrals and connections to community providers,
and having a conversation with the family about why they are declining services and how
they plan to partner with family, friends, and/or services providers in their local community
to mitigate the risks. We’ve referred to these conversations or meetings as “Safe Closure
Meetings”, where we support families in developing their own plan.
Vermont chose two evidence-based practices to implement in year 1 of our 5-Year Prevention
Plan. We decided to start with a small number of EBPs in the rst year to support a success-
ful implementation and reliable CQI processes. Each of these practices have at least a small
foothold in Vermont. Because these practices are already known and have been adopted as
benecial interventions by our greater system, there was a lot of support from our stakehold-
ers for these practices. Additionally, these practices have high efcacy ratings, which also
enhanced support for them. Vermont’s two selected EBPs are Motivational Interviewing (MI)
and Child Parent Interactive Therapy (PCIT). Specic to MI, contracts have been amended
for Intensive Family Based Services (IFBS) and Balanced and Restorative Justice (BARJ).
We are partnering closely with the Department of Mental Health (DMH) regarding PCIT.
We are planning to begin by providing preventive services to candidates involved with the
division through open Family Support Cases and Conditional Custody Orders (CCOs). Over
time, our vision is to collaborate with and support our key community stakeholders so that
in the future, the funding would follow the child/youth/family regardless of the division’s
involvement or case status. This will mean that their needs can be met without ever having to
enter the child welfare system. We also recognize the need to expand our array of prevention-
based services over time.
Vermont (continued)
Child Maltreatment 2022
Appendix d: State Commentary 286

Virginia
Contact Shannon Hartung Phone 804–629–7125
Title Protection Program Manager
Division of Family Services
Email
Address Virginia Department of Social Services
801 East Main Street, 11th Floor
Richmond, VA 23219
General
There were not any substantial changes to the Code of Virginia in 2022. Section 63.2-1504 of
the Code of Virginia provides Virginia with a differential response system. The differential
response system allows local departments to respond to valid reports or complaints of child
abuse or neglect by conducting either an investigation or a family assessment. Virginia reports
data from both pathways to NCANDS.
The Virginia Administrative Code 22VAC40-705-10 denes Family assessment as the collec-
tion of information necessary to determine:
1. The immediate safety needs of the child;
2. The protective and rehabilitative services needs of the child and family that will deter abuse
or neglect;
3. Risk of future harm to the child; and
4. Alternative plans for the child’s safety if protective and rehabilitative services are indicated
and the family is unable or unwilling to participate in services. These arrangements may be
made in consultation with the caretaker of the child.
The Virginia Administrative Code 22VAC40-705-10 denes “Investigation” as the collection of
information to determine:
1. The immediate safety needs of the child;
2. The protective and rehabilitative services needs of the child and family that will deter abuse
or neglect;
3. Risk of future harm to the child;
4. Alternative plans for the child’s safety if protective and rehabilitative services are indicated
and the family is unable or unwilling to participate in services;
5. Whether or not abuse or neglect has occurred;
6. If abuse or neglect has occurred, who abused or neglected the child; and
7. A nding of either founded or unfounded based on the facts collected during the
investigation.
Reports
CPS referrals increased from FFY 2021 to FFY 2022. However, the rate of referrals being
accepted decreased over this same period. Additionally, the rate of Family Assessments being
completed over investigations remained consistent with FFY 2021. The increase in referrals is
likely due to the end of COVID-19 restrictions and a statewide return to in-person learning for
students in public school settings.
As a state supervised locally administered system, referral validity is determined by the local
department of jurisdiction. Local departments assess the validity criteria of age, caretaker,
and jurisdiction and are required to use the Structured Decision Making (SDM) Intake Tool to
determine if the allegations meet a denition of abuse or neglect. The SDM Intake Tool is also
Child Maltreatment 2022
Appendix d: State Commentary 287

used to determine the referral track (family assessment or investigation) and response priority
(R1, R2, or R3). The SDM Intake Tool used by Virginia was revised in August 2020.
Children
Child victims increased slightly from FFY 2021 to FFY 2022. Virginia does not include all
children in the household as victims. To be identied as a victim, the child must be directly
associated with a maltreatment allegation.
Virginia captures alcohol and drug child risk factors; however, when both risk factors are
indicated the system only reports one risk factor. There have been no changes in the methodolo-
gies of our reporting from FFY 2021 to FFY 2022 for sex trafcking victims and infants with
prenatal substance exposure.
Fatalities
Virginia investigated less child fatalities in FFY 2022. The number of unique child fatalities
decreased from FFY 2021 to FFY 2022, likely due to the high number of child fatalities involv-
ing unsafe sleep environments that are often unsubstantiated. Virginia does not collect child
fatality data from external agencies. Virginia only investigates infant and child deaths when
there is a child maltreatment allegation.
Virginia did not make any policy related changes to the child fatality review process; however,
we signicantly revised our guidance around the investigation of child deaths. Virginia con-
tinues to prepare an annual report on child deaths investigated for abuse or neglect across the
Commonwealth.
Perpetrators
The number of perpetrators decreased. In Virginia, any individual who is in a caretaking role of
a child can be identied as a perpetrator of abuse or neglect, this includes individuals under the
age of eighteen. Consideration is given to the amount of authority delegated to the individual
for the care, control, and discipline of the child. Virginia reports non caretaker perpetrators of
sex trafcking to NCANDS.
Section 63.2-1509 of the Code of Virginia says:
B. A valid report or complaint regarding a child who has been identied as a victim
of sex trafcking or severe forms of trafcking as dened in the federal Trafcking
Victims Protection Act of 2000 (22 U.S.C § 7102 et seq.) and in the federal Justice
for Victims of Trafcking Act of 2015 (P.L. 114-22) may be established if the alleged
abuser is the alleged victim child’s parent, other caretaker, or any other person
suspected to have caused such abuse or neglect.
Services
Virginia implemented Family First on July 1, 2021. This implementation included the alignment
of Prevention, CPS Ongoing, and Family First to create In-Home Services, and the utilization
of IV-E Prevention Services funding for evidence-based programs (EBPs). Virginia began with
three EBPs – Multisystemic Therapy (MST), Functional Family Therapy (FFT), and Parent-
Child Interaction Therapy (PCIT). LDSS began utilizing IV-E Prevention Services funding in
the rst few months of implementation. As so December 1, 2021, all three of these EBPs were
Virginia (continued)
Child Maltreatment 2022
Appendix d: State Commentary 288

also Medicaid eligible, resulting in a decrease in IV-E spending. The Center for Evidence-
based Partnerships in Virginia (CEP-Va) completed and submitted a Needs Assessment and
Gaps Analysis (NAGA) report to VDSS in October 2021, which included the recommendation
for the addition of EBPs in Virginia’s Prevention Plan. Virginia is in the process of getting
approval for ve additional EBPs – Brief Strategic Family Therapy (BSFT), Family Check-Up,
Homebuilders (HB), Motivational Interviewing (MI), and High Fidelity Wraparound (HFW).
None of these EBPs are currently covered under Virginia Medicaid, so the expectation is that
IV-E utilization will increase during FFY 2024.
Virginia has utilized Transition Act funds to expand the availability of EBPs across the state.
Despite the availability of funds, due to the mental healthcare workforce stafng crisis the
ability of providers to bring new EBPs (or sustain current EBPs) has been a major challenge to
expansion efforts. CEP-Va began a second round of NAGA in the spring of 2022 which takes
this into consideration. Their report and recommendations will be submitted to VDSS in early
2023.
The 2022 Special Session of the Virginia General Assembly authorized a change in funding
source for the Relative Maintenance Support Payments for eligible relatives and ctive kin
from Temporary Assistance for Needy Families (TANF) federal block funds to 100 percent
state general funds. The Relative Maintenance Support Payment aligns with the Virginia
Department of Social Services (VDSS) Kin-First culture and is a state supported approach to
providing needed nancial assistance and promotes concerted efforts that honors and maintains
family connections. This appropriation of general funds presented VDSS with the opportunity
to provide support payments for children who do not meet the TANF child-only require-
ments and are being cared for by ctive kin to avoid placement into foster care. This support
payment was incorporated into the Virginia Case Management System (VaCMS) to manage
and disperse payments with payments to eligible relative and ctive kin caregivers begin-
ning December 19, 2022. In SFY 2022, 652 families received Relative Maintenance Support
Payments.
Virginia continues to value and support usage of PSSF funds for preventive services. There has
been a targeted focus on the technical assistance provided to local agencies to increase the use
of PSSF funds to ensure children and families receive appropriate and necessary wrap-around
services and/ or that PSSF funds be used to complement other funding streams to ensure
there are no gaps in services when working with families. Another targeted focus has been to
increase the use of PSSF funds to provide supportive services to relatives and ctive kin caring
for children as a result of CPS involvement to reduce the risk of entry or re-entry into foster
care.
For SFY 2022, in comparison to SFY2021, there was a 38 percent increase in the use of Family
Support funds, a 55 percent increase in the use of Family Preservation funds, 49 percent
increase in the use of Family Reunication funds and a 282 percent increase in the use of
Monthly Caseworker Visits funds. In the same year, 898 relatives received supportive services
through PSSF funds. The primary services being housing/ material assistance, case manage-
ment, information and referrals, parent-family resource center, assessments, transportation,
parenting education and counseling services.
Virginia (continued)
Child Maltreatment 2022
Appendix d: State Commentary 289

Virginia accessed and used PSSF COVID funds. All COVID funds were exhausted and used
to provide supportive services to 1,676 families, 2,636 children and 209 relatives. The primary
services being housing/ material assistance, transportation, parent education, assessments,
educational supports, home based services, and childcare.
Virginia (continued)
Child Maltreatment 2022
Appendix d: State Commentary 290

Washington
Contact Lisa Barber Phone 360–407–1461
Title Report Design/Development
Ofce of Innovation, Alignment, and Accountability
Email
Address WA State Department of Children, Youth, and Families
1500 Jefferson Street
Olympia, WA 98504
General
A Structured Decision Making (SDM) intake screening tool supports a two pathway response
for CPS response when there were allegations of child abuse and neglect (CA/N) and clear
denitions for CPS risk-only intakes.
CPS risk-only intakes involve a child whose circumstances places him or her at imminent
risk of serious harm without any specic allegations of abuse or neglect. When CPS risk-only
intakes are screened in, children must be seen by a CPS investigator within 24 hours and a
complete investigation is required. If child abuse or neglect is found during the response to a
CPS risk-only intake, a new CPS intake is created regarding the allegation, the case worker
records the ndings and the record is included in the NCANDS Child File. CPS risk-only
intakes were not historically submitted to NCANDS because of no substantiation of mal-
treatment. However, because CPS Risk-Only intakes receive a full investigation it has been
requested that they be included to provide an accurate reection of the number of CPS cases
being investigated and assessed. CPS Risk-Only intakes are now included as of the FFY 2019
report. Historical counts of CPS Risk-Only intakes were provided in each year’s commentary.
Washington’s Children’s Administration (CA) uses a two pathway response for CPS intakes:
investigation which requires a 24- or 72-hour response time, and FAR, requiring a 72-hour
response. Intakes screened to FAR predominately contain allegations for physical abuse and
neglect that were and still are considered low risk, not requiring an immediate response.
The SDM provides consistency in screening, and it guides intakes with neglect allegations
considered low risk to the FAR pathway. Intakes involving cases that have had three or more
screened in CPS intakes within the last 12 months or allegations of moderate to severe physical
abuse and all sexual abuse allegations are screened to the investigation pathway. Intakes with
any allegations of physical abuse for children under age 4, with a dependency within the last 12
months or an active dependency are screened to investigation. This two pathway response has
been phased-in across the state as of June 2017.
Reports
To be screened-in for CPS intervention, intakes must meet sufciency. Washington’s suf-
ciency screening consists of three criteria:
■ Allegations must meet the Washington Administrative Code (WAC) for child abuse and
neglect.
■ The alleged victim of child abuse and neglect must be younger than 18 years.
■ The alleged subject of child abuse or neglect has a role of parent, acting in loco parentis, or
unknown.
Intakes that do not meet all three of the above criteria do not screen in for a CPS response,
unless there is imminent risk of harm (CPS risk-only) to the child. Intakes that allege a crime
has been committed but do not meet Washington’s screening criteria are referred to the law
Child Maltreatment 2022
Appendix d: State Commentary 291

enforcement jurisdiction where the alleged crime occurred. CPS Risk Only intakes receive an
Investigation with a 24 or 72-hour response, when protective factors are in place mitigating the
imminent risk of harm to the child for the 72 hours following the intake (e.g. hospitalization).
Intakes screened to the FAR pathway do not receive a CPS nding. Additionally, FAR intakes
are mapped as alternative response non-victim in NCANDS and don’t receive ndings on alle-
gations. In FFY 2015, there was a signicant increase in intakes screened to the FAR pathway
from FFY 2014, thus eliminating a large pool of victims receiving a nding. The increase in
the number of intakes screened to the FAR pathway in FFY 2015 is a result of the staggered
implementation of the FAR pathway across the state. In FFY 2016 there was a similar increase
in intakes screened to the FAR pathway from FFY 2015 as a result of additional ofces imple-
menting FAR and due to additional training and consultation on the SDM intake screening tool
and FAR pathway. Prior to full implementation of FAR, for ofces that had not launched FAR,
intakes screened to FAR through the use of the SDM were diverted back to an investigation
pathway, allowed under the Washington state statute. Since the full implementation of FAR
statewide, the number of intakes screened to the FAR pathway have continued to increase
which resulted in a reduction of cases that involved a victim and subject.
During FFYs 2014–2016 there was a signicant increase noted for 24-hour emergent intakes,
both with allegations of CA/N and CPS risk only. Also during FFYs 2014–2015, there was
an enhanced focus on child safety related to children age 0–3. A new intake policy was
implemented requiring that screened-in physical abuse intakes regarding children 0–3 would
be investigated, and children would be seen within 24 hours. In FFY 2017 there was again an
increase in CPS Risk Only and 24-hour emergent intakes.
The Licensing Division (LD), formally known as the Department of Licensed Resources
(DLR), complete DLR-CPS risk-only intakes alleging, abuse or neglect of 18–21 year olds in
facilities licensed or certied to care for children require a complete investigation. If, during
the course of the investigation, it is determined that a child younger than 18 was also alleg-
edly abused by the same perpetrator, the investigation would then meet the criteria for a CPS
investigation rather than a CPS risk-only investigation. A victim and ndings will be recorded,
and the record will be included in the NCANDS Child File. For intakes containing child abuse
and neglect allegations, response times of 24 hours or 72 hours are determined based on the
sufciency screen and the SDM intake screening tool.
Children
An alleged victim is reported as substantiated if any of the alleged child abuse or neglect was
founded. The alleged victim is reported as unsubstantiated if all alleged child abuse or neglect
identied was unfounded. The NCANDS category of “other” disposition previously included
the number of children in inconclusive investigations. Legislative changes resulted in inconclu-
sive no longer being a ndings category. The NCANDS category of neglect includes medical
neglect.
Fatalities
The state includes child fatalities that were determined to be the result of abuse or neglect by
a medical examiner or coroner or if there was a CPS nding of abuse or neglect. The state
previously counted only those child fatalities where the medical examiner or coroner ruled
Washington (continued)
Child Maltreatment 2022
Appendix d: State Commentary 292

the manner of death was a homicide. Washington only reports fatalities in the Agency File.
Information about fatalities is also requested from the County Coroner’s/Medical Examiner’s
Ofces, Law Enforcement departments, and the Washington State Department of Health,
which maintains vital statistics data, including child deaths.
Children’s Administration (CA), now Dept of Children, Youth and Families (DCYF), began
maintaining a separate database of child fatality data (AIRS) in 2002. At that time the CAMIS
system used before the SACWIS system was implemented. CAMIS did not support a database
of child fatality and other critical incident information. In February 2009, CA released a new
SACWIS system (FamLink). The objective was to have all child fatality and other critical
incident information stored in FamLink and the reporting of all critical incidents would be done
through FamLink. However, this plan was cancelled due to budgetary considerations. FamLink
does identify child fatalities and other critical incidents, but it does not include the level of
detail necessary to determine whether the fatality was the result of abuse and neglect. This
information continues to be maintained in the AIRS database and reported in the Agency File.
Washington has seen a signicant increase in the numbers of fentanyl and opioid related
fatalities. In the FFY21 data, fentanyl and opioid overdose/ingestion deaths accounted for
.08% of the child fatalities that year. In FFY 2022, fentanyl and opioid overdose/ingestion
deaths accounted for 23 percent of the child fatalities. In 2021, 28 percent of the fatality and
near fatalities that qualied for a review were the result of fentanyl and opioid overdose/inges-
tion. In 2022, 44 percent of the fatality and near fatalities that qualied for a review were the
result of fentanyl and opioid overdose/ingestion. These are signicant increases from previous
years. Note: per state law, DCYF is required to conduct child fatality and near fatality reviews
when the child’s death or near fatal injury is the result of abuse or neglect and the department
provided services to the child within 12 months of the fatal or near fatal injury. In FFY 2022,
DCYF had no prior contact, or no recent contact, with the families in 55 percent of the child
fatalities. This is also reected in the cases that qualify for fatality and near fatality reviews.
Perpetrators
The perpetrator relationship value of residential facility provider/staff is currently mapped to
the NCANDS category of “other” perpetrator relationship. The NCANDS category of “other”
perpetrator relationship includes the state categories of other and babysitter.
The parental type relationship is a combined parent birth/adoptive value. Because the
NCANDS eld separates biological and adoptive parent and Washington’s system does not
distinguish between the two, parent birth/adoptive is mapped to the NCANDS category of
unknown parent relationship.
Washington does not report noncaregiver perpetrators of sex trafcking. These are screened out
as a third party report to law enforcement.
Services
Families receive preventive and remedial services from the following sources: community-
based services such as public health nurses, infant mental health, early intervention, Head Start
and other early learning programs, the Parent-Child Assistance Program, and referrals for
mental health, domestic violence, and/or substance use disorder treatment. Contracted services,
Washington (continued)
Child Maltreatment 2022
Appendix d: State Commentary 293

including several evidence-based practices such as Homebuilders, Incredible Years, Safe Care,
Triple P, Parent-Child Interaction Therapy, and Promoting First Relationships. Families can also
receive CPS childcare, family reconciliation services, family preservation, and intensive family
preservation services. The number of recipients of the community-based family resource and
support grant is obtained from community-based child abuse prevention (CBCAP). Service
provision has been negatively impacted by the pandemic with many service providers under-
staffed and/or unable to see families in-person. Some service providers have successfully
transitioned to virtual delivery of services.
Washington (continued)
Child Maltreatment 2022
Appendix d: State Commentary 294

West Virginia
Contact Stephanie Lindley Phone 304–558–5864
Title Program Manager Email
stephanie.l.lindley@wv.gov
Address Ofce of Management Information Systems
WV Department of Health and Human Resources
One Davis Square, Suite 200
Charleston, WV 25301
General
West Virginia currently has only one response, accepted for assessment.
Report
The number of referrals in FFY 2022 was very similar to FFY 2021. The Hotline continued
to operate 24/7. Stafng level was impacted by resignations and vacancies. Due to continu-
ous staff turnover, WV is always hiring and training new staff. The CPS workforce data is
calculated using full-time equivalents (FTEs). During screening, a supervisor will review all
the information in the report to determine whether there is reasonable cause to suspect a child
is abused or neglected. The supervisor will use the legal and operational denitions to make the
decision. CPS must accept for assessment any report which suggests that an individual between
birth and eighteen years of age may have been subject to treatment which meets the denition
of abuse or neglect in WV Code and CPS Policy. Once accepted, the intake is transferred to the
district for assignment to a CPS worker. Intakes that do not meet the legal denition of abuse or
neglect are screened out. The intake is peer reviewed the following day by a Centralized Intake
(CI) CPS supervisor to ensure the accuracy of the original screening decision.
Children
West Virginia investigates/assesses all children in a household if any child in the household has
a maltreatment allegation. West Virginia began reporting sex trafcking data in FFY 2018.
Fatalities
Fatality information is collected by the Title IVE agency within the Ofce of the Chief Medical
Examiner. If there is no allegation that the child’s death or near death was due to maltreatment
or concerns of existing safety threats, CI screens those out.
Perpetrators
A maltreater must be 18 years old or a parenting youth under the age of 18. The NCANDS
category of “other” perpetrator relationship includes the state categories of non-guardian,
household members and out of household perpetrators regarding trafcking. Noncaregiver
perpetrators of sex trafcking are reported to NCANDS.
Services
All services in West Virginia are outsourced.
Child Maltreatment 2022
Appendix d: State Commentary 295

Wisconsin
Contact Wendy Henderson Phone 608–422–6989
Title Division of Safety and Permanence Email
wendy[email protected]
Address Wisconsin Department of Children and Families
201 West Washington Avenue
Madison, WI 53703
General
There were no signicant state policy changes that affect the data submission. Certain counties
in Wisconsin have implemented the Alternative Response (AR) approach. The maltreatment
disposition for AR assessments identies whether services are needed and will appear in
NCANDS as alternative response nonvictim dispositions.
Reports
The state data are child-based, with each report associated with a single child. The report date
is the date when the agency was notied of the alleged maltreatment, and the investigation start
date is the date when the agency made initial contact with the child or other family member. In
Wisconsin’s child protective services (CPS) system, multiple maltreatment reports for a single
child may be assessed during a single investigation.
There are a variety of reasons why a report might be screened out. In most cases screened-out
reports are those reports where the information provided does not constitute maltreatment of a
child or risk of maltreatment of a child. Additionally, when multiple reports are made about the
same maltreatment, the subsequent reports may be screened out. In Wisconsin, CPS agencies
are currently not required to investigate instances of abuse by noncaregivers, so those reports
may be screened out. In rare instances, cases may be screened out because there is insufcient
identiable information available. Finally, cases may be screened out because jurisdiction more
properly rests with another state.
There is no signicant difference in the number of referrals or screened-in referrals (reports)
between FFY 2022 and FFY 2021.
Children
A child is considered to be a victim when an allegation is substantiated. The NCANDS unsub-
stantiated maltreatment disposition includes instances where the allegation was unsubstantiated
for that child, or when critical sources of information cannot be found or accessed to determine
whether maltreatment as alleged occurred.
No changes were made to the policies regarding conducting investigations and assessments as a
result of the pandemic. Our state continued to conduct investigations and assessments through
face-to-face contact, as well as a combination of phone and video calls. All initial contact for
investigations and any contact necessary for ensuring children’s safety was expected to be
face-to-face. Workers continued to gather information per requirements laid out in the state’s
Initial Assessment Standards, Ongoing Services Standards, and Safety Intervention Standards.
DCF issued practice guidance for engaging families through virtual means, such as video calls,
for the purposes of information gathering and assessing during the pandemic.
Child Maltreatment 2022
Appendix d: State Commentary 296

Fatalities
The number of fatalities includes only those children who were reported as subjects of abuse
or neglect and the maltreatment allegation was substantiated. Only the Wisconsin Department
of Children and Families is involved in compiling information on child maltreatment fatalities,
and all fatalities are reported in the Child File.
Perpetrators
Details of the perpetrators is included for allegations in which the child was substantiated. The
NCANDS category “other” perpetrator relationship includes perpetrators who are not primary
or secondary caregivers to the child (such as non-caregivers) for example, another child or
peer of the child victim or a stranger. As mentioned previously, there are no substantiations in
AR cases, so the alleged perpetrators in AR cases will not be recorded as substantiated per-
petrators. Services, if needed, are established based on the assessment determination, not the
determination of a specic perpetrator.
Services
Wisconsin is currently not able to report prevention services. The state continues to support
data quality related to service documentation and ultimately to modify the NCANDS le to
incorporate services reporting for future data submissions.
Wisconsin (continued)
Child Maltreatment 2022
Appendix d: State Commentary 297

Wyoming
Contact Debra Hibbard Phone 307–777–5479
Title Deputy Administrator
Services Division
Email
Address Wyoming Department of Family Services
2300 Capitol Avenue
Cheyenne, WY 82002
General
Wyoming has three (3) types of responses to child protection referrals. There is an
Investigation Track, Assessment Track, and a Prevention Track. The Investigation Track is
assigned as described in the Level of Evidence section. Victims that have been substantiated
on unsubstantiated are identied and reported to NCANDS through the Investigation Track.
The Assessment Track gets assigned if the referral alleges abuse and /or neglect but does not
meet the criteria for the Investigation Track. The Prevention Track is assigned when there
is no allegation of abuse and/or neglect, but there are identied risk factors that indicate the
need for services to prevent abuse and/or neglect. Non-victims are identied and reported to
NCANDS through the assessment and Prevention Tracks. No changes were made to policy
or programs during the COVID pandemic. Procedures for eld staff were adjusted to allow
for discretion when conducting visits with children, foster families and biological families
through mechanisms other than in person visits. These decisions are being made on a case-
by-case basis, and in consultation with supervisors and managers based on assessed safety
risk and need.
Reports
Wyoming saw an increase in the number of referrals for abuse/neglect due to children return-
ing back to school after the COVID pandemic lessened in severity and youth were no longer
being conned in their homes due to COVID restrictions and the children were seen on a
more frequent basis for observation.
Children
Wyoming did not change policy related to investigations and assessments. Procedures for
the investigation and assessment process continued to be conducted with caution. However,
workers were able to enter homes on a more frequent basis to conduct investigations and
assessments. In FFY 2022 the state implemented a tracking mechanism in SACWIS that will
allow for reporting on IPSE. This was implemented in December 2022 and guidance was
provided for all staff. In FFY 2023 we have data available. For prior years we have manually
collected this data through review of all intakes for calendar years 2021 and 2022. In 2022,
132 children were included in reports to the Department as it pertained to prenatal substance
exposure.
Fatalities
Wyoming did not change any policies related to child fatality reviews. Wyoming has a major
injury and fatality review team that is comprised of the Department of Family Services,
the Wyoming Citizen Review Panel, the Wyoming Children’s Trust Fund, the Wyoming
Department of Health, the Wyoming Department of Corrections, the Wyoming Division
of Victim Services, the Wyoming Department of Education as well as members represent-
ing the disciplines of judges, mental health, local medical professionals and local law
enforcement.
Child Maltreatment 2022
Appendix d: State Commentary 298

Perpetrators
Wyoming utilizes a SACWIS that is incident based and does not have the ability to cat-
egorize incidents to see trends. Over the course of the last three years the department has
developed and implemented a special investigation unit that has one focus of facility related
maltreatment, which has included updated procedures and two dedicated investigators.
Services
Wyoming had a slight reduction in Services Responses as the Department was able to offer
other services to children and families through other federal COVID Funds to better meet
their needs.
Wyoming (continued)
Child Maltreatment 2022
Appendix d: State Commentary 299

